
Abstract
Post-traumatic cerebral infarction (PTCI) is a significant complication in polytrauma patients with traumatic brain injury (TBI). Identifying high-risk patients for early intervention is crucial. This study aims to investigate the independent risk factors for PTCI in polytrauma patients with TBI to establish and validate a prediction model. A retrospective analysis was conducted on 511 patients with TBI and multiple injuries admitted between January 2016 and July 2023. The patients were divided into groups based on whether they developed PTCI. Independent risk factors for PTCI were identified using univariable, Lasso, and multivariable logistic regression analysis. A nomogram was established to predict the risk factors for PTCI. The receiver operating characteristic (ROC) area under the curve (AUC), calibration curve, and decision curve analysis (DCA) were used to determine the predictive accuracy, discrimination, and clinical effectiveness of the nomogram, respectively. In addition, the Hosmer–Lemeshow test was used to assess the goodness-of-fit. Clinically significant associations were observed between PTCI and factors such as cerebral hernia, traumatic subarachnoid hemorrhage, basilar skull fracture, shock index, platelets, platelet–lymphocyte ratio (PLR), prothrombin time, international normalized ratio, D-dimer, albumin, injury severity score, and Glasgow coma score (all p < 0.05). These variables screened by Lasso regression were incorporated in multivariate logistic regression. They identified cerebral hernia, basilar skull fracture, PLR, D-dimer, and albumin as independent risk factors for PTCI (all p < 0.05). The analysis results were visually represented using a nomogram. The AUC of the prediction cohort was 0.9 [95% confidence interval (95% confidence intercal (CI)): 0.84, 0.97], and of the validation cohort was 0.87 (95% CI: 0.79, 0.96). The nomogram prediction model demonstrates excellent performance according to the ROC, calibration curve, and DCA, providing valuable insights for the early identification of high-risk PTCI patients.
Introduction
The rapid societal progress and increasing industrialization in China have led to a notable increase in construction and traffic accidents. Despite the implementation of enhanced protective measures, the incidence of polytrauma with traumatic brain injury (TBI) continues to rise. These patients typically present complex conditions, predisposing them to severe complications. Furthermore, critical illness, often linked with polytrauma and TBI, frequently results in poor prognoses with multiorgan dysfunction, further complicating treatment and worsening patient outcomes. 1,2 Post-traumatic cerebral infarction (PTCI) significantly impacts the course of polytrauma with TBI, affecting patient prognosis, survival, and quality of life and imposing a substantial financial burden on families. 3 Therefore, identifying clinical risk factors for PTCI in polytrauma patients with TBI can enhance diagnostic accuracy and improve patient outcomes. This retrospective study examines the factors associated with PTCI development in polytrauma patients with TBI by analyzing data from patients admitted to the Affiliated Hospital of Jiangsu University over 8 years (Fig. 1). The independent risk factors for PTCI in this population were identified by constructing a nomogram to establish a more reliable and robust model. This tool provides valuable guidance for screening high-risk populations following polytrauma with TBI, helping to improve diagnostic strategies and offering hope for better patient outcomes.
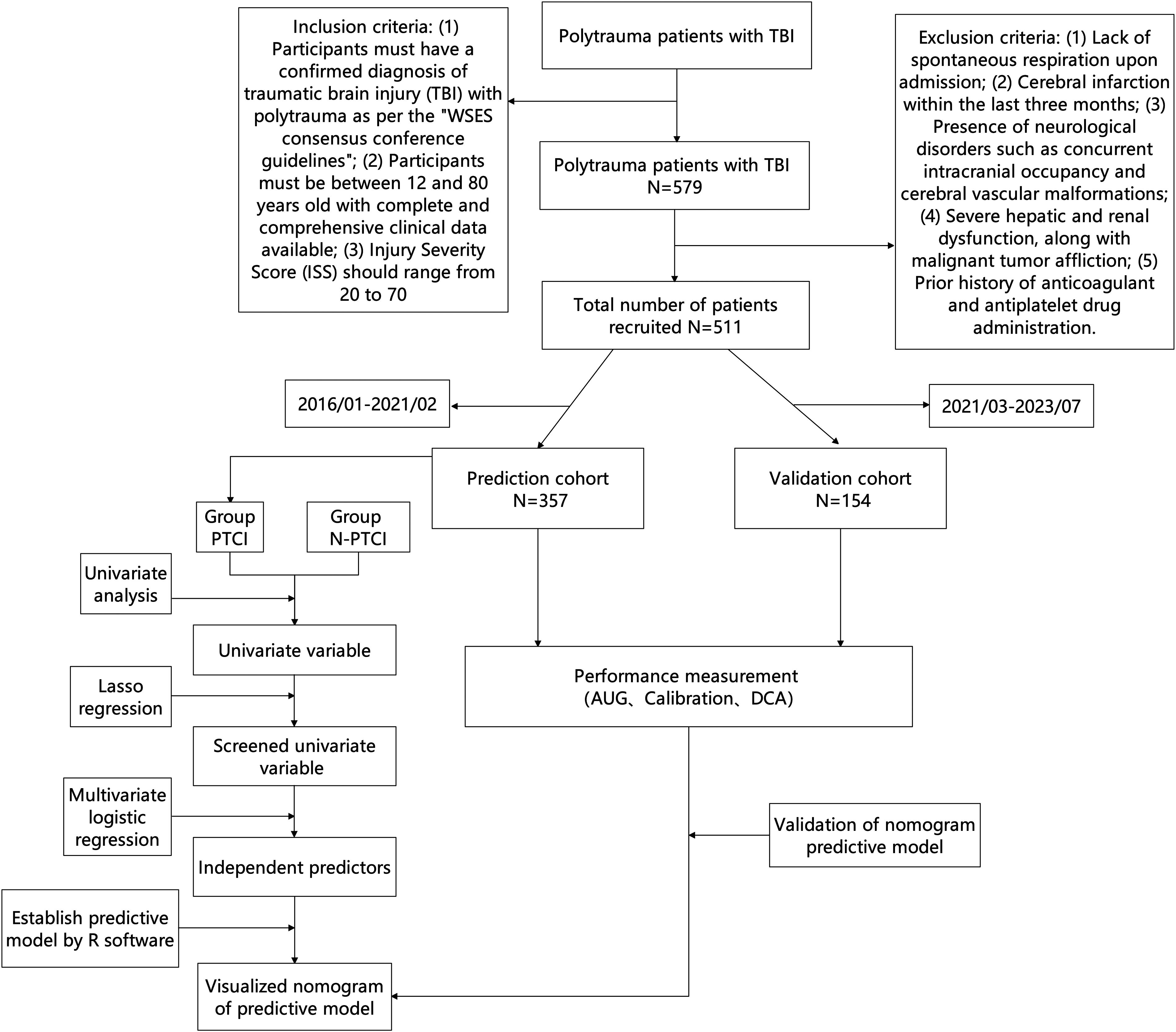
Study flow chart. PTCI, post-traumatic cerebral infarction; AUC, area under the curve; DCA, clinical decision curve analysis.
Materials and Methods
Data source
Between January 2016 and July 2023, 579 patients diagnosed with polytrauma and TBI were treated at the Affiliated Hospital of Jiangsu University. After screening, 511 patients were included in this study. Among these patients, 345 were male, and 166 were female. A total of 157 patients succumbed, while 354 survived. To develop the prediction model, 357 patients admitted between January 2016 and February 2021 were included as the prediction cohort, while 154 patients admitted between March 2021 and July 2023 comprised the validation cohort.
Inclusion and exclusion criteria
Inclusion criteria
(1) Participants must have a confirmed diagnosis of polytrauma with TBI as per the “WSES consensus conference guidelines.” 4 (2) Participants must be between 12 and 80 years old and have complete and comprehensive clinical data available. (3) The injury severity score (ISS) should range from 20 to 70.
Exclusion criteria
1. Lack of spontaneous respiration upon admission. 2. Cerebral infarction within the last three months. 3. Presence of neurological disorders such as concurrent intracranial occupancy and cerebral vascular malformations. 4. Severe hepatic and renal dysfunction, along with malignant tumor affliction. 5. History of anticoagulant and antiplatelet drug administration before participation.
Upon admission, the patients in the prediction cohort were divided into two groups based on the presence of traumatic cerebral infarction: the PTCI and the post-trauma without cerebral infarction (N-PTCI) group. The N-PTCI group consisted of 321 patients (218 males and 103 females) with a mean age of 57.6 ± 17.4 years. The PTCI group comprised 36 patients (25 males and 11 females) with a mean age of 56.5 ± 10.7 years. The Ethics Committee of Jiangbin Hospital Affiliated Jiangsu University granted ethical approval for this study (KY2024K0401).
Data collection
The review and analysis of medical records for each patient encompassed the following data: age, sex, past medical history, craniotomy, cerebral herniation, cerebral contusion, subdural hematoma (SDH), epidural hematoma (EDH), diffuse axonal injury (DAI), traumatic subarachnoid hemorrhage (tSAH), skull base fracture, model of trauma, shock indices, neutrophil/lymphocyte ratio (NLR), platelets, platelet–lymphocyte ratio (PLR), activated partial thromboplastin time (APTT), prothrombin time (PT), international normalized ratio (INR), D-dimer, blood lactate, albumin, total bilirubin (TBIL), blood urea nitrogen (BUN), serum creatinine (Scr), blood glucose (Glu), and mortality.
Clinical and imaging evaluation
Assessment of TBI and polytrauma: (1) Glasgow coma score (GCS); (2) ISS.
Auxiliary examinations: Upon admission, all patients had Computed tomography (CT) scans of the brain, cervical spine, chest, and abdomen to clarify the circumstances of the injury in the head or other organs. The CT scan was repeated within 24 or 12 h to determine whether there were any changes in the condition of their brain injuries and other injured organs. A third CT scan might be scheduled on the third day post-trauma. Follow-up brain CTs were performed at the discretion of the attending physicians. The ischemic lesion discovered during the first CT scan, which maintained a constant density during the follow-up CT scan, is considered an old infarction and was excluded from this analysis. New territorial cerebral infarctions (complete or incomplete) were observed in subsequent CT scans. The observations revealed well-defined, low-density lesions within the brain’s vascular territory, exhibiting distinct or indistinct margins. These lesions were associated with clinical symptoms aligning with established cerebral infarction diagnostic criteria. This finding indicates the emergence of new independent infarct lesions on CT responsible for symptoms manifesting after a delay. 5 Alternatively, there may be watershed cerebral infarctions. These cerebral infarctions are commonly diagnosed as PTCI (Fig. 2). We require that these low densities be detectable in CT scans 7 days after their discovery. Two skilled double-blinded neuroradiologists interpreted these radiographical images.

Computed tomography (CT) images of a patient with subdural hematoma within 14 days after admission.
Statistical analysis
The data analysis utilized SPSS 26.0 statistical software and R software (version 4.4.2). Categorical variables were depicted as the number of cases and percentage (%), and comparisons were made using the χ2 or Fisher’s exact test when appropriate. The normality of continuous data was tested using the Kolmogorov–Smirnov test. Normally distributed data were expressed as mean ± standard deviation (x ± s) and compared using the independent samples t-test. Nonnormally distributed data were presented as the median and interquartile range (M [Q1, Q3]) and compared using the Mann–Whitney U rank-sum test. Missing data were handled using the multiple value assignment (i.e., MICE) method. Data points exceeding 1.5 times the interquartile range were identified as outliers and treated as missing data.
Risk factors for PTCI in patients with TBI and polytrauma were identified using a stepwise forward inclusion multivariate logistic regression model. This model included variables showing a trend toward significance (p < 0.05) in univariate analyses and screening by Lasso regression. In addition, a nomogram was established based on the identified independent risk factors. The values on the predictive variable axis correspond to different points in the nomogram. The points of each predictor variable are added to get the total score. According to the established nomogram, the increased risk of PTCI in polytrauma patients with TBI can be inferred based on the higher total score. All patients were divided into a prediction cohort (n = 357) and a validation cohort (n = 154) in a 7:3 proportion according to the time of admission. Discrimination was evaluated by calculating the concordance index (C-index), which is generally considered to be equivalent to the area under the curve (AUC) of the receiver operating characteristic curve (ROC). The calibration curve was used to verify the consistency of the model. Clinical decision curve analysis (DCA) was a method to evaluate the clinical application value of the predictive model. In addition, the Hosmer–Lemeshow test was used to assess the goodness-of-fit of the predictive model, and p > 0.05 indicated that the model had a good goodness-of-fit.
Result
Univariate and Lasso regression analysis of PTCI in polytrauma patients with TBI
Our univariate analysis revealed significant associations between the following factors and PTCI in polytrauma patients with TBI (p < 0.05): cerebral herniation, tSAH, basilar skull fracture, shock index, platelet, PLR, PT, INR, D-dimer, albumin, ISS, and GCS. We detected no significant associations between the following factors and PTCI in polytrauma patients with TBI (all p > 0.05): age, sex, underlying disease including hypertension and diabetes, craniotomy, cerebral contusion, SDH, EDH, DAI, model of trauma, NLR, APTT, TBIL, blood lactic acid, BUN, Scr, and Glu (Table 1).
Univariate Logistic Analysis of PTCI in Polytrauma Patients with TBI
SDH, subdural hematoma; EDH, epidural hematoma; tSAH, traumatic subarachnoid hemorrhage; DAI, diffuse axonal injury; NLR, neutrophil/lymphocyte ratio; PLR, platelet–lymphocyte ratio; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; TBIL, total bilirubin; BUN, blood urea nitrogen; Scr, serum creatinine; Glu, blood glucose; GCS, Glasgow coma score; ISS, injury severity score; PTCI, post-traumatic cerebral infarction.
To avoid overfitting due to the large number of factors above and potential collinearity in the predictive model, screening the selected univariate variables using Lasso regression analysis was necessary. The optimal value was determined by cross-validation to identify the potential predictors. The results showed that the variables included in the multivariate logistic regression analysis were (p < 0.05) cerebral herniation, basilar skull fracture, shock index, PLR, D-dimer, and albumin (Table 2 and Fig. 3).

Lasso regression analysis of PTCI in polytrauma patients with TBI.
Lasso Regression of PTCI in Polytrauma Patients with TBI
PLR, platelet–lymphocyte ratio; PTCI, post-traumatic cerebral infarction.
Multivariate logistic analysis of PTCI in polytrauma patients with TBI
Multivariable logistic regression analysis identified the following independent predictors of PTCI in patients with TBI and polytrauma (p < 0.05): cerebral hernia [odds ratio (OR) = 11.33, 95% confidence interval (95% CI): 3.49, 36.81, p < 0.001], basilar skull fracture (OR = 6.05, 95% CI: 2.17, 16.88, p < 0.001), PLR (OR = 1.01, 95% CI 1.01, 1.02, p < 0.001), D-dimer (OR = 1.02, 95% CI: 1.01, 1.03, p < 0.001), and albumin (OR = 0.89, 95% CI: 0.83, 0.95, p < 0.001). After accounting for other potential influencing variables, these factors were independently associated with PTCI (Table 3).
Multivariate Analysis of the Predictive Value of PTCI in Polytrauma Patients with TBI
OR, odds ratio; CI, confidential interval; PLR, platelet–lymphocyte ratio; PTCI, post-traumatic cerebral infarction.
Establishment of a nomogram predictive model
Based on the results of multivariate logistic analysis, the predictive model was visualized as a nomogram using R software (Fig. 4). The predictive variables included in the nomogram were cerebral hernia, basilar skull fracture, PLR, D-dimer, and albumin. Each patient’s variables need to be scored, and a vertical line is drawn from the corresponding value to the points scale to determine the total score and assess the risk of PTCI in polytrauma patients with TBI. A higher total score indicates a greater risk of PTCI.
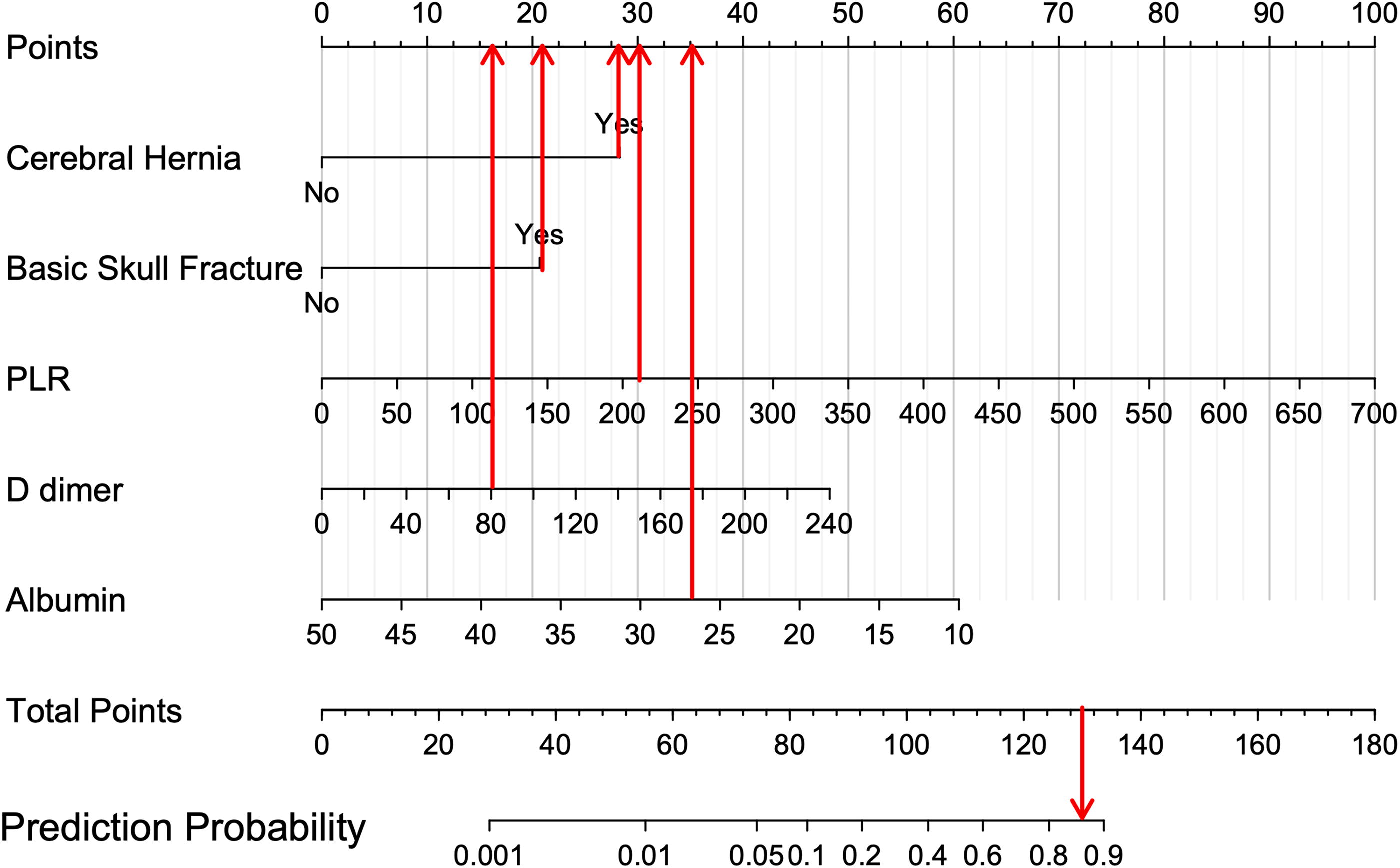
A nomogram indicates the risk of PTCI in polytrauma patients with TBI. PLR, platelet–lymphocyte ratio; TBI, traumatic brain injury; PTCI, post-traumatic cerebral infarction.
Validation of nomogram predictive model
The ROC analysis of the predictive model yielded AUC values of 0.90 (95% CI: 0.84, 0.97) and 0.87 (95% CI: 0.79, 0.96) in the prediction and validation cohorts, respectively, indicating that the predictive model demonstrated excellent discrimination in both cohorts (Fig. 5A and B). The calibration curves of the prediction and validation cohorts aligned closely with the actual observation, demonstrating that the model had strong consistency (Fig. 5C and D). In addition, DCA showed that the threshold probability of the nomogram in the prediction cohort was 3∼99%, and the net benefit >0. In the validation cohort, the threshold probability of the nomogram was 1∼99%, and the net benefit >0, suggesting that the nomogram prediction model had excellent clinical application value for predicting the risk of PTCI in polytrauma patients with TBI (Fig. 5E and F). According to the Hosmer–Lemeshow test, χ2 = 11.98, p = 0.152 in the prediction cohort, and χ2 = 15.70, p = 0.257 in the validation cohort, which means the predictive model exhibited great goodness-of-fit in both cohorts.
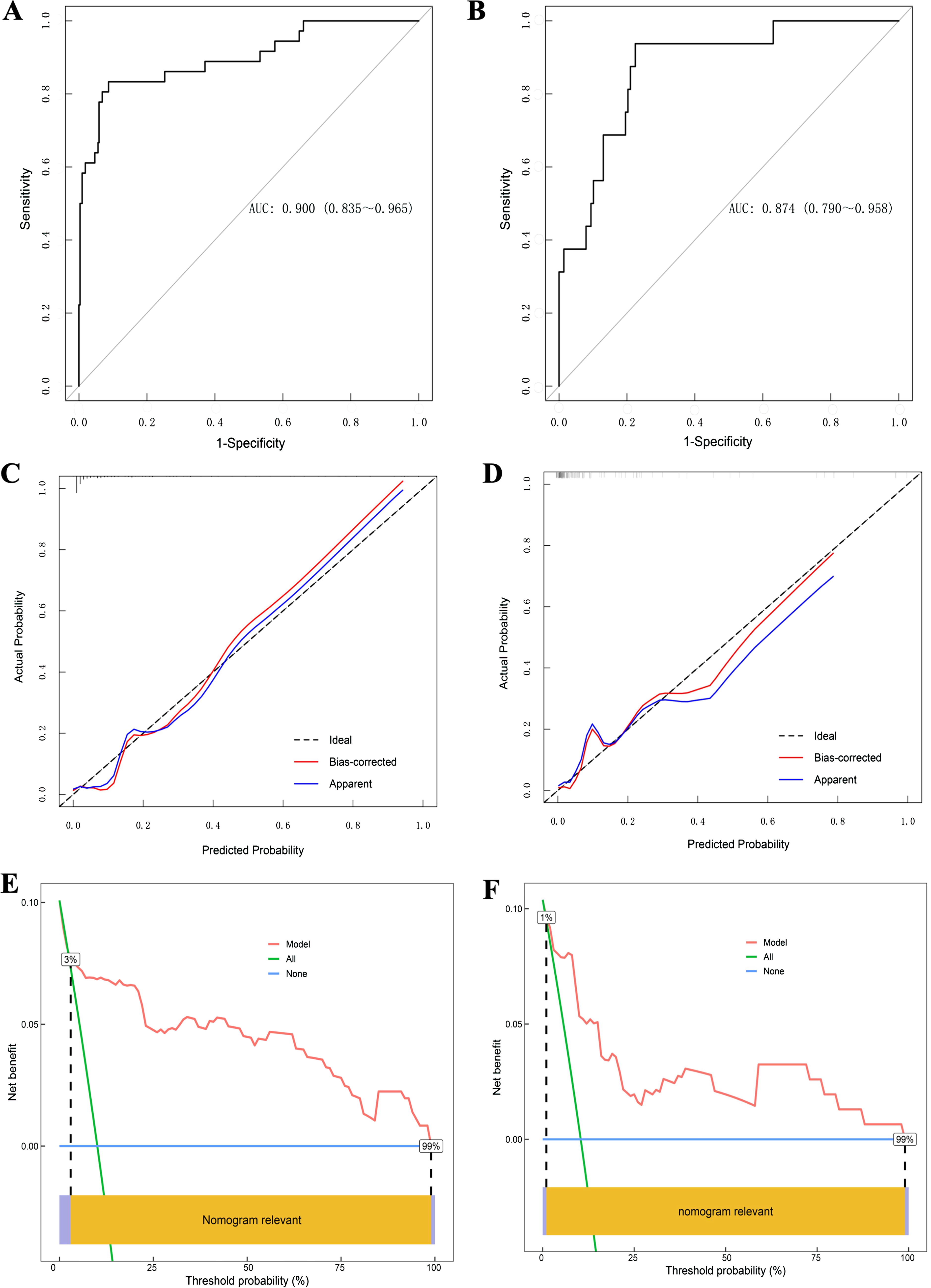
The ROC curves, calibration curve, and DCA of the nomogram for the risk of PTCI in polytrauma patients with TBI.
Discussion
Patients with TBI and polytrauma face severe injuries, impaired consciousness, rapid disease progression, and a high burden of complications. 6 These factors will increase the risk of PTCI. The development of PTCI can exacerbate the intracranial condition, leading to a poor prognosis and increased mortality. This study is significant as it aims to identify clinical risk factors associated with PTCI in polytrauma patients with TBI, with the goal of establishing a protective model that offers excellent predictability and clinical application.
Our investigation has revealed a 10.08% (36/357) prevalence of cerebral infarction in patients with TBI and polytrauma in the protection cohort. This finding aligns with Tawil et al.’s reported 8% prevalence of PTCI in severe TBI patients. 7 The PTCI group exhibited a higher mortality rate (36.11%) compared with the non-PTCI group (30.53%) in the protection cohort, indicating an elevated risk of death associated with PTCI. Univariate analysis shows no significant differences in patients with and without PTCI following polytrauma and TBI regarding sex, which aligns with previous studies, 8,9 indicating that sex does not affect the occurrence of PTCI after trauma. Our comparative analysis in this study identified various independent risk factors associated with an increased incidence of cerebral infarction in patients with TBI and polytrauma (p < 0.05). These risk factors encompass cerebral herniation, basilar skull fracture, PLR, D-dimer, and albumin, all of which may contribute to the development of cerebral infarction after TBI with polytrauma.
Concurrent extracranial injuries can exacerbate cerebral hypoperfusion and coagulopathy in patients with TBI. Previous studies have established a correlation between coagulopathy and an increased risk of cerebral infarction. 10 D-dimer, a degradation product of fibrin cross-linking, is a crucial clinical indicator for venous thromboembolism following TBI, 11 reinforcing the practical implications of our research.
Watanabe et al. proposed that elevated D-dimer levels in TBI patients with severe extracranial injuries significantly contribute to the development of PTCI. 12 Similarly, Chen et al. demonstrated the potential of abnormal PT and D-dimer values in predicting the occurrence of early PTCI. 13 Our analysis unveiled a significant association between the co-occurrence of ischemic stroke and polytrauma in patients with TBI. Notably, abnormal D-dimer levels emerged as an independent predictor of this serious complication, aligning with prior observations in the literature. Severe trauma has the potential to disrupt the hemostasis between thrombosis and fibrinolysis within the cerebral vasculature. This disruption triggers a pathological cascade, resulting in the insidious accumulation of fibrin deposits within the vasculature. This process depletes coagulation factors and triggers the formation of small blood clots, known as microthrombi, by activating the coagulation mechanism and inhibiting the body’s natural anticoagulation cascade. 14 Elevated D-dimer levels, a byproduct of fibrinolysis, signify an increased risk of ischemic stroke. Furthermore, D-dimer shows promise as a biomarker for trauma-induced brain tissue damage and an early predictor of ischemic stroke, offering hope for improved patient outcomes.
Albumin, an essential nutrient synthesized by hepatocytes, possesses antioxidants, anti-inflammatory, and antithrombotic properties. 15 Oxidative stress, inflammatory injury, and thrombosis are key factors involved in the development of cerebral infarction. Patients with cerebral infarction often present with hypoproteinemia. Zhao et al. reported significantly decreased albumin levels in patients with cerebral infarction who did not survive, 16 highlighting the critical role of albumin in the progression of this condition. Similarly, our study identified a link between decreased albumin levels and an elevated risk of ischemic stroke in polytrauma patients with TBI. Reduced serum albumin has been observed in patients with TBI 17 and polytrauma, 18 potentially triggered by traumatic hemorrhage. To counteract the inflammatory cascades induced by trauma, albumin promotes the synthesis of anti-inflammatory molecules, which are subsequently consumed, exacerbating inflammatory damage and oxidative stress.
In addition, albumin reduces blood viscosity by lowering multiple coagulation factors, preventing platelet aggregation, and inhibiting the formation of thrombosis. Its antithrombotic properties may be key to its protective role against cerebral infarction. Furthermore, as a vital component of plasma colloid osmotic pressure, a decrease in albumin leads to insufficient intravascular osmotic pressure, resulting in fluid migration from blood vessels to the interstitium. This fluid shift can worsen cerebral edema and potentially precipitate brain herniation. Therefore, decreased albumin levels serve as a critical risk factor for the early prediction of PTCI in polytrauma patients with TBI.
Patients with TBI, polytrauma, and a concurrent skull base fracture demonstrate heightened susceptibility to PTCI. This increased vulnerability likely results from disrupting blood vessels at the skull base during the fracture, compromising cerebral perfusion due to vessel compression from bony fragments. Moreover, the trauma may compromise the vessels’ endothelium (inner lining), fostering thrombus formation and further constraining cerebral tissue perfusion, ultimately contributing to PTCI progression. 19
Following trauma, the host immune response can be altered, 20 –22 potentially resulting in a post-traumatic inflammatory state believed to contribute to the pathogenesis of ischemic stroke. Our study demonstrated markedly elevated PLR levels in the PTCI group compared with the control group, consistent with previous findings by Sung et al., indicating a correlation between inflammatory markers and the onset of cerebral infarction. 23 PLR has emerged as a clinically relevant biomarker for assessing the severity of the inflammatory response. Previous research has established its predictive value in gauging inflammatory responses in conditions such as stroke and cancer. 24 Moreover, there is emerging evidence of a plausible link between altered PLR values and acute ischemic stroke in young patients, highlighting the potential utility of PLR in early screening. 25 However, the role of PLR in cerebral infarction with concomitant multiple injuries and TBI remains unexplored. This study represents an initial investigation into PLR as an independent risk factor for PTCI development in this patient population.
Furthermore, the evidence suggests a potential, albeit undefined, role for PLR in the pathophysiology of PTCI. Substantiating these findings, Altintas et al. have reported an association between elevated PLR and both the volume of cerebral infarction volume and poor prognosis. 26 Moreover, Lee et al. have illustrated the superior predictive ability of PLR prognosticating outcomes following endovascular treatment of acute ischemic stroke. 27 Further elucidation is required to understand the precise mechanism through which PLR signifies the occurrence of cerebral infarction in TBI with multiple injuries. TBI is known to elicit robust inflammatory responses. 2,28,29 This sequela is characterized by lymphocytopenia, accompanied by an increase in platelets, which occurs concomitantly with the continuous release of inflammatory factors. 30 The interplay between inflammatory cytokines, platelets, and lymphocytes contributes to a significant rise in PLR, potentially contributing to a higher incidence of PTCI. Lukito et al. did not discern a substantial association between PLR and cerebral infarction. 31 Such disparities from prior findings may be ascribed to variances in the patient population and the variables under investigation. Despite inconsistencies in past research findings, the potential for PLR, as an inflammatory marker, to evolve as a more refined biomarker for predicting the development of neurotraumatic pathologies remains.
Our multifactorial analysis indicates that cerebral herniation represents an independent risk factor for ischemic stroke in the context of TBI with polytrauma. A common cause of PTCI is the mechanical compression or displacement of the large intracranial artery, 32 which our research has shown to correlate with changes in PLR and the activation of an inflammatory response in trauma patients. The subsequent release of inflammatory cytokines increases vascular permeability, resulting in the leakage of plasma components and edema. 33,34 Vasogenic cerebral edema exacerbates brain tissue damage and may elevate intracranial pressure, precipitating cerebral herniation, 35 which, in turn, constricts local cerebral blood flow and amplifies the risk of PTCI. Moreover, heightened intracranial pressure can reduce cerebral blood volume, predisposing individuals to the development of PTCI.
As this study is retrospective, it is crucial to acknowledge the limitations associated with potential biases in patient selection and data collection processes. Vascular imaging was not performed to diagnose patients with PTCI in this retrospective study. However, we plan to include it in the future, as it may significantly improve the diagnosis of PTCI. The absence of data on patients’ body weight and medication histories, as well as the relatively small sample size in the PTCI group, highlights the need for further validation through an extensive, multicenter, prospective investigation, which could significantly impact future research in this field.
Conclusion
Our findings, which highlight the independent risk factors of cerebral herniation, basilar skull fracture, PLR levels, D-dimer levels, and albumin levels for cerebral infarction in polytrauma patients with TBI, have significant potential. The predictive model constructed based on the above variables exhibits excellent predictive performance. This knowledge, along with new potential therapeutic strategies, 27,36,37 can empower clinicians to make precise, early predictions and interventions.
Transparency, rigor, and reproducibility statement
A total of 511 patients diagnosed with polytrauma and TBI were admitted to Jiangsu University Affiliated Jiangbin Hospital between January 2016 and July 2023. Patients were divided into groups based on whether they developed PTCI within 7 days of admission. The sample sizes of 459 and 52 patients in each group were not preplanned but were based on the number of patients meeting the inclusion criteria. The key inclusion criteria and outcome evaluations are established standards. The patients’ data were collected by team members blinded to relevant characteristics. The model developed in this study demonstrated excellent predictive capabilities. As reported in the text, missing data were handled using the multiple imputation by chained equations (MICE) method. A small proportion of data was missing, specifically concerning the shock index and TBIL; these missing values were classified as missing completely at random, accounting for less than 2% of the total dataset. To address the issue of multivariate missing data, we employed the MICE method utilizing R software, whereby a distinct model was used to impute each variable exhibiting incompleteness. Consequently, we generated a complete dataset that included all the missing values from the initial dataset. Each imputed dataset underwent analysis, and the results were subsequently summarized. This study adhered to the Standards for Reporting of Diagnostic Accuracy Studies, STARD.
Footnotes
Authors’ Contributions
J.M. and X.Q. contributed equally. J.M. and X.Q. designed the study and drafted the article. Z.M., J.L., L.Z., and R.Z. collected and analyzed the data. Y.R.-K., L.L., N.L., Q.B., J.Z., and C.J. prepared figures and revised the article. X.M., S.G., J.W., and J.M.W. reviewed and revised the article. All authors approved the final article.
Author Disclosure Statement
None declared.
Funding Information
This study was supported by the Youth Project of the National Natural Science Foundation of China (82101602).