
Abstract
Traumatic brain injury (TBI) affects millions globally each year, with mild TBI comprising about 75% of cases. While most mild TBI symptoms are resolved within 3 months, some patients experience persistent issues. This study aimed to identify underlying mechanisms contributing to decrements in fluid cognitive abilities in chronic (>6 months) mild-to-moderate TBI. Specifically, the study focused on the relationships between cognitive performance, white matter integrity, TBI-related symptoms, and blood biomarkers, which are thought to be indicative of biological processes including neuronal injury (neurofilament light [NF-L], neurofilament heavy, ubiquitin C-terminal hydrolase-L1), vascular injury (vascular endothelial growth factor A), glial injury (glial fibrillary acidic protein [GFAP]), neurodegeneration (tau, phosphorylated-tau), immune response (GFAP immunoglobulin G), and inflammation (tumor necrosis factor-α, interleukin [IL]-2, IL-4, IL-6, IL-8, IL-10, interferon-γ, and macrophage inflammatory protein-1α). The final study sample included 57 participants (42 males, 15 females) aged 19–59 with a history of chronic, remote mild-to-moderate TBI. Participants underwent cognitive and behavioral testing, neuroimaging, and a blood draw. Diffusion-weighted magnetic resonance imaging was used to assess white matter integrity in tracts connecting frontal and parietal regions with fractional anisotropy utilized as the metric. Blood samples were analyzed for TBI-related biomarkers. The study found that higher fluid cognition scores were associated with higher white matter integrity in frontal–parietal networks, fewer reported TBI-related symptoms, and mixed biomarker and cytokine levels. Inflammatory processes were linked to lower fractional anisotropy in white matter pathways, more reported symptoms, and increased biomarkers of injury. Higher white matter integrity was also associated with fewer reported neurobehavioral symptoms. The findings provide evidence for a complex interplay of ongoing neuroinflammatory processes, white matter integrity, symptomology, and cognitive function in chronic mild-to-moderate TBI. The results underscore the importance of considering both structural brain changes and systemic responses in understanding the long-term effects of TBI. The observed correlations between cognitive deficits, white matter disruptions, and biomarker profiles suggest potential avenues for targeted interventions aimed at mitigating these effects in TBI patients.
Introduction
Traumatic brain injury (TBI) affects 69 million people annually. 1 –5 Approximately 75% of cases are categorized as mild (mTBI) based on presenting characteristics such as loss of consciousness, with most seeing apparent symptom resolution within 3 months. 5 –7 However, some patients report persistent physical, emotional, and cognitive symptoms. 8 Despite their prevalence, the mechanisms underlying ongoing symptoms are not well understood. Furthermore, addressing and treating TBI has proven challenging due to the heterogeneity of injuries and the delay between injury and clinical presentation. It is often unclear what symptoms, brain changes, and physiological responses are due to TBI, especially over time and age.
Attributing changes in neurobehavioral function to a remote TBI is challenging, but it is thought that long-term effects may result from a cascade of biological alterations triggered by the primary head injury. These processes, referred to as “secondary injury,” include microglial and astrocytic activation, neuroinflammation, axonal degeneration, glutamate excitotoxicity, altered cerebral blood flow, vascular injury, blood–brain barrier (BBB) disruption, and neurodegeneration. 9 –13 Dysregulation of such responses can exacerbate acute injury and contribute to chronic neurocognitive and neuropsychiatric effects. Additional injury may also occur from comorbidities including post-traumatic stress disorder (PTSD), sleep disruption, and chronic stress; however, the mechanisms underlying these secondary injury sources and sequelae remain poorly understood, necessitating investigation of potential biological markers that may provide insight into these processes. 14 –16
Magnetic resonance imaging (MRI) techniques such as diffusion-weighted imaging (DWI) have demonstrated that white matter injuries may be associated with neurobehavioral outcomes in mTBI. 9,17,18 Chronically, previous work has reported an accelerated loss of white matter after moderate and severe TBI compared with healthy controls. 17,19,20 Additionally, the existing literature on white matter injury in the chronic phase suggests that axonal injury increases the risk of neurodegeneration which persists for many years following initial injury and may lead to disease. 20 –22 Animal models have implicated a number of potential mechanisms for this chronic degeneration, including the development of progressive proteinopathies through axonal swelling and bulb formation, amyloid precursor protein buildup, axonal damage-induced tau dissociation from microtubules, or propagation of transmissible tau proteins from the site of injury. 22 –25
Novel blood biomarkers, including glial fibrillary acidic protein (GFAP), neurofilament light (NF-L), neurofilament heavy (NF-H), ubiquitin C-terminal hydrolase-L1 (UCH-L1), and tau (or phosphorylated tau [P-tau]) have shown potential as indicators of TBI pathophysiological events, summarized in Table 1. 20,26,27 These cell-type-specific proteins are released into biofluids following injury. 27 GFAP is recognized as a marker of glial injury, while NF-L, NF-H, NF-H, and UCH-L1 are indicators of axonal injury. Tau and P-tau may indicate neurodegeneration, and immunoglobulins are understood to represent immune response. 27 Elevations in such biomarkers can provide mechanistic and temporal insight into white matter injury and chronic TBI.
Sample Demographics
AOC, alteration of consciousness; LOC, loss of consciousness; TBI, traumatic brain injury.
Neuroinflammation plays a pivotal role in both acute and chronic phases of TBI and serves as a key contributor to sustained damage and a potential therapeutic target. 10,28,29 While neuroinflammation initially functions to repair damaged cells and prevent the passage of invasive pathogens into the brain, sustained inflammation has been linked to white matter degradation and neurodegeneration. 10,28,30,31 An upregulation of proinflammatory cytokines (tumor necrosis factor-α [TNFα], interleukin [IL]-2, IL-6, IL-8, interferon-γ [IFNγ], and macrophage inflammatory protein-1α [MIP-1α]) is observed acutely after injury, accompanied by a regulatory rise in anti-inflammatory cytokine levels (IL-4 and IL-10). Neuroinflammatory processes have been detected in individuals up to 17 years after the initial injury, even after a single incidence of moderate or severe TBI. 32 However, the order of events remains unclear, even in animal models. 22,31
The release of cytokines during inflammation leads to the activation of an immune response, involving a complex interplay of cells and signaling molecules. Microglia and astrocytes are rapidly activated following injury, contributing to the inflammatory milieu and formation of glial scars, which can impede axonal regeneration and contribute to chronic neuroinflammation. 33,34 The BBB is often compromised in TBI, allowing peripheral immune cells to infiltrate the brain and exacerbate the inflammatory response. 23 Of particular mechanistic interest in TBI are immunoglobulins or autoantibodies to cerebral proteins. The response to TBI consists of an immediate, short-lived increase in immunoglobulin M (IgM), followed by sustained production of immunoglobulin G (IgG), which has been detected even years after injury. 35,36 Following TBI, cognitive nervous system (CNS)-specific proteins such as GFAP are released into the bloodstream, where it can serve as an autoantigen. 36 Subsequently, increased GFAP-specific autoantibodies (i.e., IgM and IgM) may indicate a breach of the BBB and an autoimmune response against brain tissues. 35 –38 It is unclear whether autoantibodies play a protective or pathogenic role in the body, and the mechanistic effects of GFAP, IgM, and IgG remain uncertain. 36
Furthermore, the effects of TBI have been identified at many levels of vasculature in all severities of TBI. Changes in cerebral blood flow, micro bleeding, edema formation, and BBB disruption can have detrimental effects. 39 Vascular endothelial growth factor A (VEGF-A), a potent mediator of angiogenesis and vascular permeability, plays a significant role in the regulation of the BBB. In the context of TBI, elevated levels of VEGF-A can disrupt BBB integrity, leading to increased permeability, resulting in increased risk of infection, influx of toxins, immune cells, and other circulating factors, elevated intracranial pressure, and ultimately increased neuronal death. 40,41 Disruption of the BBB is a critical event in the cascade of secondary injury processes following TBI and may contribute to chronic TBI.
The complexities of TBI are profound, with even mild injuries leading to persistent symptoms and residual sequelae. Previous research has highlighted decrements in fluid abilities, which encompass reasoning, attention, and memory abilities, to persist beyond 3 months postinjury, associating these decrements with alterations in neural structure and function related to aging or injury. 42 –49 This domain of cognition may be particularly susceptible to the effects of TBI due to its reliance on multiple brain regions. 43,46,47 Neuroimaging studies have shown that a network of frontal and parietal regions supports the neural basis of intelligence. 47,50 –62 However, it is unclear how fluid ability is impacted long-term in patients with mTBI, and whether known physiological processes of primary and secondary injuries relate to function. Such relationships may highlight vulnerabilities to chronic difficulties or unidentified issues contributing to poorer recovery trajectories. Efforts to identify biomarkers for TBI classification and patient outcomes have faced limitations such as inconclusive findings, unreliable results, or focus on single biomarkers, leaving a notable gap in the literature. The present study aims to address this gap by not only evaluating the individual relationships between biomarkers and cognitive performance but also providing a dynamic analysis of the complexities that may exist between inflammatory, immune, vascular mechanisms, structural brain differences, and symptom complaints.
Specifically, the study sought to delineate underlying mechanisms contributing to decrements in fluid abilities in those with chronic mild-to-moderate TBI. We hypothesized that lower fluid cognition scores would be associated with more reported TBI-related symptoms (i.e., vestibular, somatosensory, cognitive, and affective), disruption of frontal–parietal white matter tracts, and increased levels of blood biomarkers of neuronal injury, vascular injury, glial injury, neurodegeneration, immune response, and inflammation. We examined the relationships between physiological indicators to better understand the systemic pathological processes occurring in chronic TBI. We anticipated that reports of more TBI-related symptoms would be associated with disruptions in long white matter tracts, and elevated levels of blood-based biomarkers of inflammation, neurodegenerative, neuroimmune, and vascular functions. Additionally, we proposed that compromised integrity of white matter in specific neural pathways would align with similar changes in biomarkers and cytokines. Moreover, we determined the role of TBI burden history in fluid cognition deficits, symptom severity, and biomarker and inflammatory profiles. We hypothesized that a greater TBI burden would be associated with lower fluid cognition, greater symptom reports, lower white matter integrity, and elevated levels of blood-based biomarkers.
Materials and Methods
Participants
A total of 73 veterans and civilians (53 males, 17 females) aged 18–60 years, with a history of chronic, remote mild-to-moderate TBI were recruited from the North Florida/South Georgia Department of Veterans Affairs Medical Center and the surrounding community. Exclusion criteria included severe neurological conditions (e.g., large vessel stroke, hydrocephalus, and unrelated seizures), autoimmune disease (controlled asthma/allergies acceptable), uncorrected sensory deficits, severe medical diseases (e.g., liver disease, severe heart disease, and heart attack), severe psychiatric conditions (e.g., schizophrenia), recent drug use, and MRI contraindications. Demographic, medical, and psychiatric history, as well as TBI history and related symptoms, were gathered using a structured interview and self-report questionnaires, and the NIH Toolbox (NIH-TB) cognitive battery provided fluid cognition scores. TBI diagnosis was based on United States Department of Veterans Affairs (VA) and Department of Defense (DoD) guidelines, supplemented by the Ohio State University TBI Identification Method Short Form and medical record review. The University of Florida (UF) institutional review board (IRB of record for VA) approved this study (IRB # 201801923). Participants provided written informed consent and were compensated for their participation.
Neuroimaging acquisition and processing
Imaging was conducted at the Advanced Magnetic Resonance Imaging and Spectroscopy Facility at the McKnight Brain Institute on the UF campus in Gainesville, FL using a 3T Siemen’s Prisma scanner (Siemens USA, Washington, DC) with a 64-channel head coil. Participants wore earplugs to counteract the adverse effects of noise and a squeeze ball to communicate with the MRI technician in case of emergency. Foam padding was used to minimize head motion. An MPRAGE T1-weighted anatomical image (magnetization prepared gradient echo, sagittal field of view = 256 mm, 256 × 256 matrix, slice thickness = 1.00 mm, repetition time/echo time (TR/TE) = 2.26 ms) was acquired for coregistration.
Diffusion-weighted MRI (dMRI; TE/TR = 89/4000 ms, 2.0 mm3, b < 3000, 9 shells, 180 directions) and T1-weighted images (TE/TR = 2.26/1800 ms, 1.0 mm3, fractional anisotropy [FA] = 8°) were collected. Anatomical reconstruction was performed on each participant’s T1-weighted image using FreeSurfer software (v7.2) to obtain a cortical parcellation and subcortical segmentation. 63 dMRI were coregistered to T1-weighted images and corrected for subject motion, eddy current distortion, and susceptibility-induced distortion, in the Functional Magnetic Resonance Imaging of the Brain (FMRIB) Software Library (FSL 6.0.6) with reverse phase-encoded field maps.
Diffusion tractography was performed using FreeSurfer’s (v7.2) TRActs Constrained by UnderLying Anatomy (TRACULA) tool, which provides an automated probabilistic reconstruction of white matter pathways from each participant’s DWI data. 64 This reconstruction approach has several advantages when compared with other DWI analytic methods (e.g., tract-based spatial statistics), including measuring white matter integrity within an individual’s native brain space, preserving individual differences, and allowing for reconstruction of major white matter tracts, providing more anatomical specificity. 65 –69 FA served as the metric for white matter integrity. Regions of interest included the dorsal cingulum bundle (CBD) and superior longitudinal fasciculus (SLF) 1, 2, and 3, which connect frontal and parietal regions. Left and right hemispheric FA values were averaged together due to being highly correlated (Fig. 1).
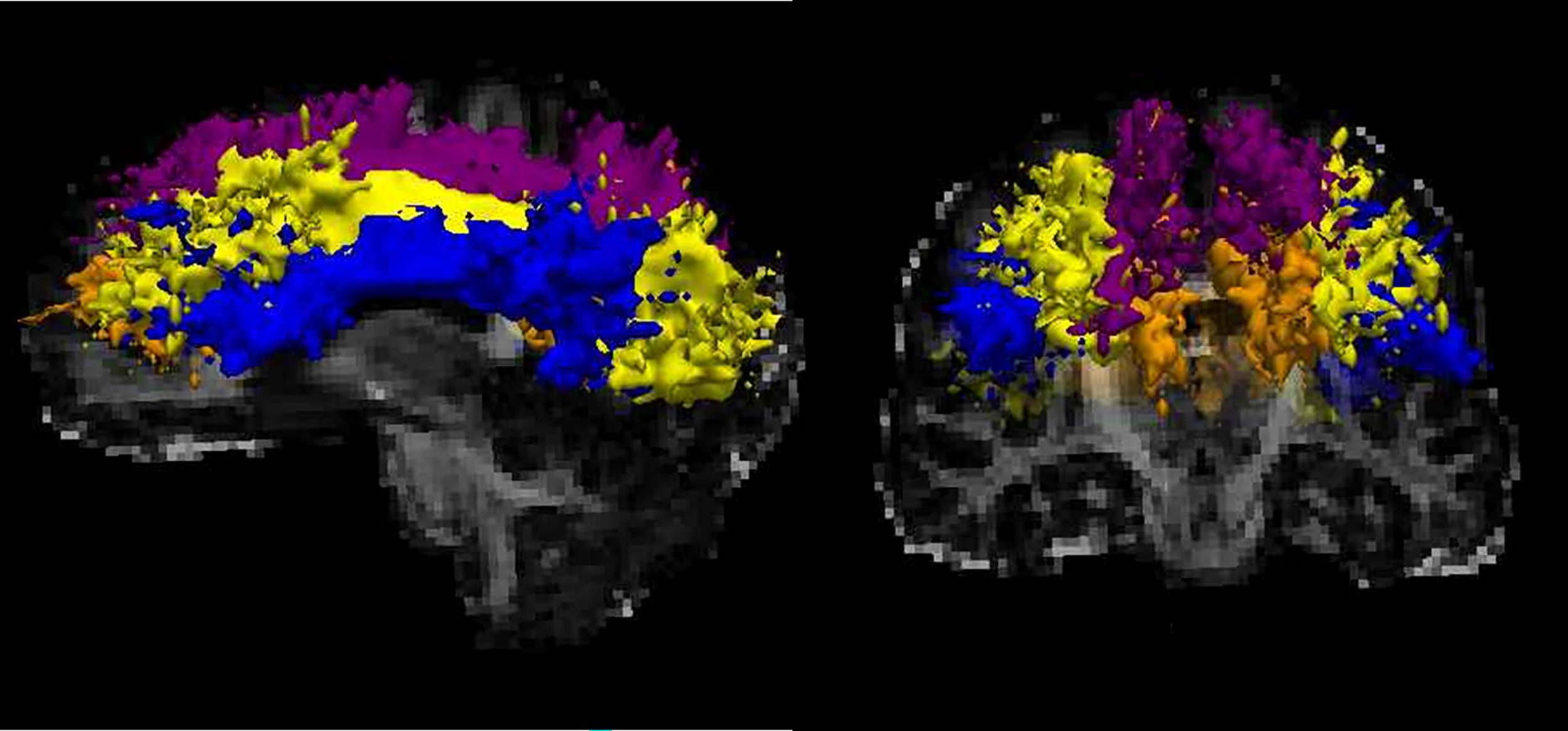
White matter pathways were visualized in FreeView using the diffusion tensor imaging (DTI) map and atlas created from FreeSurfer v 7.3.2. Sagittal (left) and coronal (right) brain views display the pathways of interest, including the SLF 1 (purple), SLF 2 (yellow), SLF 3 (blue), and CBD (orange). CBD, dorsal cingulum bundle; SLF, superior longitudinal fasciculus.
Serum biomarker collection and processing
A certified phlebotomist collected 30–45 mL of blood, and a variety of common assay platforms (e.g., enzyme-linked immunosorbent assay [ELISA]) and contemporary, highly sensitive platforms (Quanterix SIMOA, RCA-SOFIA) were selected for use. GFAP, UCH-L1, NF-L, tau, and NF-H were analyzed using an ultrasensitive immunoassay (Quanterix Single Molecule Arrays [SIMOA]-based Human Neurology 4-Plex B assay). VEGF-A was assayed using the MesoScale Discovery U-PLEX Human VEGF-A Assay. P-tau was assessed with the highly sensitive Rolling Circle Amplification-Surround Optical Fiber Immunoassay (RCA-SOFIA) platform. GFAP-specific autoantibodies (IgG/IgM) were quantified using an autoantibody direct ELISA assay. Assays followed standardized protocols to ensure precision and reproducibility.
Inflammatory marker bead array
Using serum samples, inflammatory biomarkers were assayed with Luminex™ bead array assays (Millipore, Billerica, Massachusetts). The Human High Sensitivity T-cell Magnetic Bead Panel included IL-10, IL-1β, IL-2, IL-4, IL-6, IL-8, MIP-1α, TNF-α, and IFN-γ. Miniaturization through the Curiox platform (Curiox Biosystems, Woburn, Massachusetts) was utilized to conserve biosample volume. The multiplex assays used microsphere technology, which consists of tagging assay beads with several fluorescent-labeled markers and analyzing the binding of each protein with a fluorescence detection laser optic system.
After receiving raw data from the Luminex facility, a “trimmed means analysis” approach was applied to eliminate outlier values. A standard curve was generated and applied to generate sample concentrations from the trimmed mean FI measurements of the unknowns. Outlier values that were 5 × interquartile range (IQR) below Q1 or 5 × IQR above Q3 for each biomarker were removed. Each plate was then “aligned” to the best-performing plate (determined using expected and observed concentrations of the standards and intraplate coefficient of variation percentages [CV] between duplicate samples) using linear indexing equations derived from interplate control samples (n = 10). Rerun samples (n = 30) were strategically placed across multiple runs to be used as interrun controls to generate linear indexing equations and aggregate data across assay runs. Intra- and interplate CV percentages were evaluated before and after data processing to assess assay performance.
Cognitive and behavioral data collection
Fluid cognition was assessed with the NIH-TB, incorporating comprehensive neuropsychological tests assessing fluid and crystallized cognition. The fluid composite score is calculated by averaging the T-scores from the Dimensional Change Card Sort Test, the Flanker Inhibitory Control and Attention Test, the Picture Sequence Memory Test, the List Sorting Working Memory Test, and the Pattern Comparison Processing Speed Test. 70
TBI-related symptoms were assessed using the Neurobehavioral Symptom Inventory (NSI), designated by the DoD as the standard assessment tool for evaluating neurobehavioral symptoms post-TBI in Military Health System TBI clinics. 71 This 22-item self-report measure contains responses ranging from “0” to “5,” indicating the presence of persistent symptoms. For scoring, responses of “0” or “1” were recoded as “0,” and recoded scores were grouped into four symptom-type subscales: Vestibular, Somatosensory, Cognitive, and Affective per literature-based recommendations. 72 This four-factor approach excludes two items—loss of appetite and hearing difficulties—that do not load onto latent factors. 72,73
TBI burden score
The burden of cumulative TBI was quantified using a TBI burden score derived using principal component analysis (PCA). The original variables included a number of TBIs (1, 2, 3, 4+), instances of alteration of consciousness ([AOC]; 1, 2, 3, 4+), and instances of loss of consciousness ([LOC]; 1, 2, 3, 4+). These ordinal variables were recoded into binary indicator variables for each count level (e.g., “TBI 1,” “TBI 2,” “TBI 3,” “TBI 4”). For instance, a participant with two TBIs would be represented by the indicator vector (1, 1, 0, 0). This approach was similarly applied to AOC and LOC, yielding 12 distinct binary input variables: TBI 1–4, AOC 1–4, and LOC 1–4.
This transformation allowed PCA to capture the cumulative effects of increasing instances of TBI, AOC, and LOC. The PCA identified the best linear combinations of these indicator variables, known as principal components (PCs), which maximized the explained variance in the data. Each PC represented a different dimension of the TBI burden. The first PC explained the largest proportion of variance, and, in subsequent modeling, the inclusion of PCs beyond the first did not improve model fit. Therefore, for clarity and interpretability, a single summary measure of TBI burden was defined using the first PC, which accounted for 48% of the total variance.
Analysis of the loadings of the first PC revealed that the third instance of TBI and the third instance of AOC contributed the most weight, underscoring their greater role in the overall burden. In contrast, the first instances of TBI and AOC contributed the least, aligning with clinical expectations.
Statistical analyses
All analyses were performed using RStudio 2024.04.2 + 764. Because fluid abilities, white matter integrity, and biomarker levels are known to be susceptible to aging, and preliminary analyses in our data showed age-related changes in these variables, age was controlled for in all models. Missing data were imputed using the “mice” package, utilizing all other variables as predictors for the imputation. 74 Appropriate transformations (detailed under the Results section) were applied to non-normally distributed outcome variables prior to analyses. Adaptive Least Absolute Shrinkage and Selection Operator (ALASSO) regression models identified key predictors for each outcome variable. 75 Briefly, ALASSO applies variable-specific penalties, shrinking less important predictor coefficients to zero while retaining more influential variables in the final model. TBI burden, TBI-related symptoms, white matter integrity, and blood biomarkers were included as predictors for fluid abilities. To obtain key predictors of NSI symptoms, TBI burden, white matter integrity, and blood biomarkers were included in the ALASSO. TBI burden and blood biomarkers were entered into the ALASSO for white matter integrity. Last, ALASSO selected predictors of neuronal injury, vascular injury, glial injury, neurodegeneration, and immune response biomarkers from TBI burden and inflammatory biomarkers. This allowed us to determine potential pathophysiological processes in the chronic phase of mild-to-moderate TBI. For these analyses, the “glmnet” package was implemented in R, which uses a coordinate descent algorithm to optimize model parameters. 76 Ten-fold cross-validation optimized the ALASSO regularization parameters.
Variables selected via ALASSO were subsequently entered into multiple linear regressions for each respective outcome variable. NSI symptom scales exhibited an overdispersion of zeros, which could not be normalized. Therefore, selected predictors for NSI symptoms were entered into either a zero-inflated Poisson (ZIP) or zero-inflated negative binomial (ZINB) model. These models provide a count estimate (indicating the strength of association between each variable and the number of symptoms) and a zero estimate (a logistical model illustrating how each variable influenced the odds of reporting zero symptoms).
Results
Descriptive statistics
Of the 73 individuals who participated in the study, 16 were excluded from all analyses; one due to incomplete scores for the NIH-TB fluid cognition composite, two participants were identified as outliers (>3 SD from the mean) across multiple domains, and 13 were missing neuroimaging data. The results presented here include data from the remaining 57 participants (42 males, M age = 36.632 years, SD = 10.371; range = 19–59 years). The sex distribution of this sample is representative of TBI prevalence, with males being twice as likely to sustain a TBI than females. 77 They had an average of 14.544 years of education (SD = 2.323), and the majority were right-handed (n = 44). Length of time since the most recent TBI varied from 6 to 336 months (M = 114.411, SD = 84.048). The sample was 77% veterans (N = 44), and 26 veterans reported experiencing at least one blast injury. Veterans and civilians differed in PTSD expression and FA in the SLF 1, 2, and 3. However, they did not differ in TBI burden, anxiety, or depression. Demographic characteristics are detailed in Table 1.
The average fluid composite standard score for the sample was 105.61 (range = 77–128). This score falls within normal expectations of performance, indicating that, on average, this sample of individuals with a history of chronic, mild TBI is not impaired in their functioning.
Assumptions for multicollinearity were checked within the full set of predictors. A variance inflation factor cutoff of 10 was used prior to performing ALASSO. Consequently, the NSI total score and IL-1β were removed from the data.
The original data set included separate measures for the left and right hemispheric white matter pathways, which were highly correlated with each other (SLF 1: r = 0.616, p < 0.001; SLF 2: r = 0.796, p < 0.001; SLF 3: r = 0.767, p < 0.001; CBD: r = 0.700, p < 0.001). Thus, measures for the left and right portions of each pathway were averaged to obtain one value per pathway. Branches of the SLF remained separate as their correlations were lower (SLF 1 ∼ SLF 2: r = 0.376, p = 0.004; SLF 2 ∼ SLF 3: r = 0.370, p = 0.004).
TBI burden score
Since ALASSO was not employed for cytokines directly, Pearson correlations with TBI burden scores were computed. TBI burden score was not significantly correlated with any of the cytokines. However, nonsignificant trends showed positive correlations with TNFα, IL-8, IFNγ, and MIP-1α, suggesting higher TBI burden correlated with higher levels of these cytokines. Conversely, TBI burden exhibited nonsignificant, negative correlations with IL-2, IL-4, IL-6, and IL-10. These data are displayed in Table 2.
Results from Pearson Correlations with TBI Burden Score
IFNγ, interferon-γ; IL, interleukin; MIP-1α, macrophage inflammatory protein-1α; TNFα, tumor necrosis factor-α.
Predictors of fluid abilities
An ALASSO for fluid cognition identified 13 factors as yielding nonzero coefficients. A subsequent multiple linear regression using these predictors explained significant variance in fluid cognition scores (adjusted R-squared = 0.562, p < 0.001). Vestibular and affective NSI symptoms were negatively associated with fluid abilities (vestibular: β = −0.022; affective: β = −0.018). FA in the SLF 2, SLF 3, and CBD was positively associated with fluid abilities (SLF 2: β = 0.405; SLF 3: β = 0.295; CBD: β = 0.159), while FA in the SLF 1 was negatively associated (β = −0.297). Three blood biomarkers were selected as important; NF-L and tau were negatively associated with fluid cognition (NFL: β = −0.052; tau: β = −0.047), and UCH-L1 was positively associated (β = 0.036). The model also selected IL-10 and MIP-1α as negatively related to fluid cognition (IL-10: β = −0.066; MIP-1α: β = −0.018), while IL-6 and IFNγ showed positive relationships (IL-6: β = 0.044; IFNγ: β = 0.071).
NSI outcomes
ALASSO analyses for NSI subscales identified predictors for each symptom type. For vestibular symptoms, CBD FA was the sole significant predictor (Fig. 2A). The subsequent ZIP model revealed that higher CBD FA was associated with lower odds of reporting vestibular symptoms (β = 16.004) and fewer symptoms in those reporting (β = −3.652). For somatosensory symptoms, SLF 2 FA was the only predictor selected (Fig. 2B). A ZINB model indicated that increased SLF 2 FA was associated with a reduced likelihood of reporting somatosensory symptoms (β = 8.219) and fewer symptoms in those reporting (β = −7.356).
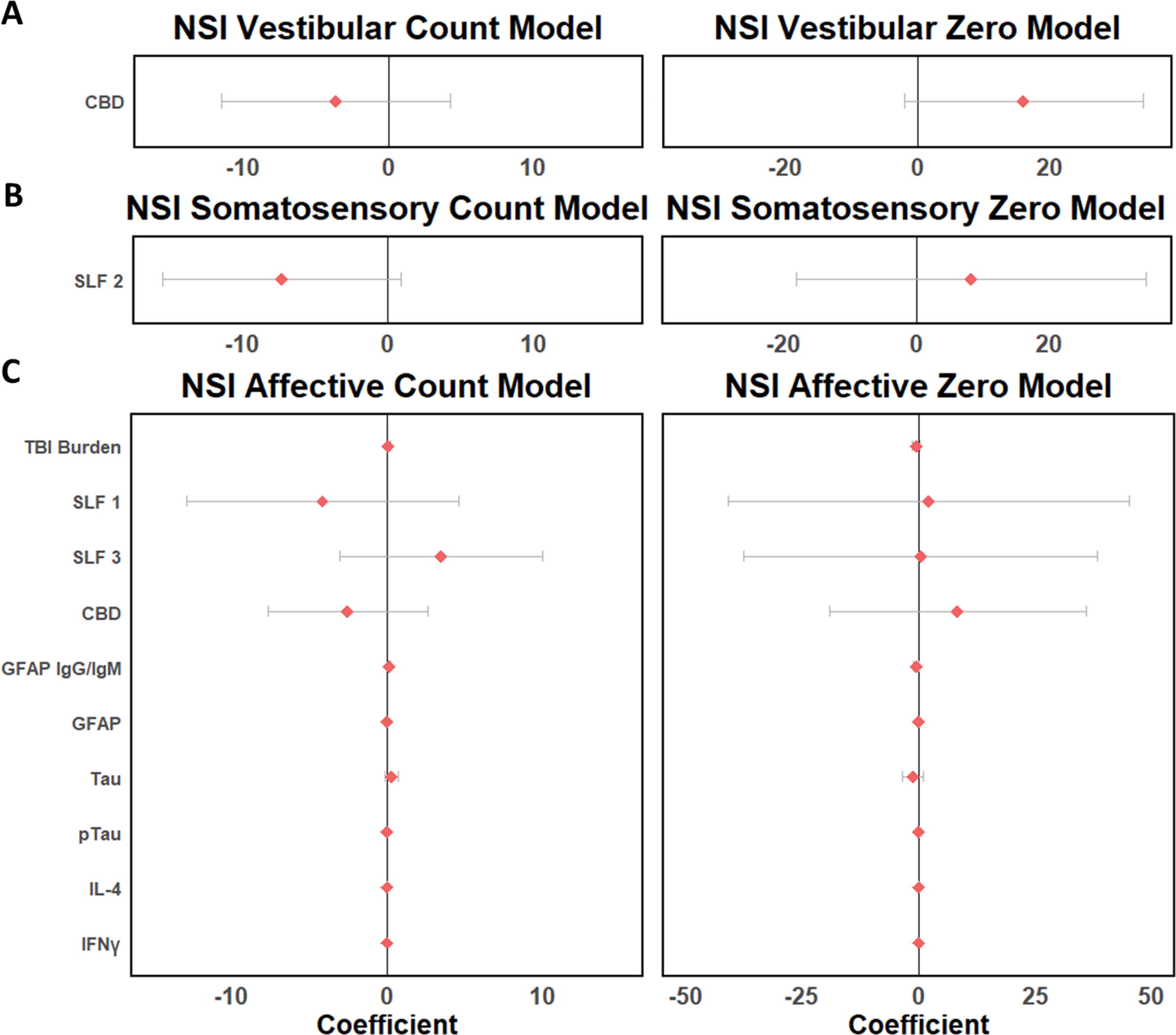
Forest plots depict the coefficients and confident intervals of predictor variables derived from the ZIP for NSI Vestibular symptoms
ALASSO selected 10 factors for predicting affective symptoms (Fig. 2C). ZINB modeling showed TBI burden increased odds of reporting affective symptoms (β = −0.695) and higher symptom counts (β = 0.052). FA in SLF 1 and CBD reduced the odds of reporting symptoms (SLF 1: β = 2.111; SLF 3: 0.404; CBD: β = 8.399), and were associated with lower symptom counts (SLF 1: β = −4.150; CBD: β = −2.528). Conversely, SLF 3 FA was associated with lower odds of reporting symptoms (β = 0.404), but positively correlated with symptom count in those reporting (β = 3.493). Blood biomarkers, such as GFAP IgG/IgM, tau, and P-tau were associated with higher odds (GFAP IgG/IgM: β = −0.520; tau: β = −1.275; P-tau: β = −0.004) and symptom counts for affective symptoms (GFAP IgG/IgM: β = 0.129; tau: β = 0.286; P-tau: β = 0.001), while GFAP showed opposite effects, associated with lower odds (β = 0.023) and fewer symptoms (β = −0.003). This model also revealed that IL-4 and IFNγ were positively associated with symptom count (IL-4: β = 0.002; IFNγ: β = 0.019) and higher likelihood of reporting symptoms (IL-4 β = −0.001; IFNγ: β = −0.002). No variables were selected in the ALASSO for cognitive symptoms.
White matter pathways
For white matter pathways, ALASSO selected five variables for SLF 2 FA; however, the subsequent multiple linear regression did not explain significant variance (adjusted R-squared = 0.121, p = 0.051). Negative associations were observed with TBI burden (β = −0.015), IL-2 (β = −0.017), and TNFα (β = −0.037), while GFAP IgG/IgM (β = 0.020) and NF-H (β = 0.011) showed positively associations. For CBD FA, IFNγ and TNFα were negatively associated (IFNγ: β = −0.063; TNFα: β = −0.070) in a model explaining significant variance (adjusted R-squared = 0.346, p < 0.001). No factors were selected by the ALASSO for SLF 1 or 3 FA.
Neuronal injury, vascular injury, glial injury, neurodegenerative, and immune biomarkers
ALASSO also identified associations between inflammatory biomarkers and markers of neuronal injury, vascular injury, glial injury, neurodegeneration, and immune response. GFAP IgG/IgM, NF-L, tau, NF-H, and P-tau were log-transformed, and GFAP, UCH-L1, and VEGF-A were square-root transformed to achieve normality. For GFAP IgG/IgM, the linear regression containing 10 selected predictors explained significant variance (adjusted R-squared = 0.313, p = 0.002). Negative associations were observed with NF-L (β = −0.210), tau (β = −0.468), VEGF-A (β = −0.511), IL-2 (β = −0.275), IL-4 (β = −0.698), and IFNγ (β = −0.864), while positive relationships were seen with UCH-L1 (β = 0.383), P-tau (β = 0.121), IL-8 (β = 0.772), and TNFα (β = 1.814).
For NF-L, four selected variables explained significant variance (adjusted R-squared = 0.233, p = 0.002). IFNγ and TNFα were negatively associated (IFNγ: β = −0.390; TNFα: β = −0.217), while IL-2 and MIP-1α were positively associated (IL-2: β = 0.260; MIP-1α: β = 0.105). ALASSO for tau selected IFNγ and TNFα, which displayed positive associations (IFNγ: β = 0.223; TNFα: β = 0.50); however, these predictors did not explain significant variance (adjusted R-squared = 0.006, p = 0.357). IFNγ was the only predictor selected for UCH-L1 and displayed a positive relationship (β = 0.373), but did not explain significant variance (adjusted R-squared = 0.071, p = 0.051). TNFα was the only selected predictor for VEGF-A and displayed a positive relationship (β = 0.376). The regression including TNFα explained significant variance in VEGF-A (adjusted R-squared = 0.092, p = 0.028). ALASSO for P-tau identified IFNγ as the only important predictor, which explained significant variance (adjusted R-squared = 0.125, p = 0.010), and exhibited a negative relationship (β = −0.178). No variables were selected by ALASSO for GFAP or NF-H.
Discussion
In this study, we sought to elucidate the mechanisms underlying chronic neurobehavioral outcomes following mild-to-moderate TBI, focusing on white matter injury, neuronal death, cell injury, and neuroinflammation in a predominantly male sample of veterans and civilians. A TBI burden score, derived from instances of TBI, LOC, and AOC, proved important in certain TBI-related symptoms and white matter pathways. We examined relationships between white matter integrity, TBI-related symptoms, blood biomarkers, cytokines, and fluid cognition in veterans and civilians with chronic, remote mild-to-moderate TBI. Results demonstrated robust associations between white matter integrity and fluid abilities, with higher integrity supporting better cognitive performance. Self-reported vestibular and affective symptoms were negatively associated with fluid abilities, while biomarkers and inflammatory markers revealed varied relationships. We further revealed that inflammatory processes have widespread relationships with cognitive and neural outcomes. Higher white matter integrity in various tracts correlated with fewer vestibular, somatosensory, and affective symptoms. Notably, consistent negative relationships were observed between inflammatory cytokines and FA in the SLF 2 and CBD. Inflammatory cytokines were also associated with blood biomarkers, indicating that inflammation, immune response, and secondary injury may be linked. Interestingly, self-reported cognitive symptoms were not associated with any outcomes of interest, including objective cognition (i.e., fluid cognition); however, it may be the case that individual awareness of such symptoms is not as sensitive as it is to symptoms such as mood and bodily sensation. Exploring self-awareness of cognition specifically following TBI may be an interesting avenue for future work, as impaired self-awareness following moderate and severe TBIs has been documented. 78,79 Furthermore, participant’s abilities were largely still in the average range, and it may be that there is a threshold at which cognitive changes are more apparent subjectively. The sample was primarily comprised of veterans, over half of whom had experienced a blast-induced TBI. Compared with civilians, veterans had higher expression of PTSD and lower FA in the SLF 1, 2, and 3. Importantly, blast injury is known to have a different injury profile in both primary and secondary injury, and is likely associated with PTSD expression. 80,81
White matter pathways, including the SLF and CBD, are critical in supporting various cognitive processes. 47,82 Prior reports have suggested that disruption of white matter pathways, indexed by reduced FA, interrupts network communication, and has linked white matter damage to cognitive and functional impairment following TBI. 83 –89 Herein, we found that SLF 1, 2, and 3, and CBD FA were important predictors of fluid cognition. Greater white matter integrity was largely associated with fewer reported TBI-related symptoms. These findings align with literature that emphasizes the critical role of white matter integrity in cognitive function. 83,84 The observed negative relationship between FA and TBI-related symptoms further supports that white matter damage disrupts neural communication, leading to cognitive and functional impairments. 86,87
Furthermore, traumatic axonal injury has been linked to chronic neurodegenerative processes and serves as an important predictor of atrophy following moderate to severe TBIs. 20,90 A number of pathologies triggered by axonal injury can lead to neurodegeneration (i.e., toxic proteinopathy buildup through various processes or disassembly of microtubules, neurofilaments, and other cytoskeletal components), and identifying such processes relies on other biomarkers, including the blood-based biomarkers GFAP, NF-L, NF-H, UCH-L1, and tau. 20,26 In the present study, tau, an indicator of neurodegeneration, was linked to several outcomes. Tau was associated with lower fluid cognition scores, higher reported affective symptoms and higher levels of inflammatory cytokines. This corroborates prior work that has found elevated levels of tau following mTBI in ice hockey players and military personnel. 91,92 The current data suggest that tau may also be closely linked with ongoing inflammation, leading to chronic cognitive effects.
Our findings regarding the chronic relationships between inflammatory cytokines and various biological outcomes are of particular interest given the pivotal role of neuroinflammation in the body’s response to TBI, and its susceptibility to becoming dysregulated. Only a small number of studies have elucidated the role of neuroinflammation in chronic TBI and, to our knowledge, only one has examined the relationship between inflammation and cognitive outcomes. Current analyses with fluid abilities revealed that IL-6, IFNγ, and MIP-1α, which are considered proinflammatory, and IL-10, an anti-inflammatory cytokine were each associated with fluid abilities, with varying directionality. In their 2021 study, Milleville and colleagues linked early inflammatory markers with chronic cognitive outcomes after moderate to severe TBI. They identified TNFα, IL-1β, and MIP-1β to correlate with worse chronic cognitive scores, IL-4 and IL-10, which are anti-inflammatory, to correspond with better cognitive performance, and IL-6 to have less clear relationship. 93 Our findings suggest that chronically, inflammatory processes are associated with many ongoing processes; however, the directionality remains unclear. Recent work has also associated inflammatory responses with numerous mechanisms that may impact cognitive outcomes following TBI, including neuronal injury, white matter damage, BBB disruption, and inhibition of neurogenesis. 28,94 –96
The present study provides support for the involvement of inflammation in various physiological mechanisms in those with a history of TBI. In particular, TNFα (Fig. 3) and IFNγ (Fig. 4), both proinflammatory, were identified as important in many processes. Specifically, TNFα and IFNγ were associated with lower white matter integrity in the CBD, and TNFα was also associated with SLF 2 FA. This finding suggests that elevated inflammation for extended periods may disrupt white matter pathways, which is in line with previous work implicating proinflammatory cytokines in damaging inflammatory processes following TBI. A study investigating postmortem human brain tissue provided evidence of diffuse axonal injury which corresponded with inflammatory responses indexed by cytokine (IL-1β, IL-6, and TNFα) levels in brain tissue. 97 For decades, rat models have demonstrated associations between TNFα and white matter damage such that reduced levels of the proinflammatory cytokine correspond with better white matter outcomes following more severe injury. 98,99 Importantly, while studies have established both neuroinflammation and neurodegeneration following TBI of all severities, few studies have sought out a causal link between them and most have been in rodent models. These studies link microglial accumulation and damage to white matter, but not inflammatory cytokines. 100 However, TNFα has been found to induce microglia activation and ultimately neuronal cell death, thus we may expect that these and other proinflammatory biomarkers would be observed with white matter degradation if there is persistent change occurring in some patients with a history of remote TBI. 101
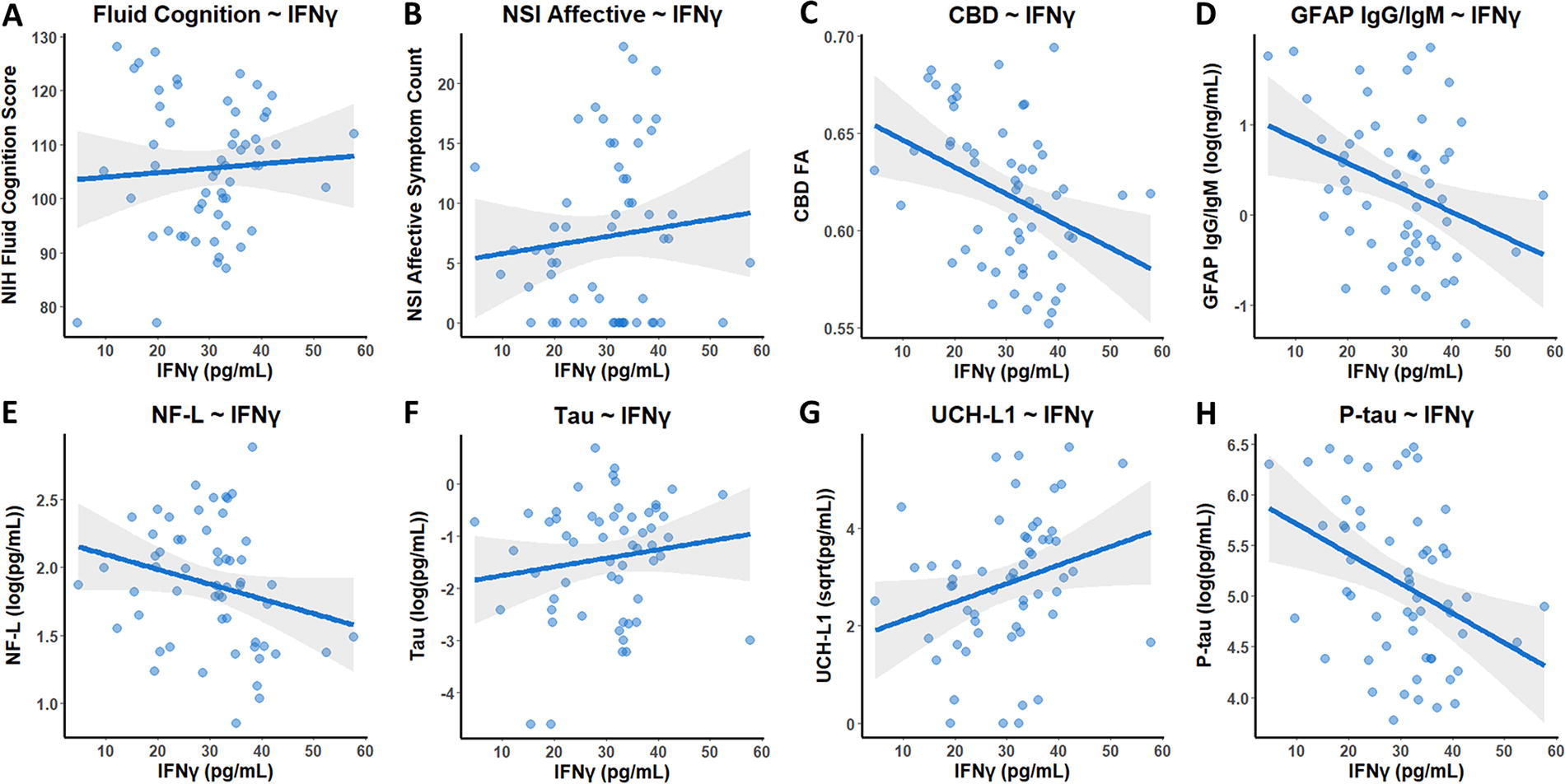
Selected associations with IFNγ. Scatter plots depict the raw correlations for which IFNγ was selected as being an important predictor. The overall trend for each plot is represented by a line of best fit with gray shading representing the 95% confidence interval. Results show that higher IFNγ was associated with higher fluid cognition score
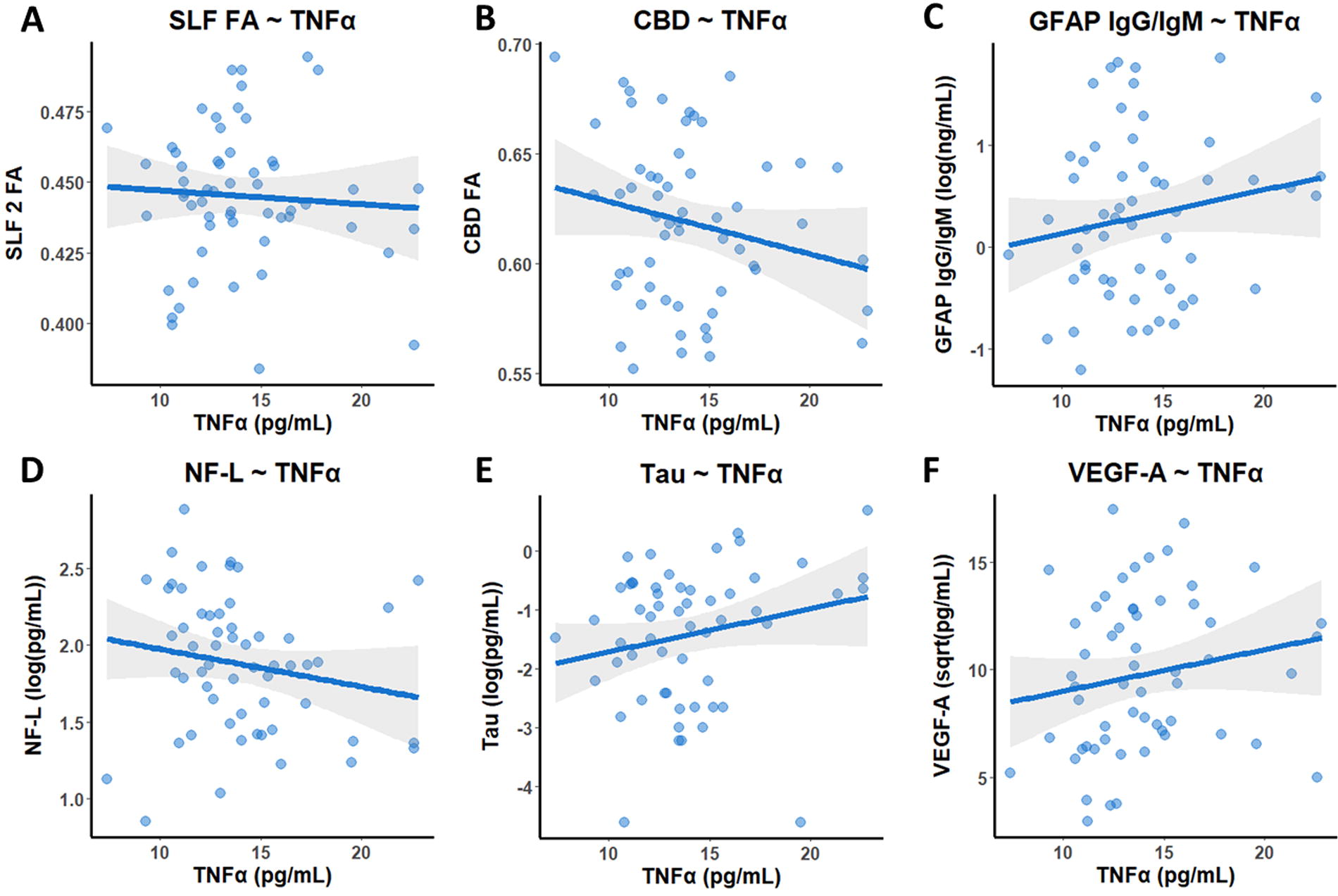
Selected associations with TNFα. Scatter plots display the raw correlations for which TNFα was selected as being an important predictor. The overall trend for each plot is represented by a line of best fit with gray shading representing the 95% confidence interval. Higher TNFα was associated with lower FA in the SLF 2
While N is small, current results suggest that specific cytokines were also linked to blood biomarkers of neuronal and vascular injury, neurodegeneration, and immune response. Both TNFα and IFNγ were associated with GFAP IgG/IgM, an indicator of immune response. TNFα showed a positive association with GFAP IgG/IgM, suggesting a connection to a more chronic inflammatory response. GFAP IgG is generally produced during the later immune response stages, indicating a shift toward chronicity. Conversely, IFNγ exhibited a negative relationship with GFAP IgG/IgM. Additionally, TNFα was associated with other biomarkers, including NF-L, tau, and VEGF-A levels. IFNγ was linked to NF-L, tau, UCH-L1, and P-tau. Under normal physiological conditions, the microtubule-associate protein tau maintains the cytoskeleton by binding to and stabilizing microtubules. 102 In disease, abnormal chemical changes, such as phosphorylation, cause tau to detach from and destabilize microtubules, resulting in defective axonal transport. The accumulation of misfolded and aggregated tau results in a toxic neuronal gain-of-function. 102 The observed associations of tau with both TNFα and IFNγ indicate potential involvement of inflammation in neurodegenerative processes. VEGF-A, crucial for angiogenesis and vascular permeability, along with TNFα, which has also been implicated in BBB permeability, may suggest chronic alterations in BBB permeability due to ongoing neuroinflammation. This aligns with previous findings of such changes in patients with mTBI experiencing postconcussive symptoms. 103,104
Although causality cannot be inferred, these associations offer insights into chronic processes that may indirectly contribute to outcomes following injury. Results revealed TNFα to be associated primarily with biomarkers of underlying injury in a direction that would suggest ongoing inflammation may be associated with further injury. However, IFNγ displayed more variable directionality. Such trends suggest that TNFα is contributing to more harmful inflammatory processes in the chronic phase, while the effects of IFNγ are more mixed. Furthermore, this provides evidence that chronic inflammatory processes may not benefit brain health or recovery to a homeostatic state. It is important to recognize that other processes beyond TBI are likely contributing to ongoing neurological injury; in fact, that is more likely the case than not. Furthermore, varied relationships between inflammatory cytokines and biomarkers of neuronal, vascular, and glial injury, neurodegeneration, and immune response indicate a complex and nuanced role of cytokines in the chronic phase, warranting further research to fully understand these interactions.
In addition to demonstrating potential mechanisms underlying the fluid abilities in a population of individuals with chronic mild-to-moderate TBI, we created a TBI burden score from the cumulative severity of TBI for each individual and observed how this score was related to fluid abilities, FA, TBI-related symptoms, and blood biomarkers. We found that TBI burden was selected as important in predicting affective symptoms and SLF 2 FA, with greater TBI burden supporting increased symptom reports and decreased white matter integrity. These results suggest that mild-to-moderate instances of TBI may have lasting impacts on various chronic systemic processes. Some researchers have suggested that even mild injuries can “prime” neuronal cells, resulting in amplified, longer-lived inflammatory signaling in response to a subsequent challenge. 100,105 However, it is important to emphasize that we are studying a mild-to-moderate TBI population greater than 6 months after injury, so it is highly likely that inflammatory and neurodegenerative processes are impacted by other ongoing processes such as chronic stress, PTSD, and changes in sleep.
Limitations
The present study provided analyses with an array of biomarkers that have been hypothesized as being important in TBI outcomes. Few studies have reported the analysis of multiple-process biomarkers in the context of neuroimaging and cognitive outcomes. We were able to analyze these biomarkers in the chronic phase of a mild-to-moderate injury sample and provide convergent evidence suggesting that one or more of these biomarkers chronically affect outcomes following injury. However, despite several strengths, there remain notable limitations in the current study. First, the sample of the present study is a predominantly male, veteran population. While the sex distribution is representative of the occurrence of TBI, it is important to keep in mind that outcome may look different between sexes, and the results observed in this study are most representative of males. Future research would benefit from including a more balanced sample or examining these outcomes in females specifically. Furthermore, the cross-sectional design of the study included no preinjury metrics, leaving us with temporal uncertainty regarding the order of events, particularly pertaining to whether lower fluid abilities resulted from injury, and if structural differences are a change from the individual’s baseline. However, it is notable that TBI burden was important in white matter and symptom reports. Nevertheless, we can only speak to trends observed and potential factors that may be driving them. It is also important to note in chronic to remote TBI, it is difficult to conclude that neurophysiological factors and behaviors are directly related to injury. While it is valuable to identify converging trends in the data, it is difficult to obtain a strong biomarker signal in this sample, and we were underpowered in running more complete mediation and moderation analyses (i.e., our sample benefits from a very wide array of biomarker, neuroimaging, and behavioral data, but it is underpowered to fully evaluate the interplay between these factors). Additionally, there are many reasons why someone may experience persistent complaints, and several conditions, such as PTSD, anxiety, and depression, which are known to produce similar symptom complaints and affect symptoms of TBI. Given the large prevalence of veterans in the current sample, it is highly likely that these comorbid factors and other bodily functions are contributing to processes that we are observing, such as chronic inflammation, though it is interesting that TBI burden appears to have an impact. Complicating matters, damage from TBI may affect the expression of these symptoms, interacting to impact cognition and long-term brain health. 15 Attempting to discern these effects was outside the scope of the present study. Additionally, future studies may consider a direct comparison of the TBI population to healthy controls including neuroimaging.
Conclusions
Overall, this study advances our understanding of physiological alterations in individuals with mild-to-moderate TBI and links these changes to cognitive outcomes. Our findings reinforce growing evidence that even mild injuries may result in long-term deviations from baseline functioning. We demonstrate that persistent processes following mild-to-moderate TBI, such as chronic symptoms, white matter disruption, inflammation, immune response, and underlying cellular injury, can negatively impact brain structure and behavior, even when these changes are subclinical. Furthermore, our work suggests that various ongoing processes may have compounding effects on long-term outcomes, leading to indirect consequences. For instance, inflammation might impact white matter integrity, symptomology, biomarkers of axonal and neuronal injury, or immune response, ultimately influencing cognitive performance. While further research is needed to elucidate the nature of these relationships in the mild-to-moderate TBI population, our results provide valuable insights to guide future investigations. By identifying key mechanisms of interest, this study lays the groundwork for more targeted research designs and interventions aimed at improving outcomes for individuals with TBI.
Transparency, rigor, and reproducibility summary
Serum samples were obtained from a cohort of chronic, remote TBI participants at UF. Samples were collected between 2019 and 2022. The UF cohort (age 18–60 years) was recruited from a VA Informatic and Computing Infrastructure generated list that provides contact information for veterans who have had a mild-to-moderate TBI at some point in their lives, and greater than 6 months prior, as well as through fliers placed in throughout the local Gainesville, FL community. Serum samples from consenting patients were collected once during their research visit. Samples were centrifuged for 15 min at 1500 × g, and the serum was removed. Serum samples were stored at −80°C until analyzed.
Demographics are provided for the UF cohort (Table 1). The Ohio State University (OSU)-TBI was used to capture information from the participants about prior head injuries. If patients obtained a head injury within 6 months before their visit, or a head injury that was categorized as greater than moderate, they were excluded from the study.
The de-identified clinical and biomarker data are available in the Federal Interagency Traumatic Brain Injury Research (FITBIR ID: FITBIR-STUDY0000396; DOI: 10.23718/FITBIR/1518842). The authors agree to publish the article using the Mary Ann Liebert Inc. “Open Access” option under the appropriate license.
Footnotes
Data Sharing
The data presented are part of a larger completed funded study. Consistent with the sharing language associated with informed consent of this study population, the sharing of de-identified raw data supporting the study findings will be considered upon reasonable request. Summary data associated with this work are also publicly available through FITBIR (FITBIR ID: FITBIR-STUDY0000396; DOI: 10.23718/FITBIR/1518842).
Authors’ Contributions
Funding: R.R., K.K.W.W., A.K.W., C.R., and J.B.W. Literature search: S.H.P. Study design: R.R., K.K.W.W., A.K.W., C.R., D.L., and J.B.W. Data collection: A.B.W., J.B.W., and D.L. Data analysis: S.H.P., A.B.W., S.S., S.D., R.R., A.K.W., D.L., F.K., and K.K.W.W. Data interpretation: S.H.P., A.B.W., and J.B.W. Writing: S.H.P., A.B.W., L.E.M., and J.M. Review and revision of the report: R.R., F.K., K.K.W.W., and J.B.W. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Author Disclosure Statement
K.K.W.W. is a shareholder of Gryphon Bio, Inc. The other authors have no competing interests.
Funding Information
This work was supported, in part, by the Assistant Secretary of Defense for Health Affairs endorsed by the Department of Defense, through the Defense Medical Research and Development Program under award numbers W81XWH19-2-0012 and W81XWH-071-0701, and by the Rehabilitation Research & Development Service (RR&D) of the Veterans Health Administration, through the Brain Rehabilitation Research Center (BRRC) under award number B3000-C. The opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by the Department of Defense and/or other funding agencies. In addition, the funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.