
Abstract
Acute traumatic cervical spinal cord injuries (TCSCI) are associated with significant mortality and morbidity, particularly when complicated by neurogenic respiratory failure. While upper cervical-level injuries are established risk factors for mechanical ventilation, patients with acute injuries below the fifth cervical level without significant chest trauma may also require ventilatory support. However, reliable early predictors remain unclear. This study aims to identify the primary predictors of early mechanical ventilation needs in patients with acute TCSCI. We conducted a retrospective analysis of 148 cases of TCSCI treated between 2019 and 2022. Among these, 27 cases (18.24%) required ventilatory support. Multivariate analysis revealed that a compression grade of 2 or higher, exceeding 25% on Computed Tomography (CT) (adjusted odds ratio [aOR]: 10.18; 95% CI: 2.03–50.94; p < 0.001), and a cord contusion length spanning at least two levels on Magnetic Resonance Imaging (MRI) (aOR: 2.11; 95% CI: 1.06–4.22; p = 0.03) were significant independent predictors. CT-based spinal cord compression measurements showed a strong correlation with MRI findings (linear regression coefficient = 0.88, 95% CI: 0.80–0.96; Spearman’s rho = 0.90; both p < 0.001). The regression line was closely aligned with the equality line, indicating CT can reliably approximate MRI. Noninferiority testing revealed no significant difference in predicting mechanical ventilation risk between modalities (p = 0.21). Survival analyses stratified by compression grades demonstrated similar predictive performance, with higher compression grades (2–4) associated with increased risk of ventilation over time. These findings suggest that the degree of cord compression and cord contusion length are reliable, noninvasive predictors of the need for mechanical ventilation in TCSCI, emphasizing the importance of early recognition, cost-effective health care management, and prognostic counseling. The Subaxial Injury Classification and Severity Scale demonstrated borderline significance (sensitivity 81.5%, specificity 87.6%). The study found that patients with >25% cervical spinal cord compression had significantly poorer outcomes compared to those with ≤25% compression, including longer hospital stays, lower survival rates, worse pre-treatment neurological status, and higher complication rates. Surgical treatment, particularly the posterior approach, was more common in the >25% compression group; however, post-treatment neurological improvement was observed only in cases of grade 2 degree compression, not grades 3 and 4 in CT and MRI. In contrast, the ≤25% compression group demonstrated better outcomes, with greater post-treatment improvement.

Introduction
Traumatic cervical spinal cord injuries (TCSCI) exhibit a significant public health concern worldwide. The prevalence of these injuries ranges from 10.4 to 83 per million people per year. 1 Among people in Wuhan, China, with TCSCI between 2016 and 2021, 15.98% experienced morbidity and were classified as American Spinal Injury Association (ASIA) Classification A (complete cord syndrome), followed by 14.5% classified as Classification B. 2 Previous studies have highlighted differences in mortality rates between developed and developing countries.3–5 Motor vehicle accidents and falls from a significant height were the primary causes of TCSCI, particularly among young male patients, 6 and have shown that TCSCI can lead to long-term dysfunction across multiple organ systems, resulting in increased morbidity and decreased quality of life.7,8
Acute complications such as neurogenic shock, bradyarrhythmias, hypotension, ectopic beats, abnormal temperature regulation, sweating abnormalities, vasodilation, and autonomic dysreflexia frequently occur in individuals with TCSCI during the acute phase, notably in emergency departments and neurosurgery units, where mortality rates are elevated. 9
Following TCSCI, respiratory failure is a common occurrence within the first-day post-injury, necessitating mechanical ventilation (MV).10–12 Respiratory complications and failure, often characterized by hypoxemia and cerebral anoxia,10–13 are significant contributors to mortality in TCSCI cases. Identifying factors associated with MV can help predict patients at risk and in need of intubation, thereby preventing hypoxia and reducing in-hospital mortality.
Several studies indicate risk factors for MV in TCSCI, including injuries above the C5 level14–16 and decreased minute ventilation due to environmental factors. 17 Some studies have discussed the severity of the injury as a predictor for respiratory failure in TCSCI, focusing on factors such as complete cord syndrome or ASIA score.18,19 However, there is no conclusive evidence on the risk factors for definitive MV that are easily examined or observed. The objective of this article is to investigate the cervical level of injury factors and severity factors associated with MV and to identify significant independent predictors of early respiratory failure prior to the onset of hypoxia in TCSCI patients.
Material and Methods
A retrospective data collection was conducted on patients diagnosed with TCSCI at Ratchaburi Hospital in Ratchaburi Province, Thailand, between 2019 and 2022. The patients were monitored for the occurrence of MV during their hospital stay. Patients with TCSCI secondary to other factors, such as bleeding disorders or spinal cord tumors, were excluded from the study. Four patients with associated injuries that could be primary causes of respiratory compromise, such as pneumothorax, flail chest, lung contusions, or severe head injury, were excluded from the study.
MV was indicated for patients with TCSCI who experienced severe respiratory distress, including hypoxemia or hypoventilation, particularly oxygen saturation below 90% despite supplemental oxygen, or those with significant loss of diaphragmatic or intercostal muscle function. Additionally, patients who were unable to protect their airway due to an impaired cough reflex, difficulty clearing secretions, or dyspnea were also considered for MV.
Personal history and general information, including gender, age, underlying diseases, alcohol consumption, smoking habits, and mechanisms of injury, were recorded. Diagnostic imaging results were obtained from all medical records. All patients underwent emergency Computed Tomography (CT) scans, while Magnetic Resonance Imaging (MRI) was performed for those with neurological deficits from the injury. Radiologists interpreted and measured key parameters, including the degree of spinal cord compression, vertebral and posterior column fractures, facet joint lock, compression and burst fractures, and distracting and rotation/translation injuries using CT scans. Spinal cord contusion, disc lesions, and discoligamentous complex (DLC) status were evaluated using MRI scans and interpreted with Synapse software version 4.4.210 (Fujifilm Thailand, Bangkok, Thailand).
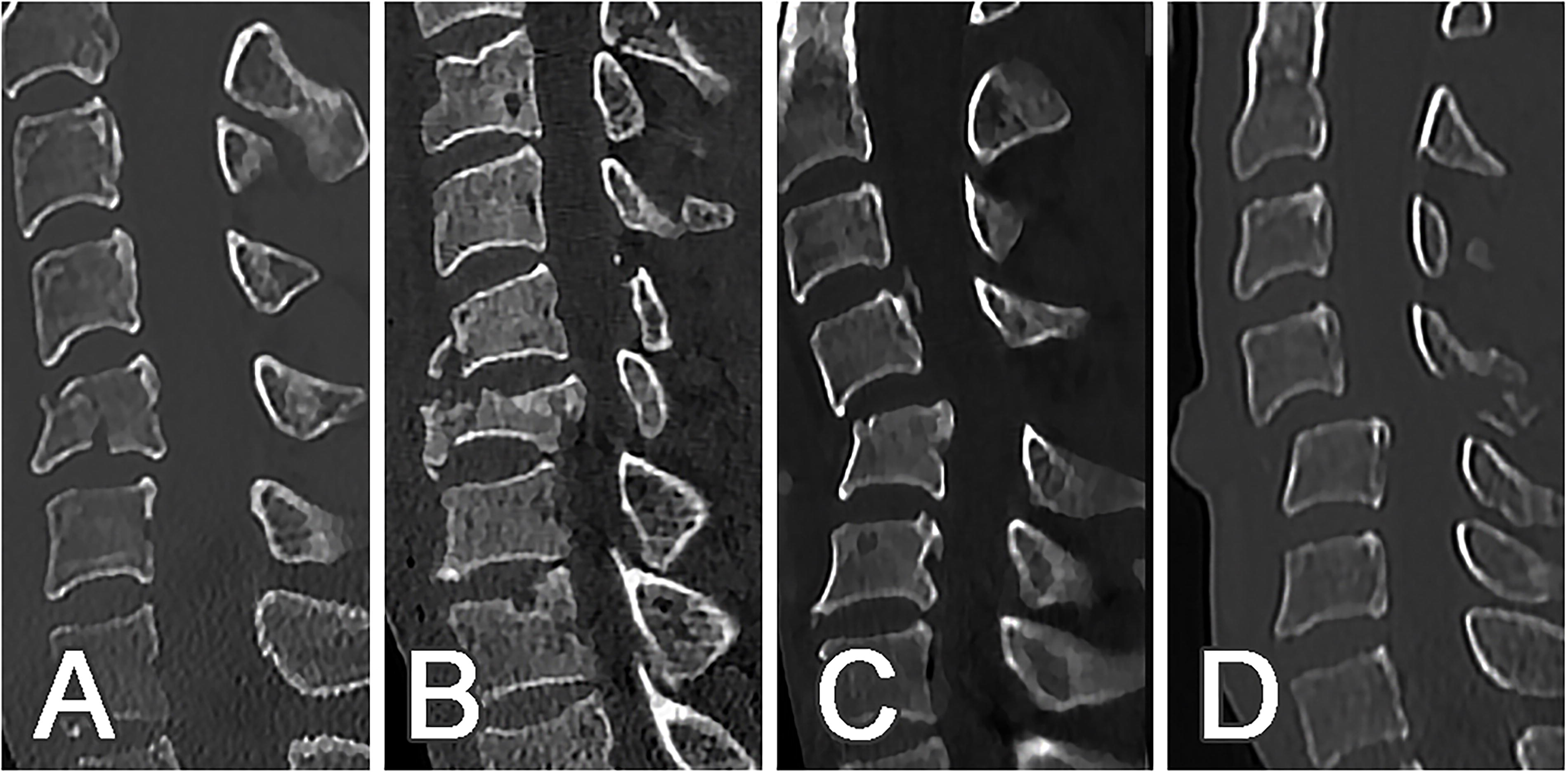
The degree of compression was evaluated by measuring the percentage of spinal cord compression based on the diameter occupied within the spinal canal, using both CT and MRI. Classification grading was performed as follows: Grade 1 represents compression ranging from 1% to 25%, grade 2 indicates compression between 26% and 50%, grade 3 signifies compression between 51% and 75%, and grade 4 represents compression ranging from 76% to 100% (Fig. 1).

The upper panel shows CT scans, while the lower panel shows MRI scans. The degree of spinal cord compression is graded as follows: Grade 1 (panel 1): 1–25% compression; grade 2 (panel 2): 26–50%; grade 3 (panel 3): 51–75%; and grade 4 (panel 4): 76–100%, indicating severe compression. White lines in the first column illustrate the measurement method.
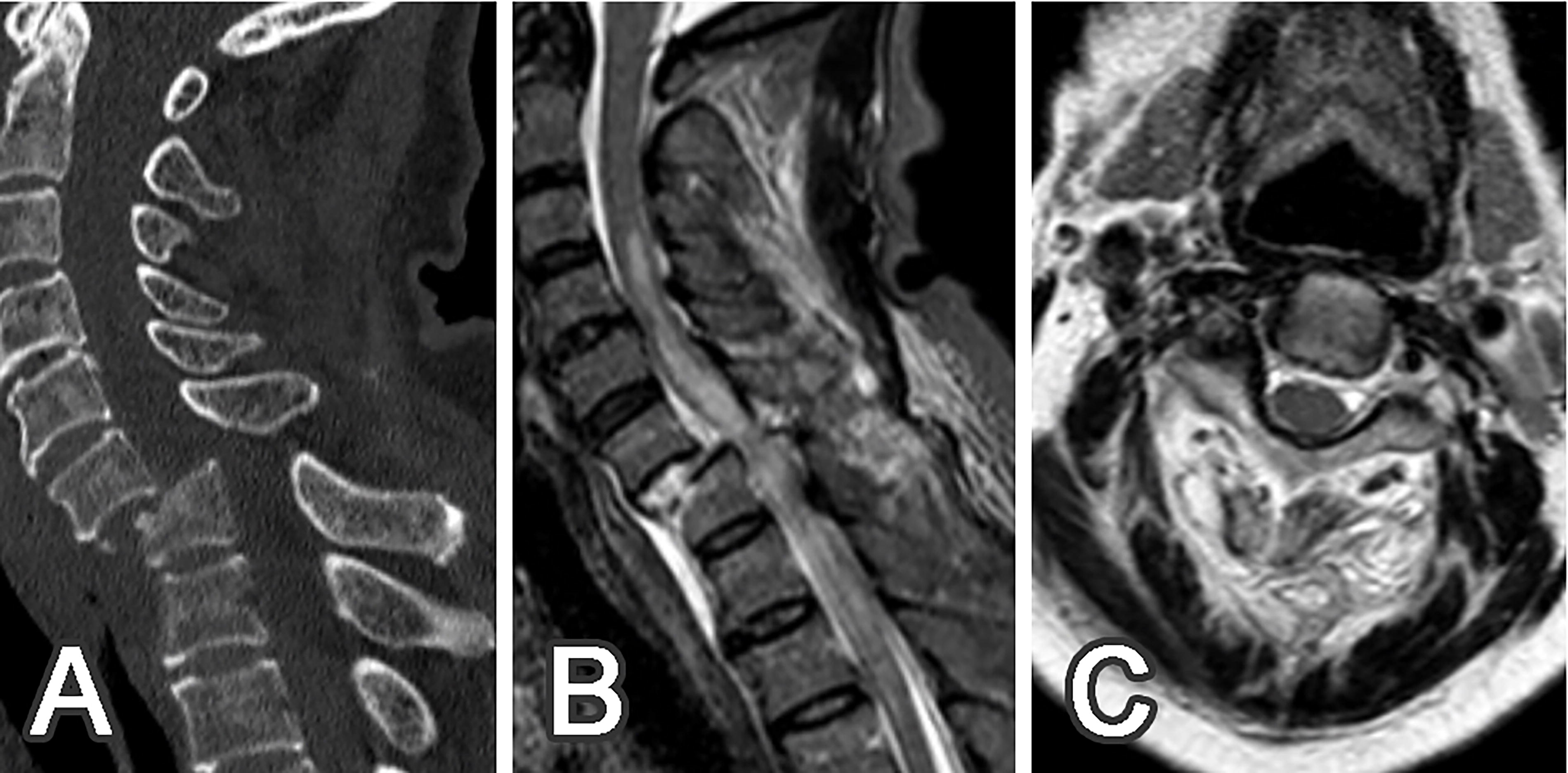
A spinal cord contusion occurs when the cord is compressed, causing damage while sparing some of its tissue. Importantly, the ventral nerve fibers linking the spinal cord above and below the injury usually remain undamaged. 20 MRI scans reveal a distinctive pattern with a high T2 signal rim encircling a central low area at the site of the spinal cord contusion. Cord contusion length is determined by counting the cervical vertebral levels affected in T2-weighted imaging MRI (Fig. 2).

T2-weighted imaging (T2WI) MRI reveals a rim of hypersignal intensity within the intramedullary spinal cord, indicating spinal cord contusion. The contusion is observed at the C3 and C4 vertebral body height levels, with an interpreted cord contusion length spanning two vertebral levels.
Morphological changes in spinal injuries vary depending on the mechanism of injury. Compression fractures typically result from axial forces coupled with flexion, primarily affecting the anterior column of the vertebral body. Burst fractures result from severe axial loading, leading to injury to the anterior and middle portions of the spinal column. Distraction injuries stem from vertical displacement, often associated with flexion-distraction mechanisms. These injuries involve failure of the middle and posterior columns under tension, leading to the widening of the interspinous spaces. Rotation/translation injuries are characterized by severe horizontal displacement or rotation of one vertebral body concerning another. This type of injury may involve vertebral subluxation, translation, or rotation, sometimes accompanied by facet joint locking and DLC (Fig. 3).
Morphology:
The DLC comprises several anatomical structures: the intervertebral disc, anterior longitudinal ligament, posterior longitudinal ligament, ligamentum flavum, facet capsules, interspinalis muscle, and supraspinous ligaments. DLC injuries represent severe spinal trauma involving both the intervertebral disc and the ligamentous structures. CT scans may reveal widening of the intervertebral and posterior interspinous spaces, as well as potentially associated subtle bony fractures or avulsions, along with paravertebral hematomas or complications such as epidural hematomas. MRI imaging may reveal disruptions, tears, or herniations of the intervertebral disc, which are evident as hypersignal intensity in T2-weighted images (Fig. 4).
Demonstrates discoligamentous injuries:
The data analysis was performed using Stata software version 17 (StataCorp, College Station, TX, USA). A comparison was conducted between patients requiring MV during hospitalization and those who did not. For variables with a normal distribution, Student’s t-test or Mann–Whitney U test were utilized. Univariate and multivariate logistic regression analyses were performed for categorical data. Kaplan–Meier survival analysis was conducted for patients who did not require MV, and failure analysis was performed to evaluate post-treatment improvement in functional outcomes. A significance level of p < 0.05 was considered statistically significant.
Results
Between 2019 and 2022, 148 TCSCI cases were identified, with 27 (18.24%) requiring MV. Table 1 summarizes the demographic and clinical characteristics associated with the need for MV. The majority of patients were male (84.46%), but gender showed no significant association with the need for MV (19.20% in males vs. 13.04% in females, p = 0.49). Age was significantly associated, with patients requiring MV being older (mean age: 58.70 ± 16.42 vs. 50.11 ± 14.94, p = 0.01, unadjusted odds ratio [uOR]: 1.04, 95% CI: 1.01–1.07). Among underlying diseases and lifestyle factors, such as smoking and alcohol use, none were significantly associated with MV. Regarding etiology, traffic accidents were significantly less likely to be associated with MV (uOR: 0.20, p < 0.001), while falls significantly increased the odds (uOR: 4.83, p < 0.001). Body assaults showed no significant relationship (p = 0.43). These findings suggest that advanced age and falls as a mechanism of injury are significant predictors of the need for MV, while other variables were not significantly associated.
Demographic Data of History

SD, standard deviation; uOR, unadjusted odds ratio.
The severity parameters significantly associated with the need for MV include the degree of spinal cord compression and cord contusion. Higher compression grades were strong predictors, with grade 2 (26–50%) increasing the odds of MV by 12.53 times in CT and 59.82 times in MRI (p < 0.001), grade 3 (51–75%) by 56.40 times in CT and 202 times in MRI (p < 0.001), and grade 4 (76–100%) showing a 100% MV incidence in both CT and MRI. Cord contusion was present in all MV patients, with longer contusion lengths significantly increasing risk. A contusion length of two levels increased the risk for MV with an odds ratio of 2.70 (p = 0.04); three levels had an odds ratio of 4.50 (p = 0.01); four levels increased the odds by 6.48 times (p < 0.001); and five levels by 13.50 times (p < 0.001). These findings highlight the predictive value of severe spinal compression and extensive cord contusion for MV (Table 2).
Severity Parameters of Traumatic Cervical Spinal Cord Injury
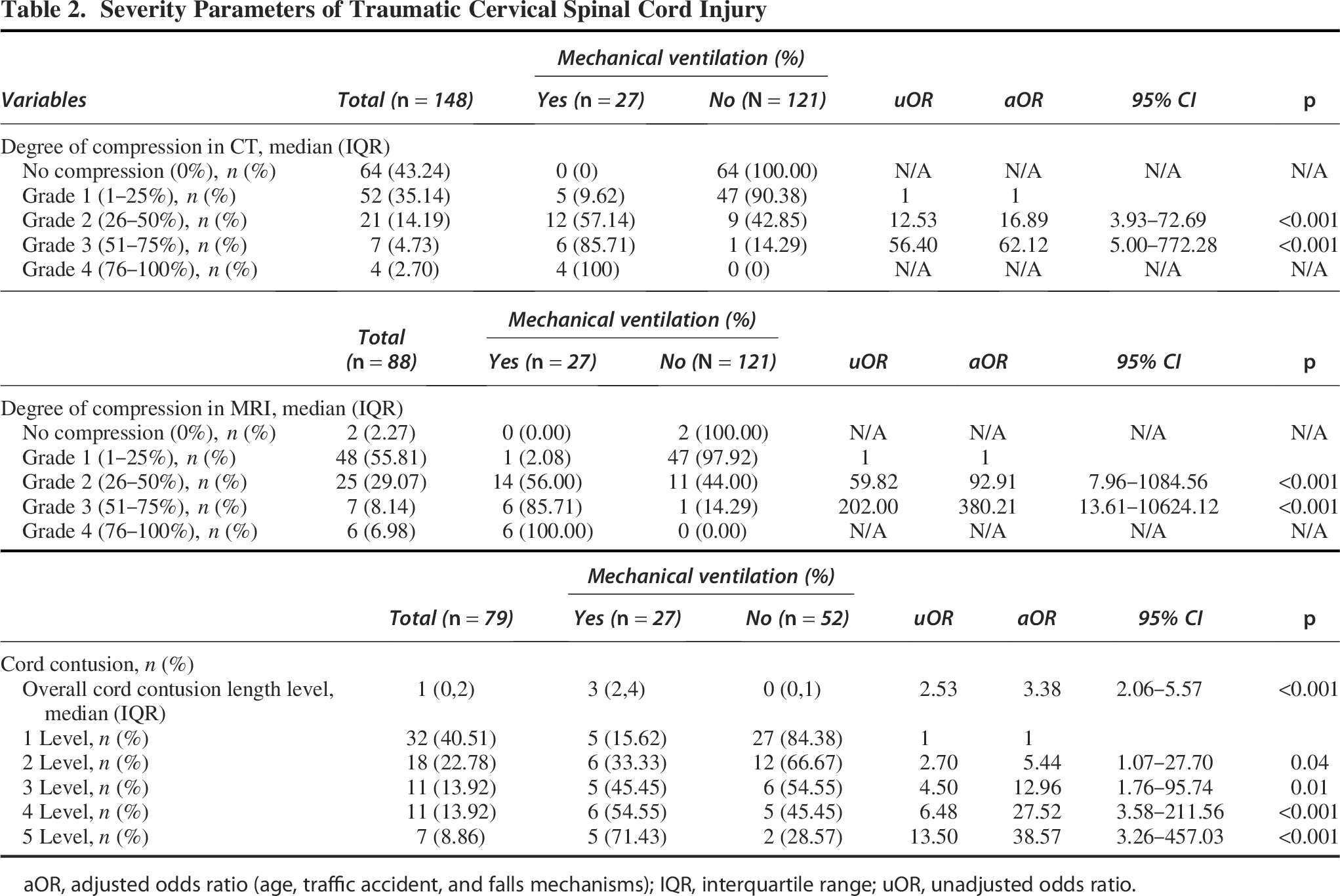
aOR, adjusted odds ratio (age, traffic accident, and falls mechanisms); IQR, interquartile range; uOR, unadjusted odds ratio.
Figure 5 illustrates the correlation between spinal cord compression measurements obtained from CT and MRI. Linear regression analysis shows a strong correlation between the degree of compression on CT and MRI, with a coefficient of 0.88 (95% CI: 0.80–0.96, p < 0.001) and Spearman’s rho of 0.90 (p < 0.001), indicating a consistent relationship between the two modalities. The regression line closely follows the line of equality, suggesting that CT measurements can reliably approximate MRI findings. Additionally, a noninferiority test comparing the risk of MV between CT- and MRI-based compression grades demonstrates no significant difference (F-statistic = 1.59, p = 0.21). Survival analyses of patients who did not require MV, stratified by compression grades on CT and MRI (panels B1 and B2), indicate that patients with higher degrees of compression (grades 2–4) are significantly more likely to require MV. Furthermore, a noninferiority test for improvement in ASIA classification (F-statistic = 1.99, p = 0.16) supports comparable prognostic utility between the two imaging modalities. Panels C1 and C2 show that patients with moderate compression, particularly grade 2, exhibited a higher rate of improvement in ASIA classification over time, whereas those with severe compression—especially grade 4—showed no improvement.
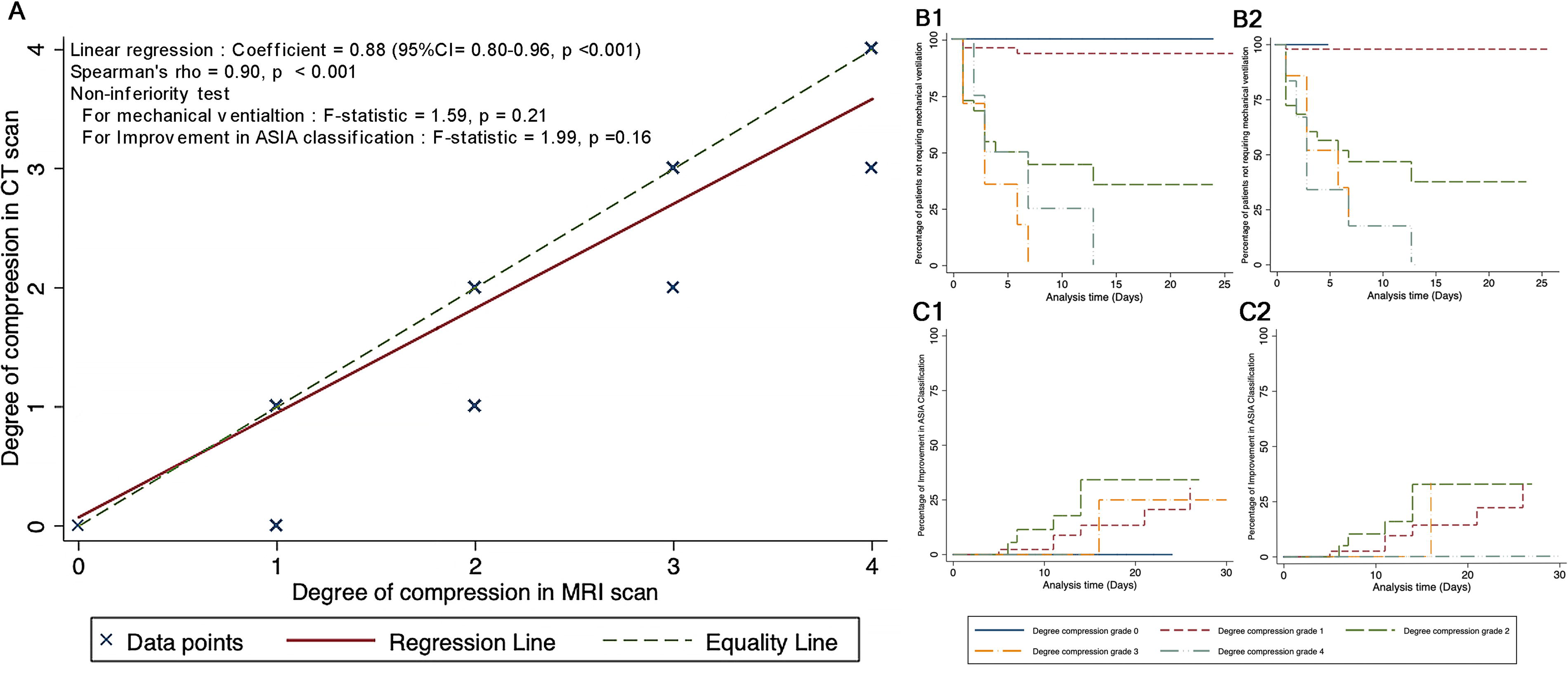
Correlation between CT and MRI measurements of spinal cord compression, survival analysis of spinal compression grades, and post-treatment ASIA Classification outcome.
Analysis of cervical cord injury severity based on CT scans revealed that injuries at the C2–3 level significantly increased the odds of requiring MV (10.14%, uOR: 3.56; p = 0.03), while other levels showed no statistical significance. On MRI, spinal cord contusion was most common at the C4–5 (58.23%) and C5–6 (55.70%) levels. MV was required in all cases at the C1–2 level (5.06%) and in a majority at C2–3 (69.23%, mOR: 7.46; p = 0.03), C4–5 (45.65%, mOR: 16.71; p < 0.001), and C6–7 (46.67%, mOR: 8.42; p < 001). In contrast, cases at C3–4 (39.02%, mOR: 0.91; p = 0.89) and C5–6 (38.64%, mOR: 0.39; p = 0.27) showed no significant association with MV. These findings are associated with spinal cord injury (SCI) levels C2/3, C4/5, and C6/7; however, levels C3/4 and C5/6 did not exhibit a consistent trend (Table 3).
Level of Injury of Traumatic Cervical Spinal Cord Injury
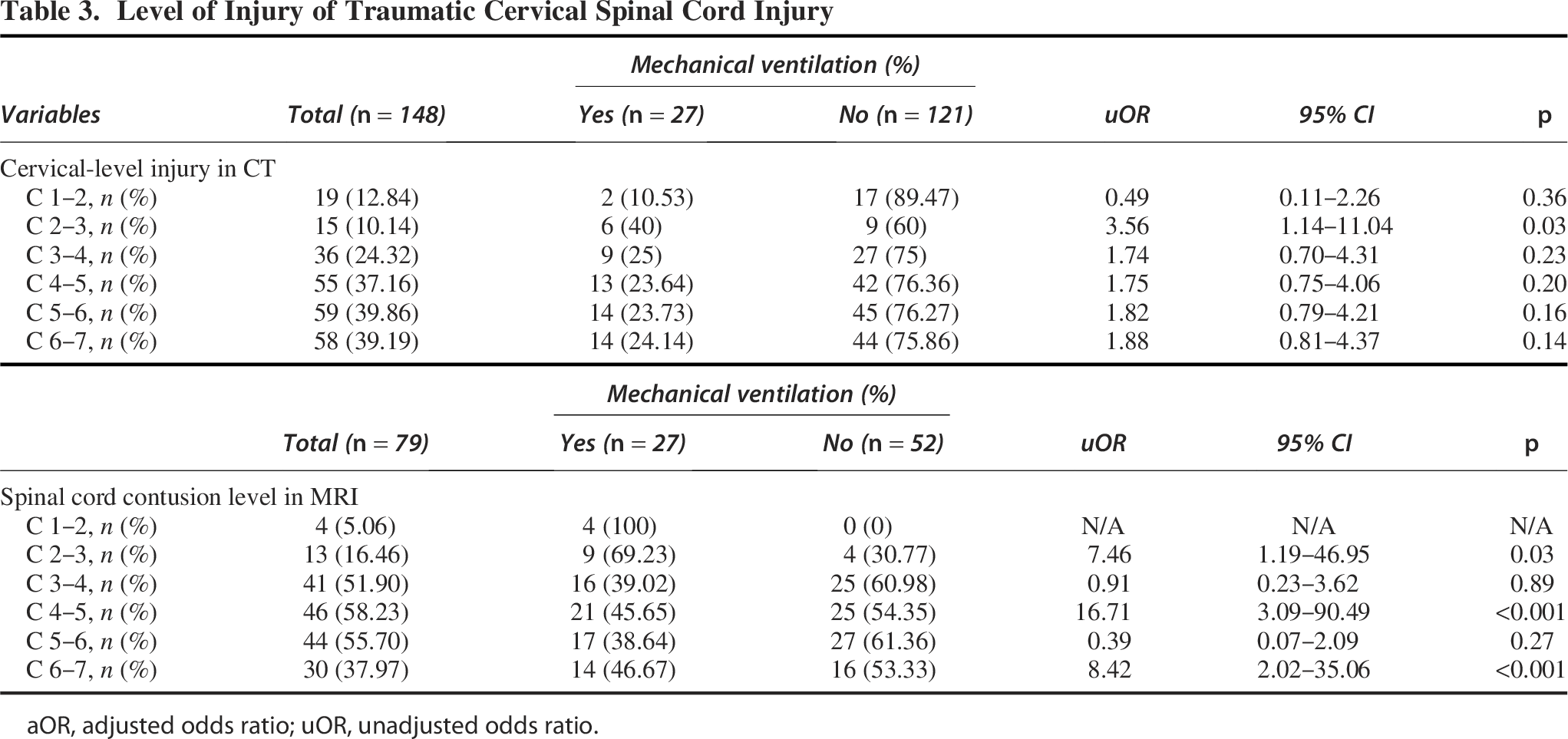
aOR, adjusted odds ratio; uOR, unadjusted odds ratio.
The analysis of morphological changes in TCSCI revealed several key associations with the need for MV. Patients requiring MV were significantly more likely to have posterior column fractures (uOR: 2.64, p = 0.03), locked facet joints (uOR: 31.47, p < 0.001), and rotation/translation injuries (uOR: 12.08, p < 0.001). Additionally, the DLC status showed a higher prevalence of intermediate (uOR: 31.20, p < 0.001) and disrupted (uOR: 25.60, p < 0.001) conditions in the ventilation group. The Subaxial Injury Classification and Severity Scale (SLICS) score was also significantly higher in these patients (median 7 vs. 1, p < 0.001), indicating more severe TCSCI. These findings suggest that certain morphological changes are strongly associated with the need for MV in this patient population (Table 4).
Morphological Change Parameters of Traumatic Cervical Spinal Cord Injury
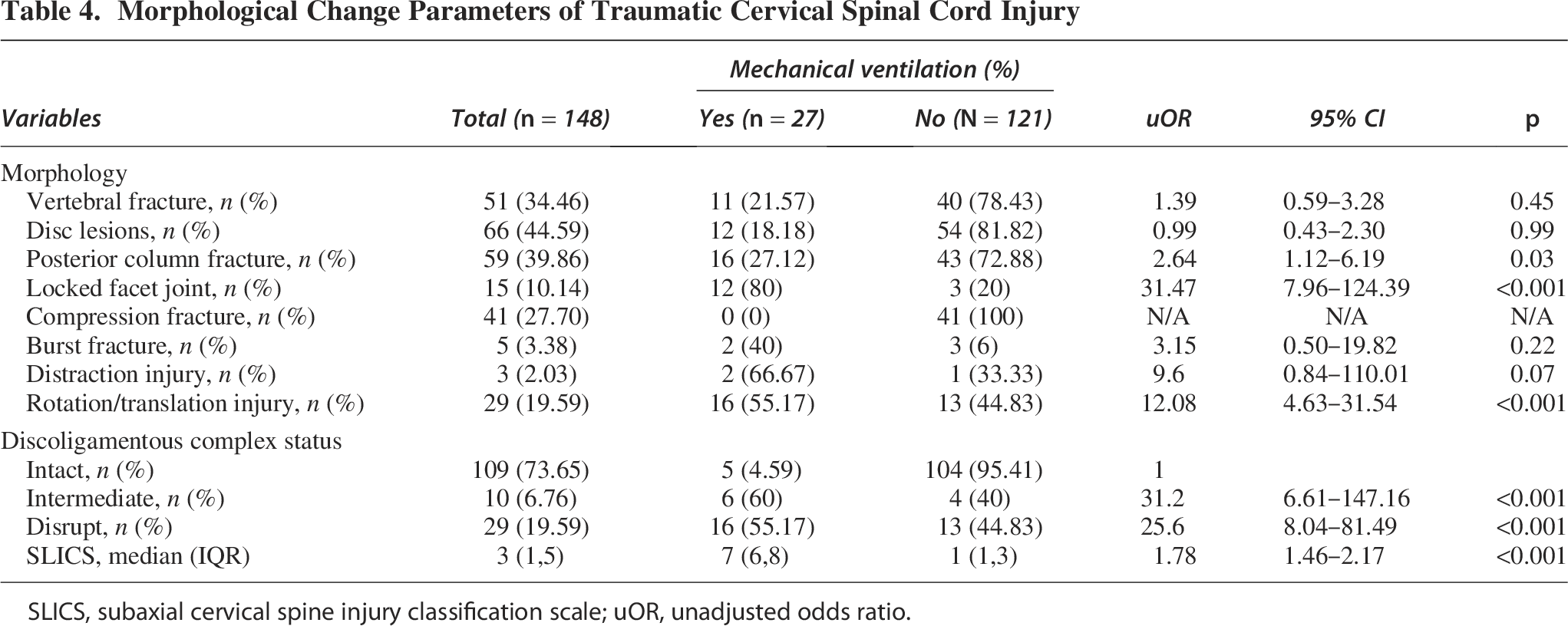
SLICS, subaxial cervical spine injury classification scale; uOR, unadjusted odds ratio.
The forest plot illustrates the standardized coefficients of various variables predicting the need for MV. The variables degree of compression (adjusted odds ratio [aOR]: 10.18; 95% CI: 2.03–50.94; p < 0.001) and cord contusion length (aOR: 2.11; 95% CI: 1.06–4.22; p = 0.03) demonstrated statistically significant associations. Among these, the degree of compression and cord contusion length exhibited the strongest positive associations. Meanwhile, the C2–3 level of injury (aOR: 8.17; 95% CI: 0.59–113.24; p = 0.12), facet joint lock (aOR: 21.18; 95% CI: 0.77–582.31; p = 0.07), and the SLICS score (aOR: 2.50; 95% CI: 0.98–6.37; p = 0.06) showed marginal significance. However, other variables, such as age, posterior column fracture, rotation/translation injury, and DLC status, did not show significant relationships (Fig. 6).

Coefficient plot of the multivariate logistic regression model of factors associated with mechanical ventilation in traumatic cervical spinal cord injury.
The receiver operating characteristic curve reflects the predictive performance of various factors in determining the need for MV. The degree of compression (area under the curve [AUC] = 0.93) and cord contusion length (AUC = 0.88) demonstrate excellent predictive ability, highlighting their strong association with injury severity and the need for MV. The SLICS score (AUC = 0.87) also performs well as a composite measure, making it a practical tool for clinical use. Facet joint lock (AUC = 0.71) shows fair predictive ability, while the C2–3 level of injury (AUC = 0.57) performs poorly, suggesting it is not a reliable predictor and is close to random chance. These findings underscore the importance of prioritizing strong predictors, such as the degree of compression and cord contusion length, in clinical decision-making (Fig. 7).

Receiver operating characteristic analysis was conducted to compare C2–3 level of injury, facet joint lock, degree of compression cord, contusion length, and Subaxial Injury Classification and Severity Scale score (SLICS score).
In patients with compression of grade 2 or higher (>25%) on both CT and MRI, a significant correlation was observed with the likelihood of needing MV support, exhibiting a sensitivity of 81.5% and specificity of 91.7% in CT and sensitivity of 100% and specificity of 68.97% in MRI. Similarly, in patients with a cord contusion length of at least 2 levels by MRI, the potential need for MV support could be predicted with a sensitivity of 81.5% and specificity of 79.2%. The SLICS score showed borderline significance, with a sensitivity of 81.5% and a specificity of 87.6%. Last, facet joint lock demonstrated borderline significance, with a sensitivity of 44.4% and specificity of 97.5%.
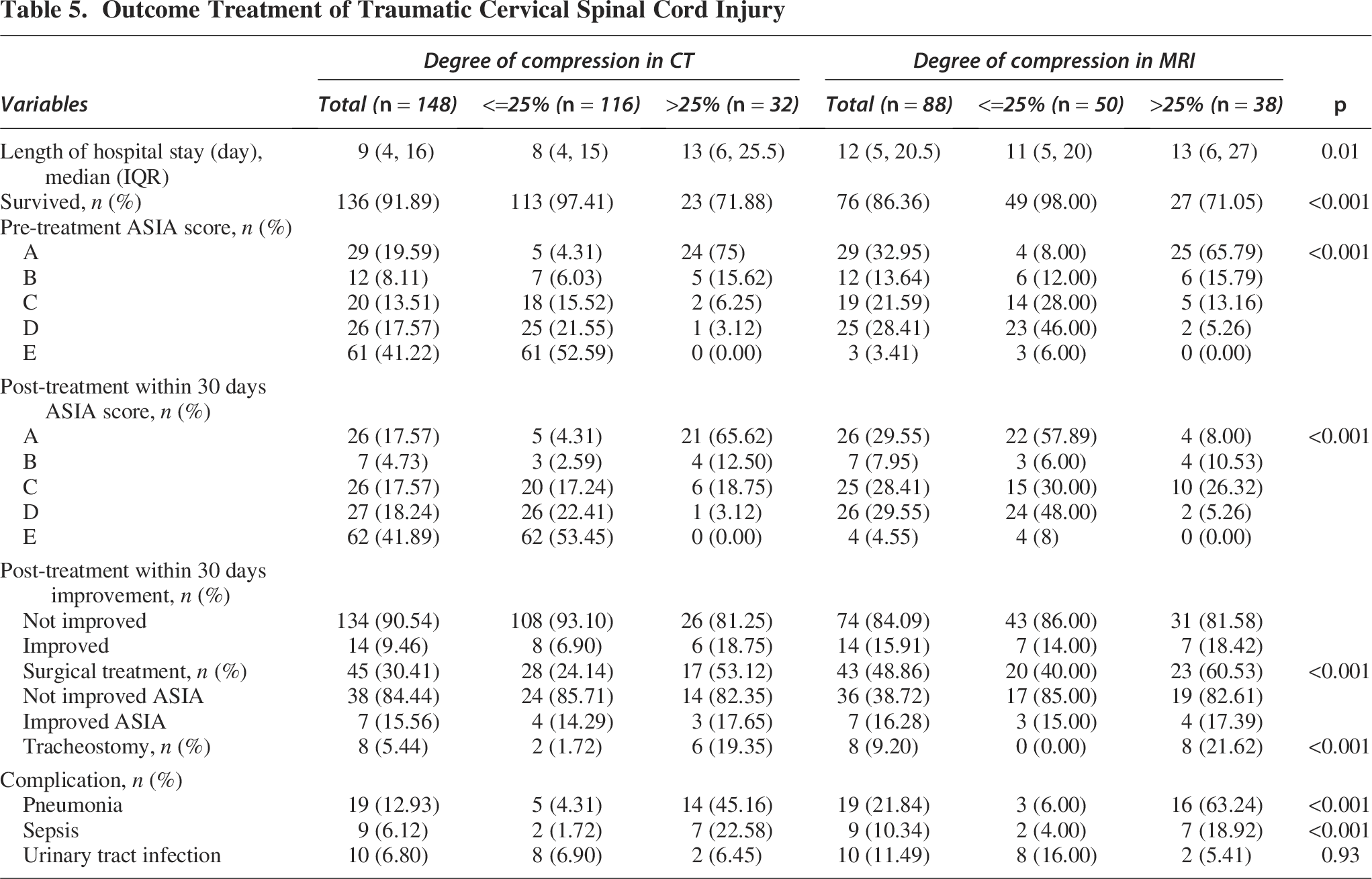
Patients with moderate-to-severe cervical spinal cord compression (≥25%, grades 2–4) had significantly worse outcomes compared to those with mild compression (<25%, grades 0–1), measured by both CT and MRI. These patients had longer median hospital stays (CT: 13 vs. 8 days; MRI: 13 vs. 11 days; p = 0.01), lower survival rates (CT: 71.88% vs. 97.41%; MRI: 71.05% vs. 98.00%; p < 0.001), and higher rates of severe neurological deficits (ASIA A). Additionally, they experienced higher tracheostomy rates and complications, including pneumonia and sepsis. Surgical intervention was more common in grade 2 or more groups (CT: 53.12% vs. 24.14%; MRI: 60.53% vs. 40.00%; p < 0.001). Although post-treatment ASIA score improvement was generally low, patients with ≥25% compression showed slightly higher improvement rates (CT: 18.75% vs. 6.90%; MRI: 18.42% vs. 14.00%), despite worse initial neurological status (Table 5).
Outcome Treatment of Traumatic Cervical Spinal Cord Injury
Discussion
For the comparison of demographic data on acute traumatic cervical spinal injury, the male-to-female ratio in this study was 5.4:1. Similarly, a recent study on TCSCI in Tianjin, China, reported a ratio of 5.6:1 21 , 5.9:1 in India, 22 and 4.7:1 in Norway. 23
In numerous other developing nations, the average age of TCSCI was 50.1 ± 15.5 years in China,21 33.5 ± 13.8 in South Africa, 24 and 31 ± 6 years in Iran. In India, the mean, median, and mode ages were 34.4 25 and 30 years, respectively. 26 The 20- to 40-year age groups were identified as high-risk groups for TCSCI. 27 For instance, the median age was 58 (IQR: 37–72) in the Netherlands,23 42.9 (SD: 21.6) in Norway 28 and 51.3 years (SD: 20.1) in Canada, 29 where the mean age of TCSCI patients was over 40 years. In this study, the mean age was 51.68 ± 15.52, and the median age was 52 (IQR: 40.5–62) which. It is worth noting that the mean age for TCSCI in this study resembled findings from many developed countries.
Lifestyle factors such as smoking and alcohol consumption were not significantly associated with MV. High mechanisms of injury, such as falls from heights, were correlated with significantly higher odds ratios and an increased likelihood of needing MV due to the potential for severe SCI. Conversely, traffic accidents, which can vary in severity, frequently entail motorcycle accidents at low speeds, leading to less severe injuries and lower odds ratios, and therefore not necessitating MV.
The frequency of cervical spinal cord injuries suggests that the predominant sites of injury in the lower cervical region, which lead to instability and necessitate intervention, are at levels C6/7, followed by C5/6 and C4/5. 30 In the present investigation, level C2/3 exhibited fluctuations in load distribution within the ligamentous cervical C2/3 area across various loading conditions. The facet joints, surrounding cancellous bone, and ligaments emerged as the most susceptible structures to rapid flexion—extension, axial rotation, and lateral bending, combined with dislocation or compression. 31 The findings of this study indicated that only the cervical level 2/3 showed significance in the univariate analysis for MV, whereas the remaining cervical levels did not. Phrenic motor neurons, stemming from the cervical C3–C5 nerve roots, are pivotal for diaphragm muscle function. Inspiratory premotor neurons in the ventrolateral and dorsomedial medulla are linked to the phrenic nerve.32–38 Uniform bulbospinal input would make phrenic motor neuron recruitment rely solely on the size-dependent electrophysiological properties of the motor neurons R. 27 Our study analyzed, identified, and presented various parameters in the results, suggesting disrupted presynaptic input to the phrenic nerve due to TCSCI.
The majority of phrenic motor neuron damage is caused by the cervical SCI, leading to significant impairment of diaphragm muscle motor innervation. 39 This inability to maintain adequate ventilation necessitates MV support, a situation associated with substantial morbidity and mortality.40, 41 Spinal cord contusions are the most common type of traumatic SCI, resulting in long-term morbidity and mortality.39 A article introduced a study investigating diaphragm muscle movement by hemisection at the C2 level rostral to the phrenic motor pool in animals, thereby disrupting ipsilateral premotor input to phrenic motor neurons. 42 Despite the presence of a limited number of descending inputs and ascending columns projecting to cervical motor pools, 43 fibers from the contralateral phrenic nerve can still innervate the cervical spinal cord.44–47 Certainly, unilateral denervation of the diaphragm muscle resulting in total unilateral paralysis does not impact the execution of ventilatory behaviors. 48 Phrenic motor neurons exhibit a diverse range of neuronal surface areas, with their inherent excitability determined by their capacitance. 49
The study found that all patients who required MV had cord contusions. Multivariate analysis of cord contusions at various cervical levels revealed that a contusion length of two or more vertebral segments, regardless of the level, was associated with an increased risk of requiring MV.
The degree of stability in spinal column structural injuries, as observed in morphology,31,50,51 and the status of the DLC, 52 was found to be relevant in this study. It was observed that compression fractures were stable and unlikely to result in displacement causing compression of the spinal cord; hence, there was no need for ventilator support among the patients. Nevertheless, burst fractures and distraction injuries increased the odds ratio for instability leading to cord compression, although this did not reach statistical significance for MV. Rotation/translation and the condition of the DLC status substantially elevated the risk of instability and the requirement for ventilator support. In another analysis of morphology, it was observed that nonspecific vertebral body fractures and disc lesions did not exhibit significance among the variables, whereas posterior column fracture and facet joint locking significantly increased the odds ratio.
The SLICS integrates a scoring mechanism intended to assist in determining whether surgical intervention is warranted, shifting from nonsurgical to surgical management. It evaluates spinal column stability across three domains: morphological characteristics, integrity DLC, and the patient’s neurological status. 20 In this investigation, the SLICS scale was computed and shown to have relevance marginally significant to MV.
The stability of the spinal column may serve as an indicator of SCI severity, and this information could provide additional confirmation that the severity of SCI plays a crucial role in elevating the risk of MV. The statistical significance observed in the univariate analysis prompted further investigation through multivariate analysis. This analysis revealed that both the degree of compression and the length of spinal cord contusion independently influenced the need for MV, serving as indicators of the severity of TCSCI.
The strong correlation between CT and MRI findings, along with the noninferiority of CT in predicting the need for MV, suggests that CT can serve as a reliable and practical alternative to MRI for evaluating spinal cord compression. Given CT’s greater accessibility, lower cost, and faster imaging time, it is particularly valuable in acute and resource-limited settings where MRI may be delayed due to factors such as skull traction, transfer difficulties, or prolonged scanning time. These findings have important clinical implications, as relying on CT as a primary diagnostic tool can facilitate faster decision-making and timely intervention, especially for patients at risk of deterioration. Moreover, utilizing CT more effectively can help optimize hospital resources without compromising diagnostic accuracy. While CT and MRI provide comparable assessments of compression severity and predict MV needs with similar accuracy, MRI still offers superior diagnostic detail for evaluating spinal cord contusion, disc pathology, and ligamentous integrity. Notably, patients with moderate spinal cord compression (particularly grade 2) demonstrated better neurological recovery, whereas those with severe compression (especially grade 4) were more likely to require ventilation and showed limited improvement in ASIA classification. This highlights the importance of early identification and intervention, especially in cases with moderate compression where recovery potential is higher. Stratifying patients by compression grade can therefore aid in prognostication and guide individualized treatment strategies.
The observed post-treatment improvement in ASIA scores among patients with a degree of compression of grade 2 or higher suggests that even those with more severe spinal cord compromise may benefit from appropriate interventions, including surgical decompression and intensive supportive care, leading to improved functional outcomes. In contrast, patients with less than grade 2 compression showed limited improvement, likely due to the mild to moderate nature of their deficits, which resulted in minimal or no improvement.
Future research on AI-assisted quantitative assessment of spinal cord compression through CT imaging upon arrival will significantly enhance the evaluation of severity, improve prognosis prediction, guide treatment strategies, and help standardize referral system information. Additionally, prevention is crucial in reducing fall risks among the elderly, as major mechanisms significantly increase the risk of TCSCI, a major concern in aging populations. Simple, accessible, and sustainable prevention programs can effectively decrease falls, improve outcomes, and enhance the quality of life and health care for older adults. It is essential to advocate for the widespread promotion of these programs within aging societies, both now and in the future, to ensure lasting and meaningful improvements in health and well-being for the elderly.
This study is limited by the 30-day follow-up period, as patients are referred to local hospitals for continued physical therapy under the health care system. Nevertheless, the findings have important implications for clinical practice, particularly in neurosurgery and trauma centers. Although CT and MRI did not report the same degree of spinal cord compression—likely due to pathological differences, particularly disc lesions (66 cases, 44.59% in Table 4)—CT still demonstrated noninferiority in predicting the need for MV and the post-treatment functional outcome. This discrepancy arises because CT primarily assesses bony structures and has limitations in evaluating soft tissue lesions, such as disc herniations and ligamentous injuries, which are better visualized on MRI. MRI remains the gold standard for the evaluation of cord contusion, surgical planning, and prognosis prediction in TCSCI. However, CT continues to be a valuable tool for outcome prediction in acute settings, especially when MRI is not readily available.
Conclusion
The need for MV in TCSCI is primarily determined by the severity of the injury. Multivariate analysis identified severe cord compression of at least grade 2 and cord contusion spanning at least two levels as independent predictors of neurogenic respiratory failure, with CT scans serving as a reliable alternative to MRI for evaluating the spinal cord compression grading system. Patients with grade 2 or greater cervical spinal cord compression had significantly poorer outcomes compared to those with less than grade 1 cord compression, including longer hospital stays, lower survival rates, worse pre-treatment neurological status, and higher complication rates. Surgical treatment, particularly the posterior approach, was more common in the grade 2 cord compression group; however, post-treatment neurological improvement was observed only in cases of grade 2 compression, not grade 3 or 4 in CT and MRI. In contrast, the less than grade 1 cord compression group demonstrated better outcomes, with greater post-treatment improvement.
Authors’ Contributions
C.C.: Methodology, software, data curation, writing original draft preparation, and visualization. A.B.: Conceptualization, investigation, supervision, writing original draft preparation, validation, and editing. All authors read and approved the final article.
Footnotes
Author Disclosure Statement
The authors confirmed that there are no potential conflicts of interest regarding the research, authorship, or publication of this article.
Funding Information
The authors did not receive any financial backing for the research, writing, or publication of this article.