
Abstract
Traumatic brain injury with a Glasgow Coma Scale (GCS) score of 3–5 is characterized by severe injury, poor prognosis, and low survival rates. Deciding between aggressive neurosurgery and treatment discontinuation is challenging among older adults. This study analyzed the characteristics, treatment, and outcomes of acute subdural hematoma (ASDH) in older adults with a GCS score of 3–5 to assess the benefits of surgery and guide future treatment decisions. We analyzed the data of 205 older adults (aged 65 years or older) with ASDH and a GCS score of 3–5 registered in the Korean Neuro-Trauma Data Bank System from January 2018 to June 2021. The patients were divided into death and survival groups, and the demographic, clinical, and radiological characteristics; treatment methods; mortality rates; and treatment outcomes were analyzed, along with the relationship between variables and mortality. We also compared the Glasgow Outcome Scale–Extended (GOSE) scores and investigated whether surgical treatment affected mortality and good recovery rates according to age. According to the GOSE, 76.1% of patients died, 12.7% survived in a vegetative state, 3.9% had severe disabilities, and only 4.0% showed good recovery. The GCS score at admission was significantly associated with pupil reactivity; Rotterdam computed tomography score; time interval from injury to operation and arrival to operation; treatment; and hospital stay between patients who died and those who survived. Surgical treatment was significantly associated with a lower mortality rate but not with good recovery rates.
Introduction
Ultra-severe traumatic brain injury (TBI) is a subgroup of severe TBIs, defined as patients with an initial Glasgow Coma Scale (GCS) score of 3–5. 1,2 Although life-sustaining management is taken in the initial treatment, patients in this category are characterized by extremely severe injury, very poor prognosis, and low chances of recovery and survival. Therefore, deciding whether to perform aggressive neurosurgical treatment or discontinue treatment in this condition is one of the most frequently encountered but difficult decisions for physicians. 1,3 –6
Recently, the older adult population has been rapidly increasing worldwide, and Korea is also expected to enter a super-aged society in 2025, with older adults aged 65 years or older accounting for more than 20% of the total population. 7 Since age has been generally recognized as the most important factor in poor prognosis and increased mortality in many studies on TBI, the increase in the older adult population is becoming an increasingly important issue for those managing TBI. 1 –3,5 In particular, clear guidelines are lacking, and various ethical, financial, and cultural issues often arise for this population; hence, careful consideration of multiple factors is required when choosing an appropriate neurosurgical strategy. 1,2,8 In this study, the authors analyzed the current status, characteristics, treatment, and outcomes of geriatric patients with acute subdural hematoma (ASDH) and a GCS score of 3–5, a condition that accounts for a large proportion of TBIs and is associated with a poor prognosis. In addition, the benefits of surgical intervention were evaluated to establish future treatment guidelines for ASDH with a GCS score of 3–5.
Materials and Methods
We analyzed data registered with the Korean Neuro-Trauma Data Bank System (KNTDBS) operated by the Korean Neurotraumatology Society (KNTS) from January 2018 to June 2021. The inclusion criteria were patients with severe TBI, aged 19 years or older, with ASDH, and a GCS score of 8 or less. The exclusion criteria were patients with a history of craniotomy or craniectomy. Eighteen university hospitals in Korea participated in the KNTDBS registry, and 662 patients with ASDH were enrolled. Of these, 250 patients with GCS scores of 6–8, 199 patients aged 19–64 years, and 8 patients with incomplete medical records were excluded, and 205 older adults with ASDH (aged 65 years or older) were analyzed (Fig. 1). Treatment outcomes were assessed using the Glasgow Outcome Scale–Extended (GOSE) after 6 months. The computed tomography (CT) classification used was the Rotterdam CT classification. 9 The patients were divided into death (n = 156) and survival groups (n = 49). The demographics, clinical characteristics, radiological characteristics, treatment methods, mortality rates, and treatment outcomes were compared and analyzed between the two groups. Additional analyses were conducted by dividing the patients into the following age groups: 65–74 years, 75–84 years, and ≥85 years. We analyzed the relationship between key variables (age distribution, sex, treatment, pupil reactivity, and GCS at admission) and mortality and compared GOSE according to subdivisions of key variables. We analyzed whether there were differences in the distribution of GCS scores, surgical rates, and good recovery rates according to the age distribution. In addition, we investigated whether surgical treatment affected mortality and good recovery rates according to the age distribution.

Flow diagram showing the patient selection process.
Statistical analyses
Continuous variables were compared between groups using independent t-tests for normally distributed variables and the Mann–Whitney U test for nonnormally distributed variables. Categorical variables were analyzed using the chi-squared test or Fisher’s exact test when the sample sizes were small. Logistic regression analysis was conducted on significant variables, including sex, age, GCS score, pupil reactivity, and treatment, to evaluate their independent associations with survival outcomes. SPSS (version 22.0; IBM SPSS Inc., Armonk, NY) was used for the statistical analyses. Statistical significance was set at p < 0.05.
Results
Demographic, clinical, and radiological characteristics of patients and their outcomes
Table 1 shows the demographic, clinical, and radiological characteristics of the patients and their outcomes. The mean age was 74.47 ± 7.23 years, and there were more males (n = 128, 62.4%) than females (n = 77, 37.6%). At admission, the GCS score was 3 in 79 patients (38.5%), 4 in 78 patients (38.0%), and 5 in 48 patients (23.4%). Pupil reactivity was most common in bilaterally unreactive pupils (n = 158, 77.1%), followed by reactive pupils (n = 30, 14.6%), unilaterally unreactive pupils (n = 15, 7.3%), and uncheckable pupils (n = 2, 1.0%). The average thickness of hematoma and midline shift on CT were 17.26 ± 7.94 mm and 13.84 ± 8.10 mm, respectively, and the average Rotterdam CT score was 4.84 ± 1.09. The mean time from injury to arrival at the hospital was 156.87 ± 375.77 min, and the mean time from arrival at the hospital to CT scan was 36.01 ± 93.52 min. Eighty-three (40.5%) patients received surgical treatment, and 122 (59.5%) received conservative treatment. As per GOSE, there were 156 deaths (76.1%), 26 vegetative states (12.7%), 6 lower severe disabilities (2.9%), 2 upper severe disabilities (1.0%), 2 lower moderate disabilities (1.0%), 5 upper moderate disabilities (2.4%), 4 lower good recoveries (2.0%), and 4 upper good recoveries (2.0%). Patients were divided into death (n = 156) and survival (n = 49) groups, and the differences between the two groups were compared. There was a statistically significant difference in the two groups in terms of GCS score at admission (p = 0.049), pupil reactivity (p < 0.001), Rotterdam CT score (p < 0.001), time interval from injury to operation (p = 0.020), time interval from arrival to operation (p = 0.001), treatment (p = 0.001), and hospital stay (p < 0.001) (Fig. 2; Table 1). Logistic regression analysis on significant variables associated with mortality included GCS score at admission (odds ratio [OR] 0.6, 95% confidence interval [CI] 0.50–1.82, p = 0.895), medical history (OR 0.75, CI 0.26–2.13, p = 0.584), pupil reactivity (OR 1.05, CI 1.08–3.17, p = 0.024), Rotterdam CT score (OR 0.61, CI 0.39–0.97, p = 0.035), treatment (OR 0.71, CI 0.25–2.02, p = 0.525), and hospital stay (OR 1.12, CI 1.08–1.17, p < 0.001).
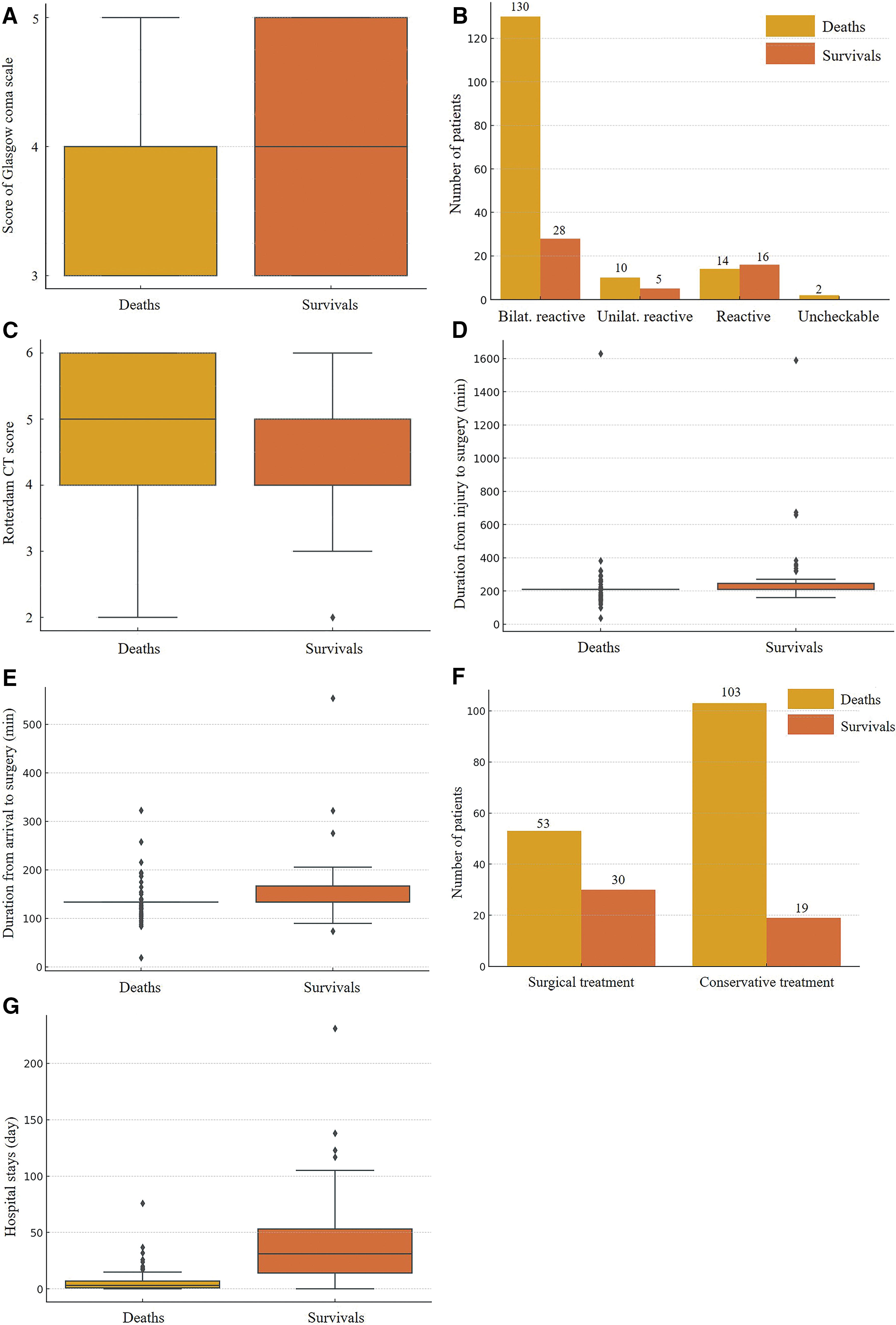
Boxplots and bar charts of significant variables related to death and survival.
Demographic, Clinical, and Radiological Characteristics of Patients with Outcomes
Data are presented as N (%).
Mean ± standard deviation.
BP, blood pressure; CT, computed tomography; GCS, Glasgow Coma Scale score; GOSE, Glasgow Outcome Scale–Extended; NA, not available.
Mortality and Glasgow Outcome Scale–Extended by variables
Table 2 shows mortality and GOSE scores for the subdivisions of the key variable. The mortality rate was 73.9% for those aged 65–74, 78.3% for those aged 75–84, and 80.0% for those aged 85 or older, showing an increasing trend in mortality with increasing age, but the difference was not statistically significant (p = 0.709). The mortality rate was 74.2% in men and 79.2% in women, with no significant difference (p = 0.406). However, the mortality rate in the surgical treatment group was 63.9%, and that in the conservative treatment group was 84.4%, which was significantly higher in the conservative treatment group (p = 0.001). For pupil reactivity, the mortality rate was 82.3% in the bilateral unreactive pupil, 66.7% in the unilateral reactive pupil, and 46.7% in the reactive pupil, and this difference was statistically significant (p < 0.001). Regarding the GCS score, the mortality rate was 82.3% for GCS 3, 75.6% for GCS 4, and 66.7% for GCS 5, indicating that the mortality rate decreased as the GCS score increased; however, the differences were not statistically significant (p = 0.134).
Mortality and Glasgow Outcome Scale–Extended by Variables
Data are presented as N (%).
(%): mortality of subdivision.
*p < 0.05, indicating statistical significance between variables and death.
LG, lower good recovery; LM, lower moderate disability; LS, lower severe disability; UG, upper good recovery; UM, upper moderate disability; US, upper severe disability; VS, vegetative state.
Comparison of mortality, GCS score, surgery, and good recovery rate by age group
Table 3 shows the comparison of mortality, GCS score, surgery, and good recovery rate by age distribution. Good recovery includes lower and upper good recovery in GOSE. In the 65–74 age group, GCS scores of 3, 4, and 5 were 48 (43.2%), 36 (32.4%), and 27 (24.3%), respectively. In the 75–84 age group, they were 23 (33.3%), 31 (44.9%), and 15 (21.7%), respectively, and in the ≥85 age group, they were 8 (32.0%), 11 (44.0%), and 6 (24.0%), respectively. However, there was no significant difference between age distribution and GCS score (p = 0.472). Forty-seven patients in the 65–74 age group (42.3%), 30 patients in the 75–84 age group (43.5%), and 6 patients in the ≥85 age group (24.0%) underwent surgery. However, there was no significant difference in the surgery rate by age distribution (p = 0.198). Good recovery was shown by six patients (5.4%) in the 65–74 age group, one patient (1.4%) in the 75–84 age group, and one patient (4.0%) in the ≥85 age group. There was also no significant difference in good recovery by age distribution (p = 0.411).
Comparison of GCS Score, Surgery, and Good Recovery Rate by Age Group
Good recovery includes lower good recovery and upper good recovery on the Glasgow Outcome Scale–Extended.
Mortality and good recovery rate by age group and treatment
Table 4 shows mortality and good recovery rate by age distribution and treatment. In patients aged 65–74, there were 30 deaths (63.8%) and 4 good recoveries (8.5%) in the surgical group and 52 deaths (81.3%) and 2 good recoveries (3.1%) in the conservative group. Surgical treatment was significantly associated with a lower mortality rate (p = 0.039), but good recovery did not show any significant difference with mortality (p = 0.215). In patients aged 75–84 years, there were 21 deaths (70.0%) and 0 good recovery in the surgical group, and 33 deaths (84.6%) and 1 good recovery (2.5%) in the conservative group. Thus, surgical treatment was not significantly associated with mortality and good recovery rates (p = 0.145 and p = 0.377, respectively). In patients aged 85 years or older, there were 2 deaths (33.3%) and 1 good recovery (16.7%) in the surgical group, and 18 deaths (94.7%) and 0 good recovery in the conservative group. Thus, surgical treatment was significantly associated with a lower mortality rate (p = 0.005) but not with good recovery (p = 0.240).
Mortality and Good Recovery Rate by Age Group and Treatment
Good recovery includes lower good recovery and upper good recovery on the Glasgow Outcome Scale–Extended.
Treatment and death.
Treatment and good recovery.
*p < 0.05, indicating statistical significance between treatment and death, as well as between treatment and good recovery.
Discussion
In cases of ASDH with clear signs of increased intracranial pressure, surgical treatment to remove the hematoma via rapid craniotomy or craniectomy is the principle. However, in the case of ASDH patients with a GCS score of 3–5, the mortality rate is very high, and even if they survive, the recovery rate is very low; moreover, many survivors are likely to live in a vegetative state or a state of severe long-term disability. 3 –6 When ASDH with a GCS score of 3–5 occurs, the decision about whether to perform surgical treatment is typically left to surrogate decision-makers, such as family members or legally appointed representatives. 10 For a surrogate to make life-or-death treatment decisions on behalf of an unconscious patient, the physician must understand and be able to fully explain to the surrogate(s) the diagnosis, treatment, and prognosis related to ASDH with a GCS score of 3–5. However, it is difficult to predict which patients will survive and which patients who survive will have long-term severe disability or functional improvement. 11 Providing appropriate management in the acute phase is one of the most difficult decisions for physicians, as not only are there complexities related to prognostic uncertainty but also the level of support from families who can care for patients with severe disabilities can be an important variable. 10
Although the importance of age, GCS score, pupillary reaction, extracranial injuries, surgical intervention, and radiological findings has been studied to predict outcomes, selecting patients who can be considered for neurosurgical intervention by predicting good outcomes remains a challenge. 12,13 Among the important factors predicting outcomes, age is closely associated with poor prognosis and increased mortality after TBI. In fact, older patients have higher mortality and worse prognosis regardless of the intervention performed, and several studies on TBI have shown that age may be the most important factor in predicting prognosis. 3,5,6,13 Shimoda et al. 3 retrospectively analyzed 888 patients with geriatric TBI, registered in the Japan Neurotrauma Data Bank, and found that neurosurgical management was associated with improved prognosis and reduced mortality in patients aged 65 years or older with geriatric TBI. In particular, surgery has been shown to improve the prognosis and mortality of older adults with a GCS score of 6–15 due to ASDH. Additionally, older patients who underwent surgery within the first 4 h after TBI had a higher incidence of favorable outcomes. However, in older adults with GCS scores of 3–5, surgical management resulted in “useful” recovery in only about 4% of the cases, and death occurred in more than 87% of the cases regardless of management. Although age alone should not be used as a contraindication to surgery in patients with TBI aged 65 years or older, the authors argued that because surgical management has not been shown to be an effective treatment option in patients with a GCS score of 3–5, these data should be discussed with the family before surgery whenever possible. 3 Their study also supports previous reports that the prognosis for older adult patients with severe TBI is dismal, and mortality rates increase dramatically with age. Jamjoon et al. 6 reported on 11 patients with a mean age of 73 years and a GCS score of 3–5. All the patients died at the hospital. Pennings et al. 14 reported on 42 patients with a mean age of 74 years and a GCS score of 3–5; at the 4-month follow-up, they also reported a mortality rate of 91%. In a study of patients with TBI aged 65 years and older, Kilaru et al. 5 reported in-hospital mortality of 100% in patients with an admission GCS score of 3; for patients with an admission GCS score of 4 or 5 (n = 7), most died (n = 5), and all survivors (n = 2) remained in a vegetative state. They also found that older adult survivors of severe TBI showed little neurological improvement over time. Thus, a low GCS score appeared to be the strongest adverse predictor of mortality in older adults with ASDH.
In this study, the mortality rate of patients aged 65 years or older with ASDH and a GCS score of 3–5 was 76.1% (n = 156), and good recovery was 4% (n = 8). The combined rate of vegetative state and severe disability was 15.6% (n = 32), indicating that many survivors remained in a vegetative state or had severe disability. The mortality rate in the surgical group (63.9%) was significantly lower than that in the conservative group (84.4%), suggesting that surgical treatment is an important factor in improving survival. Although this finding may appear clinically useful, it must be interpreted with caution. Typically, patients who undergo surgical treatment receive more aggressive treatments than those who undergo conservative treatment. Previous studies have reported that patients who underwent surgery received much more intensive management, including intracranial pressure monitoring and therapeutic hypothermia, which may be associated with more favorable outcomes and lower mortality rates than patients who did not undergo surgery. 3,15 In contrast, in the group that received conservative treatment, there were many cases where family members or surrogates refused to allow the patient to survive in a vegetative or severely disabled state or refused active treatment for various economic, religious, or personal reasons. Older adults are more likely to refuse aggressive surgical treatment than younger patients, which may lead to poorer prognosis and higher mortality. Previous studies have shown that the treatment intensity provided to older adults with TBI is lower than that provided to younger patients with TBI. 16
In our study, the vegetative state rate was 53.1% (n = 26), severe disability rate was 16.3% (n = 8), and good recovery rate was 4% (n = 8) among the 49 survivors in total. Among the 30 survivors in the surgical treatment group, 53.3% (n = 16) were in a vegetative state, 16.7% (n = 5) had severe disability, and 16.7% (n = 5) showed good recovery. Among the 19 survivors in the conservative treatment group, 52.6% (n = 10) were in a vegetative state, 15.7% (n = 3) had severe disability, and 15.7% (n = 3) showed good recovery (Table 2). These results imply that surgical treatment significantly improved survival rates, but there was no difference in treatment outcomes compared to conservative treatment. Although there was no significant difference, surgical treatment increased not only good recovery but also the rates of vegetative state and severe disability. Shimoda et al. 3 argued that surgical treatment is not justified and is not cost-effective for older adults with TBI with a GCS score of <5. In addition, Kotwica and Jakubowski 4 analyzed 136 patients with TBI aged 70 years or older and reported that all but one patient with a persistent vegetative state died among 24 patients with GCS scores of 3–5, regardless of whether surgery was performed, suggesting that treatment should be limited in this group of patients. In our study, surgical treatment was performed in 40.5% of patients aged 65 years or older despite having a GCS score of 3–5, a rate higher than expected; this may be because the investigation was limited to ASDH.
In Korea, the law on death with dignity was first implemented in 2018, and the total number of people who refused life-sustaining treatment and died between 2019 and 2023 was 327,097. The number of people who wrote an advance directive before they got sick, stating that they do not want life-sustaining treatment, was 2,441,805 as of June 2024. 7 As of October 2024, one in five people over the age of 65 have written an advance directive stating that they want to preserve their dignity at the end of their lives. Therefore, the cessation of life-sustaining treatment will become more common in the future. This change in perception shows that the value of the quality of life has increased in present times. This aligns with the fact that the treatment goal for patients with severe brain damage is to restore a good quality of life for them rather than simply preserve life. Although each individual’s quality of life is subjective, diverse, and variable, it is important to deeply consider whether the vegetative state is what the patient or their family wants. 11 Vegetative state refers to a clinical condition where a patient is awake but not aware of themselves or their environment. While they may have sleep–wake cycles, open their eyes, or display reflexive movements, there is no evidence of conscious awareness or purposeful response to stimuli. The vegetative state typically follows severe brain injury, and if it persists beyond a certain period (usually around 4 weeks), it is termed a “persistent vegetative state,” 17 in which there is very little chance of improvement even with sufficient time, especially in older adults. If the prediction of poor outcomes is extremely high, the discussion of surgical decompression cannot be simply a matter of life and death. This is because the long-term outcomes of patients who survive after surgery and the burden-to-benefit ratio imposed on them and their families are very high. 11
According to the current Korea’s Life-Sustaining Treatment Decision Act, if two doctors determine that a patient has no possibility of recovery and is in the terminal stage, the patient is classified as being in the “end-of-life process,” and the intention to discontinue life-sustaining treatment is confirmed. This decision is made by consulting either the patient or their family. If an advance directive has been written, the doctor can verify it and discontinue life-sustaining treatments such as cardiopulmonary resuscitation, hemodialysis, chemotherapy, and mechanical ventilation. 7 If there is no advance directive, life-sustaining treatment can only be discontinued if the patient, while still conscious, has written a life-sustaining treatment plan. In cases where the patient is unconscious and no advance directive exists, the intention to discontinue life-sustaining treatment is determined through either a statement from at least two family members or a consensus among the patient’s family. 7 Therefore, Korea’s Life-Sustaining Treatment Decision Act is unlikely to cause any significant bias or distortion in treatment choices.
Study limitations
This study was a multicenter retrospective analysis conducted across 18 hospitals and has several limitations. First, although detailed data registration instructions were provided to each hospital’s registrar to enhance data quality and consistency, variability in treatment processes and decision making across hospitals was not accounted for. Outcomes may differ depending on factors such as the hospital’s resources, size, and individual circumstances, including the surgeon’s philosophy, surgical expertise, and experience in critical care; however, these variables were not investigated. Additionally, patient-specific factors such as personal circumstances or social conditions (e.g., economic or educational level) were not investigated. Second, this study lacks an investigation of specific treatment processes essential for managing critically ill patients, such as intensive care unit protocols, intracranial pressure monitoring, and daily therapy intensity level. Third, patients with a history of previous craniotomy or craniectomy were excluded from registration during the KNTS second project. 18 However, this exclusion may introduce selection bias and limit the generalizability of our findings, particularly for patients with a history of previous neurosurgical procedures. Our results may not be fully applicable to this subgroup, as their clinical trajectories and outcomes may differ from those without prior surgery. Recognizing this limitation, future studies, including the planned third project, will consider incorporating this patient population to further investigate their unique clinical characteristics and treatment outcomes.
Conclusion
Among patients with ASDH aged 65 years or older and with a GCS score of 3–5, those who received surgical treatment had a higher survival rate than those who received conservative treatment. However, there was no difference in the outcome of treatment compared to conservative treatment, and many patients survived in a vegetative state or with severe disability. Therefore, in the treatment of older adults with ASDH and a GCS score of 3–5, the benefit of surgical intervention is limited to improving survival rates. The findings of this study will contribute to understanding patient prognosis and supporting rational decision making. In the future, these findings will be helpful in establishing treatment guidelines for ASDH in patients with a GCS score of 3–5.
Transparency, Rigor, and Reproducibility Summary
The KNTS established the Korean Neuro-Trauma Data Bank Committee and developed the KNTDBS in 2006. 19 Since then, KNTS has carried out two trauma-related data registration projects. 18,20 The KNTS registered data for the second project from January 2018 to June 2021 through the KNTDBS. 20 Data from the second project were registered into seven major categories: patient registration, neuroimaging, neuromonitoring, hypothermia, surgical treatment, medical treatment, and patient evaluation. A total of 14 data committee members, consisting of neurosurgeons from each University Hospital nationwide, were part of this project. To improve data quality and uniformity, detailed data registration guidelines were established and provided to the person in charge of registration at each hospital. The inclusion criteria were (1) patients who visited the hospital owing to TBI, (2) severe TBI patients with a GCS score of 8 or lower, and (3) adult patients aged 19 years or older. Exclusion criteria were (1) patients under 18 years of age, (2) patients with a GCS score of 9 or higher, and (3) patients with a history of previous craniotomy or craniectomy. A total of 1,109 TBI patients were registered from 18 hospitals. 19 This study was conducted retrospectively by analyzing extracting data registered in the KNTDBS for the second project. Patient registration was approved by the ethics committees of each 18 hospitals. This study received Institutional Review Board approval, and the requirement to obtain informed consent from patients was waived. Additionally, this study was approved by the ethics committee of our University Hospital.
Footnotes
Acknowledgments
This article was supported by Wonkwang University in 2025. The authors are thankful to members of the KNTDB investigators: Jung Hwan Lee (Pusan National University Hospital), In Bok Chang (Hallym University Sacred Heart Hospital), Tae Seok Jeong (Gil Medical Center), Eun Sung Park (Wonkwang University Hospital), Jong Yeon Kim (Wonju Severance Christian Hospital), Min Kyun Na (Hanyang University Medical Center), Jeong Ho Lee (Daegu Fatima Hospital), Kwang Wook Jo (Bucheon St. Mary’s Hospital), Han Seung Ryu (Chonnam National University Hospital), Kyung Hwan Kim (Chungnam National University Hospital), Yu Deok Won (Hanyang University Guri Hospital), Min Su Kim (Ulsan University Hospital), Jin Gyu Choi (Yeouido St. Mary’s Hospital), Sae Min Kwon (Keimyung University Hospital), Jae Sang Oh (Soonchunhyang University Hospital), and Soon O. Hong (Seoul Medical Center).
Authors’ Contributions
K.S.E. made substantial contributions to the conception and design of study, data acquisition, and data analysis and interpretation. Members of the KNTDB investigators contribute to data acquisition. K.S.E. has also been involved in drafting and revising the article.
Author Disclosure Statement
The authors have no competing interests to disclose.
Funding Information
There was no funding provided for this study.