
Abstract
High-level spinal cord injury (SCI) often disrupts supraspinal control of sympathetic input to the heart. The resulting imbalance in the autonomic nervous system increases the risk of developing cardiac arrhythmias. It was previously demonstrated that passive hindlimb cycling (PHLC) effectively maintains or improves bodily function including cardiovascular performance following SCI. However, it remains unclear whether the exercise can affect cardiac electrical disorders. To address this specific question, we complemented a complete SCI at a high-thoracic level in rats and then performed PHLC for 5 or 10 weeks. Naive rats or those receiving injury alone served as controls. Subsequently, a telemetric transmitter was implanted to record blood pressure and electrocardiogram. In 24-h resting recordings, cycling training did not influence SCI-induced hypotension but significantly reduced the events of spontaneous autonomic dysreflexia. When colorectal distension was employed to artificially trigger autonomic dysreflexia, a fewer number of severe arrhythmias (e.g., atrioventricular block, premature ventricular contraction single, and sinus pause) were found in animals with 10-week PHLC compared with injury controls. As a stress test, a series of increasing concentrations of dobutamine was administered to stimulate cardiac sympathetic activity. Consequently, various types of arrhythmias occurred in animals with SCI alone, whereas very few were detected in animals obtaining exercise training for 10 weeks. Furthermore, pharmacological intervention disclosed that exercise appeared to reduce unopposed parasympathetic tone that arose post to injury. Thus, the results suggest that activity-based training for the long term improves autonomic balance to enhance tolerance of cardiac electrical conduction following SCI.
Introduction
The autonomic nervous system regulates cardiovascular activity. Most blood vessels receive predominantly sympathetic innervation, while the heart has input from both sympathetic and parasympathetic divisions. Following traumatic spinal cord injury (SCI), interruption of supraspinal vasomotor pathways (decentralization) reduces sympathetic regulation and results in cardiovascular disorders, including low blood pressure at rest, orthostatic hypotension, and bouts of life-threatening autonomic dysreflexia. 1
The sympathetic system increases heart rate (HR) and contractility, whereas the parasympathetic system decreases HR and relaxes the myocardium. Under normal conditions, the balance between sympathetic and parasympathetic activity maintains proper cardiac performance. After high-level SCI, supraspinal regulation of cardiac sympathetic tone is disrupted, while cranial parasympathetic pathways (vagal) remain intact. Consequently, reduced sympathetic and unopposed parasympathetic activity shifts cardiac regulation out of balance, leading to a higher risk for cardiac disorders. 2 During the acute phase, symptoms manifest as various arrhythmias since cardio-electric transduction is compromised.3,4 Although cardiac arrhythmias are infrequently observed at rest in the chronic phase, the heart is vulnerable to specific provocations when individuals with SCI are exposed to increased heart stress or burden, such as urodynamic examinations, 5 penile vibratory stimulation for ejaculation, 6 and tracheal intubation before surgery. 7 This is possibly due to the occurrence of autonomic dysreflexia during these scenarios.
Detrimental autonomic dysreflexia, which is defined by episodic hypertension and baroreflex-mediated bradycardia, can occur more than 40 times per day and cause debilitating damage to vasculature.8,9 If left untreated, it may give rise to seizures, cerebral hemorrhaging, and ultimately, death. In the clinic, there is no definitive intervention for this disease. Previous studies in SCI rats and humans have shown that repetitive and severe autonomic dysreflexia impairs left ventricle contractility because of high blood pressure. 10 This can progressively develop into myocardial infarction and cardiac failure. Despite the fact that cardiac disorders are acknowledged in patients with SCI, very few animal studies have been implemented to model this ailment and test potential therapeutic approaches. 11 Recently, we employed a complete spinal cord crush injury at the T2/3 level in rats, which partially disrupted supraspinal regulation of sympathetic activity to the heart, and successfully established a reliable model for cardiac disorders. 12
Exercise training after SCI promotes central neuronal plasticity and prevents peripheral atrophy. Numerous investigations have demonstrated that exercise is advantageous at both cellular and biomedical levels for neuroprotection, regeneration, and rehabilitation. As a noninvasive treatment, exercise maintains physical fitness and passively, or actively, provides rhythmic stimulation not only to affected regions of the spinal cord but the whole body by reducing inflammation, preserving muscle mass, 13 inducing synaptic plasticity, 14 and restoring motor and sensory function.15,16 Passive hindlimb cycling (PHLC) is an effective, low-cost, practical, alternative exercise modality for populations with SCI. Previous studies reported that (PHLC) increases levels of endogenous neurotrophic factors in the spinal cord, such as nerve growth factor (NGF), glial cell-line derived neurotrophic factor (GDNF), and neurotrophin-3/4 (NT-3/4), which likely facilitates axon elongation, synaptic activity of regenerating axons, and plasticity of spinal interneurons below the level of injury.17,18 The mechanisms beneath the effects of exercise have been identified to activate phosphatase and tensin homolog (PTEN)/mammalian target of rapamycin (mTOR) signaling pathways in propriospinal neurons. 19 In the cardiovascular system, exercise intervention has obvious clinical implications for preventing the deterioration of the organs among the SCI population. It appears that activation of skeletal muscle activity and increased venous return provide a potent stimulus for cardiac and vascular adaptations.20,21 Recent studies indicate that PHLC in rats with acute SCI reverses the rapid onset of cardiac dysfunction and improves arterial function.22,23 In both human patients and SCI animal models, it was demonstrated that exercise training can improve hemodynamics and the incidence of spontaneous autonomic dysreflexia events.4,23,24 Generally, the advantage of passive exercise is its non-invasive and economical feature that is suitable for patients with limited lower extremity function. The goal of this study is to examine the effects of PHLC on the susceptibility of cardiac electric disorders following SCI.
Materials and Methods
Animals
Adult female Fisher 344 rats (150–200 g, 2–3 months, Envigo) were used for experimentation. The animals were housed in micro-isolator cages in a light and temperature-controlled room. All rats for this study were cared for and treated according to the Institutional Animal Care and Use Committee and Society for Neuroscience guidelines. Animals were divided into four groups: (1) SCI with 10 weeks of exercise (PHLC 10wks, n = 10), (2) SCI with 5 weeks of exercise (PHLC 5wks, n = 10), (3) SCI only (Injury, n = 9), and (4) naive control (n = 7).
Spinal cord injury and Basso, Beattie, and Bresnahan test
Rats were anesthetized by inhalation of 4% isoflurane and maintained by inhalation of 2% isoflurane for the remaining surgery. Rats were placed on the surgical station in the prone position. A midline incision was made to the skin between T1 and T4. The muscle and connective tissue were moved aside using tissue separators to expose the T2 vertebrae. Then, a T2 laminectomy was performed to remove the dorsal part of the vertebrae and the spinal cord was completely crushed between the second and third thoracic level (T2/3) using fine forceps as previously described. 25 Afterward, the muscle and skin were closed with a 4-0 suture. Postoperative care included subcutaneous injections of Lactate Ringer’s (3 mL), cefazolin (10 mg/kg), and Buprenex (0.035 mg/kg) once following injury. Manual bladder expression was performed three times per day for the first 2 weeks and later twice per day until sacrifice. Animals were given 5 days to recover before initiating exercise experiments.
As an exclusion criterion and simple examination of hindlimb motor function, Basso, Beattie, and Bresnahan (BBB) testing was performed weekly following injury until telemeter implantation. In the test, each rat was observed in an open field for 4 min to evaluate hindlimb motor function. Locomotor function was graded on a 0–21-point scale. Within the first 3 weeks post-injury, if a rat received a score greater than 3 exhibiting extensive movement of two joints in the hindlimb, it often indicated incomplete injury and tissue sparing in the lesion. The animal was then excluded from further experiments (n = 2).
Passive hindlimb cycling
Five days after injury, animals began PHLC training. The exercise was performed 5 days a week for 30 min (at a rate of 45 rpm) per session or each day using a custom-made ergometer. For each training session, animals were placed in a horizontal position on a leather sling with two large openings for the hindlimbs to be placed through. The animal’s abdomen was fastened to the apparatus with Velcro straps and the feet were gently secured to the peddles with medical tape, as previously described. 13 To examine the possible distinct effects of exercise with different durations (short or long term) on cardiac conduction disorders, PHLC was conducted for either 5 or 10 weeks after SCI.
Telemeter implantation
Following the completion of exercise (6–11 weeks following injury), animals were anesthetized again with isoflurane and placed on a surgical station with a supine position. A midline incision was performed to access the abdominal cavity. Gauze and tissue separators were used to push aside intestine organs and expose the descending aorta. Subsequently, the catheter of an HD-S11 radio telemetric device (DSI) was threaded into the descending abdominal aorta, and the insertion site was sealed with tissue glue. The intestinal organs were situated back into place, and the telemeter body was sutured to the abdominal wall. The electrocardiogram (ECG) electrodes were subcutaneously placed onto chest muscles using an electrode guide. The positive lead was placed on the lower chest and the negative lead on the upper chest and then sutured to the muscle. After completion of electrode placement, the muscle and skin were sutured closed. Postoperative care was performed as described above. Animals were given 1 week to gain hemodynamic recovery before starting physiological recordings. 26
Twenty-four-hour hemodynamic recordings
Before the start of each experiment, each radio transmitter was paired to a single receiver pad. To record hemodynamic parameters, animals were placed on receivers (PRC-1) and the transmitter was turned on with a magnet. The parameters were recorded using the Ponemah software (v6.3, DSI).
Resting blood pressure, such as mean arterial pressure (MAP), systolic blood pressure (SBP), and diastolic blood pressure (DBP), was recorded for 24 h. The logging rate (sampling) for this experiment was set to record every 20 sec. It was important to note that there were fluctuations in blood pressure and HR over the 24-h period that were thought to reflect diurnal activity. 27 Accordingly, data collected were analyzed based on daytime and nighttime cycles to observe diurnal rhythms in blood pressure and HR. In each rat, the parameters were consistently analyzed in 3-h periods at specific times, day (3:00 pm to 6:00 pm) and night (11:00 pm to 2:00 am) for statistical comparison between groups.
The number of spontaneous autonomic dysreflexia episodes during the 24-h period was examined using a specialized algorithm program in MatLab (MathWorks). 28 This detected events based on abnormal increases in MAP and accompanied by a decrease in HR. Episodes were characterized by increases in MAP from baseline Tp = 15 mmHg and HR decreases Th = 15 bpm within the event interval.
Colorectal distension-induced autonomic dysreflexia
Animals were lightly restrained with a tower and placed on the receiver pad. To induce viscero-sympathetic reflexes, a lubricated latex balloon-tipped catheter, which was attached to a syringe, was inserted approximately 2 cm into the rectum. Animals were then given approximately 15 min to rest, which allowed for hemodynamic parameters to stabilize before beginning experimentation. Subsequently, a volume of 1.4 mL of air was injected into the balloon and held for 1 min ECG, and blood pressure was recorded 1 min before, during, and after colorectal distension (CRD) induction. 29 The procedure was performed twice for each animal with at least 15-min interval, and the values were averaged for statistical analysis. The severity of the CRD-induced autonomic dysreflexia events was assessed based on the changes in MAP and HR. The types and occurrence of various arrhythmias during CRD were analyzed using the Data Insights plugin (DSI). In our observation, many benign arrhythmias, such as junctional arrhythmias, could emerge in healthy subjects, while severe electrical conduction disorders rarely occur. Therefore, we count the number of severe arrhythmia including atrioventricular (AV) block, single premature ventricular contraction (PVC single), and sinus pause. The sum of these three arrhythmias in each rat was used for statistical comparison.
Dobutamine test
To assess the susceptibility of cardiac electrical disorders under stress, animals were intravenously (i.v.) administered with dobutamine (DOB), a β1-receptor agonist, that mimics stress to stimulate cardiac sympathetic activity. Previous studies reported DOB test is a useful tool for investigating sympathetic activation on the occurrence of cardiac arrhythmias. 30 Under isoflurane anesthesia, a butterfly needle attached to a catheter was inserted into the tail vein. Animals were then disconnected from isoflurane, put into restraining tubes, and placed on the receiver pads. After approximately 1 h, awaken rats were administered with DOB i.v. in a series of increasing concentrations (5.0, 12.5, and 20 µg/[kg·min]) using a syringe pump, as previously described. 24 Each dose was injected over 4 min at a volume of 100 µL saline and injections were continuous. The types and occurrence of various arrhythmias during CRD were analyzed using the Data Insights plugin. The number of three severe arrhythmias, described above, was counted. The sum of them in each rat was used for statistical analysis.
Pharmacological interventions to assess autonomic tone
The cardiac autonomic tone was assessed in conscious, freely moving rats using pharmacological manipulations. 31 Before drug administration, a 30-min basal HR and MAP recording was performed to ensure stable conditions. The muscarinic-cholinergic receptor antagonist, atropine (3 mg/kg), was used to block cardiac parasympathetic activity. The β1-adrenergic receptor antagonist, metoprolol (10 mg/kg), was used to block cardiac sympathetic activity. The drug doses for the sympathetic and parasympathetic antagonists were calculated according to each animal’s body weight on the day of each experiment. To assess sympathetic tone, atropine was first injected intraperitoneally (i.p.), and effects were recorded for 15 min. Subsequently, metoprolol was administered, and HR was recorded for 20 min. For analysis, HR was averaged over the last 5 min of either atropine or metoprolol. Intrinsic HR (HRI) was defined as the HR under both atropine and metoprolol administration. The sympathetic tonus was calculated as HRM-HRI, where HRM represents HR under muscarinic blockade. On a separate day, the order of the drugs was reversed, metoprolol then atropine, to assess parasympathetic tone. The parasympathetic tone was calculated as HRβ-HRI, where HRβ represents HR following β1 receptor blockade. The results from both tests allowed us to ascertain how therapeutic intervention affects autonomic regulation after SCI.
Statistical analysis
Basal hemodynamic parameters were analyzed using a one-way or two-way analysis of variance (ANOVA) followed by Tukey’s post hoc. The number of spontaneous autonomic dysreflexia and arrhythmia was analyzed using a non-parametric Kruskal–Wallis test followed by Dunn’s post hoc. Pharmacological assessment of autonomic tone was analyzed using a one-way ANOVA with Tukey’s post hoc.
Results
Resting hemodynamics
Hemodynamic parameters were measured and separately analyzed according to diurnal and nocturnal rhythms. A complete SCI at the level T2/3 resulted in a significant decrease in MAP, SBP, and DBP compared with naive animals during either daytime or nighttime (Fig. 1A–C). Regardless of exercise intervention, there was no apparent improvement in these parameters during diurnal rhythm, while MAP and DBP during nocturnal rhythm were higher in animals receiving 10-week PHLC compared with animals receiving 5-week PHLC (both p < 0.01, two-way ANOVA followed by Tukey’s post hoc). However, both improvements did not differ from the injury control or reach the level in naive rats. In addition, HR was not affected by the injury or exercise (Fig. 1D).
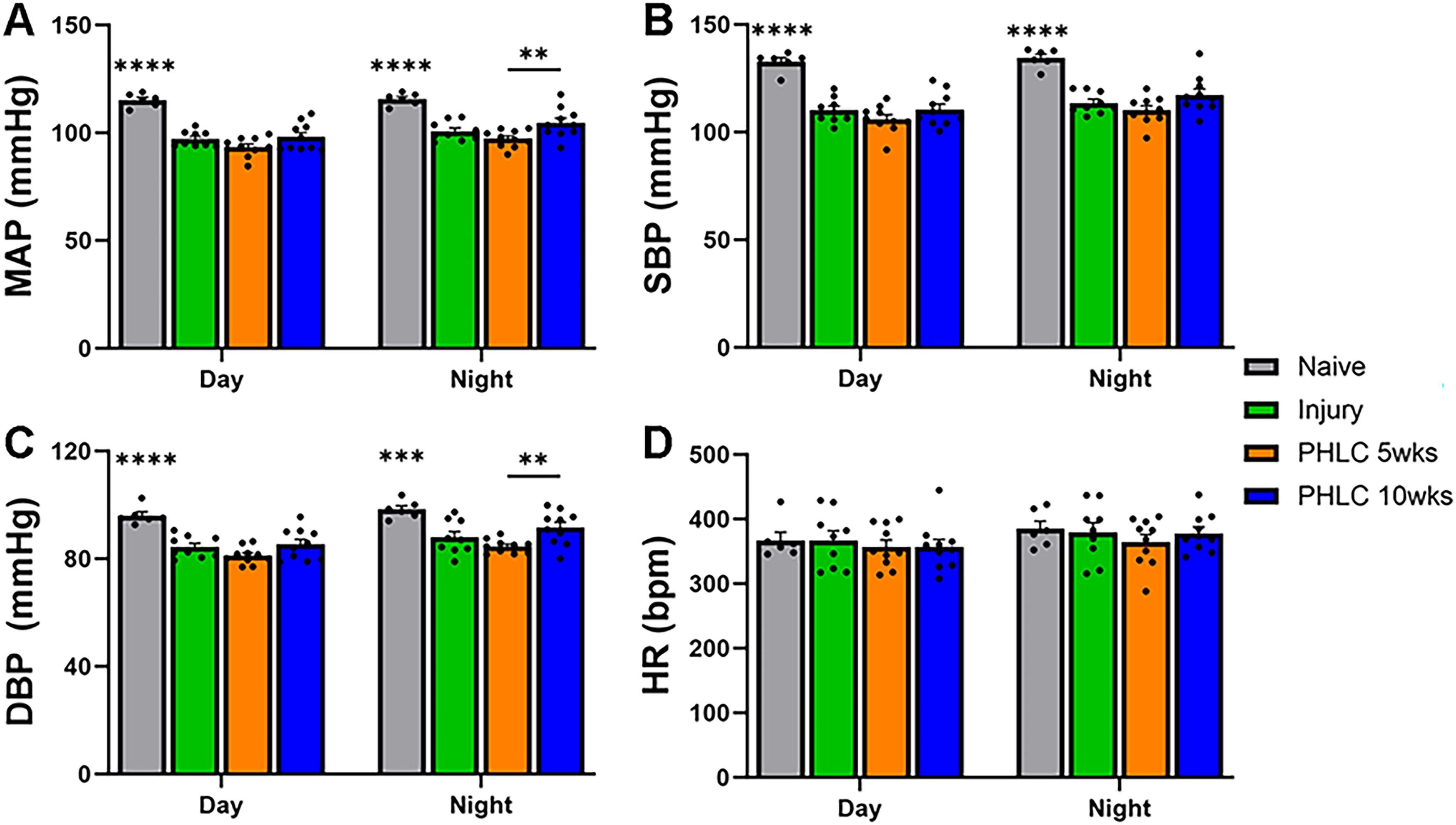
Resting hypotension following SCI remains post to passive exercise intervention.
Spontaneous autonomic dysreflexia
The occurrence of spontaneous autonomic dysreflexia events was assessed by analyzing hemodynamic parameters from the 24-h recording. Following SCI, episodes of spontaneous autonomic dysreflexia were frequently detected, which were characterized as a short period of blood pressure elevation accompanied by bradycardia (Fig. 2A and B). The data distribution was variable (from 3 to 13 bouts) in individual subjects, which might be associated with variable bodily conditions post to injury. Notably, passive cycling caused a significant reduction in the number of spontaneous autonomic dysreflexia events in rats receiving the training either for 5 weeks (6.6 ± 1.2 vs. 2.3 ± 1.6, p < 0.01, non-parametric Kruskal–Wallis test followed by Dunn’s post hoc) or for 10 weeks (3.1 ± 0.9, p < 0.05) (Fig. 2C). No significant difference was seen between training with 5 and 10 weeks.
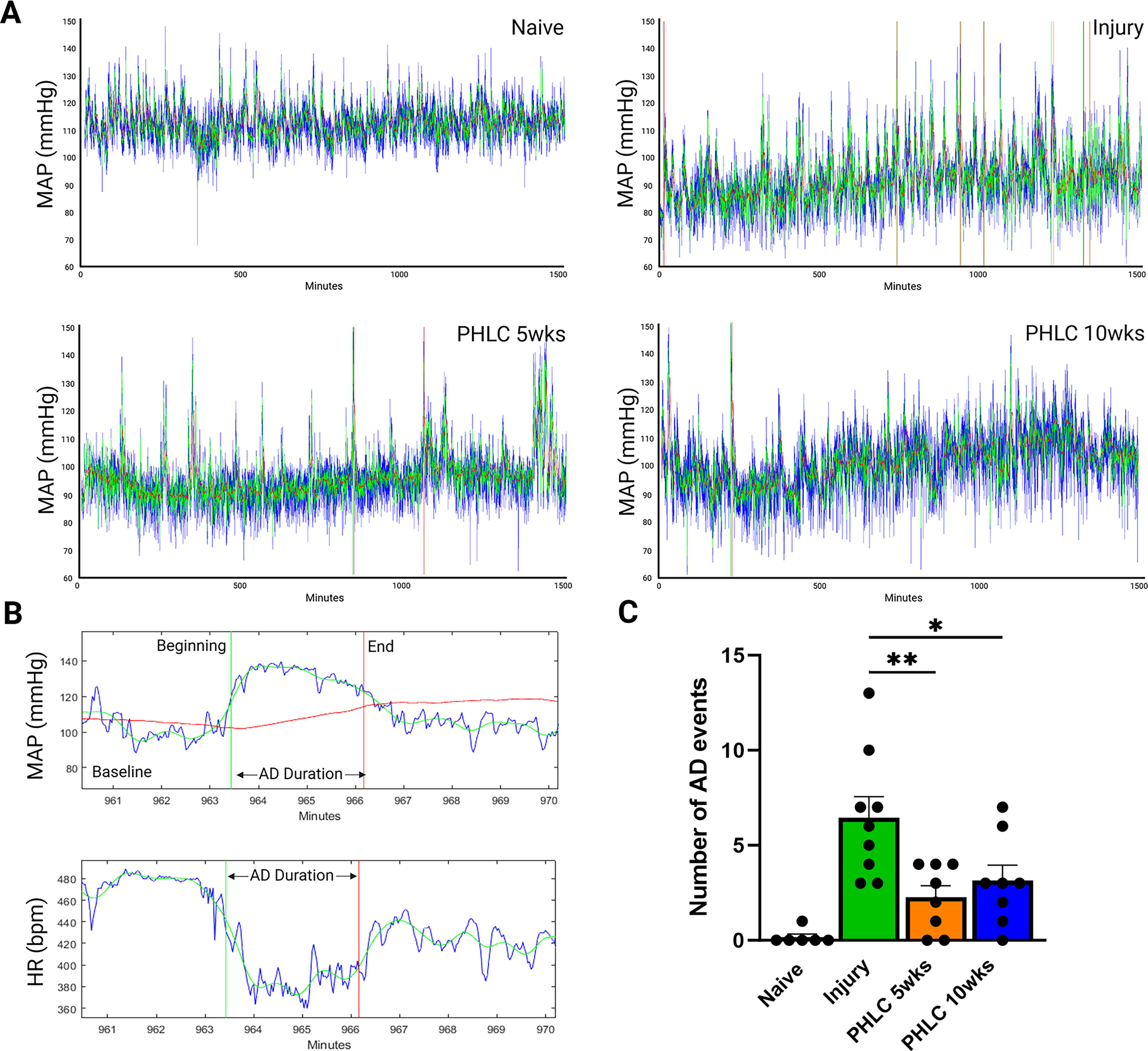
PHLC reduces the occurrence of spontaneous autonomic dysreflexia events.
CRD-induced autonomic dysreflexia and arrhythmias
Noxious CRD induced a dysreflexic response in all groups of SCI rats. Various cardiac arrhythmias were detected in ECG recordings (Fig. 3A and B). Statistical analysis showed no significant (both p > 0.05, one-way ANOVA following by Tukey’s post hoc) difference in blood pressure and HR changes between groups with and without exercise (Fig. 3C). Compared with the injury control, the number of severe arrhythmias, including AV block, PVC single, and sinus pause, was significantly decreased in animals with PHLC for 10 weeks (p < 0.05, non-parametric Kruskal–Wallis test followed by Dunn’s post hoc) and has a trend of decrease in animals with PHLC for 5 weeks (p = 0.082) during CRD-induced autonomic dysreflexia (Fig. 3D).

PHLC decreases the occurrence of cardiac arrhythmias during CRD-induced autonomic dysreflexia.
Dobutamine test for arrhythmias
To assess if exercise is beneficial for the tolerance of cardiac electrical conduction in response to environmental changes following SCI, DOB was administered in serial doses to stimulate sympathetic pathways to the heart. The drug at different doses induced a large number of arrhythmias in rats with SCI only. However, a reduction in the number of cardiac arrhythmias was identified in rats treated with PHLC (Fig. 4A). We counted the number of AV block, PVC single, and sinus pause arrhythmias. Delivery of a low dose of DOB (5.0 µg/[kg·min]), compared with rats with injury only, triggered fewer severe arrhythmias in rats trained with PHLC for either 5 or 10 weeks (both p < 0.01, non-parametric Kruskal–Wallis test followed by Dunn’s post hoc). Similarly, a mid or high dose of DOB (12.5 or 20 µg/[kg·min]) caused significantly reduced occurrence of arrhythmias in animals with PHLC for 10 weeks (p < 0.05) than that in injury controls (Fig. 4B). Furthermore, there was no significant difference in this cardiac parameter between both PHLC groups and naive controls in all doses. It indicates that passive exercise can enhance the adaptation of cardiac electrical conduction to stimulations.

PHLC reduces the occurrence of cardiac arrhythmias during DOB test.
Pharmacological interventions to assess autonomic tone
To examine exercise-induced potential alterations in autonomic tone, pharmacological agents were delivered, and changes in HR were measured. When atropine was administered to block parasympathetic tone, there was no statistical difference (p > 0.05, one-way ANOVA) in the change of HR reflecting sympathetic tone between groups, although the value was nonsignificantly reduced in rats with SCI alone but elevated in rats with PHLC for 5 weeks (Fig. 5A). When metoprolol was delivered to block cardiac sympathetic activity, sympathetic tone slightly reduced while there was a significant increase (p < 0.01, one-way ANOVA followed by Tukey’s post hoc) in parasympathetic tone in animals receiving SCI alone compared with naive animals (Fig. 5B). Notably, a trend of reduction in parasympathetic tone was observed in rats trained with PHLC for 5 (p = 0.097) or 10 weeks (p = 0.062). This suggests that exercise can improve the balance of autonomic activity following SCI.
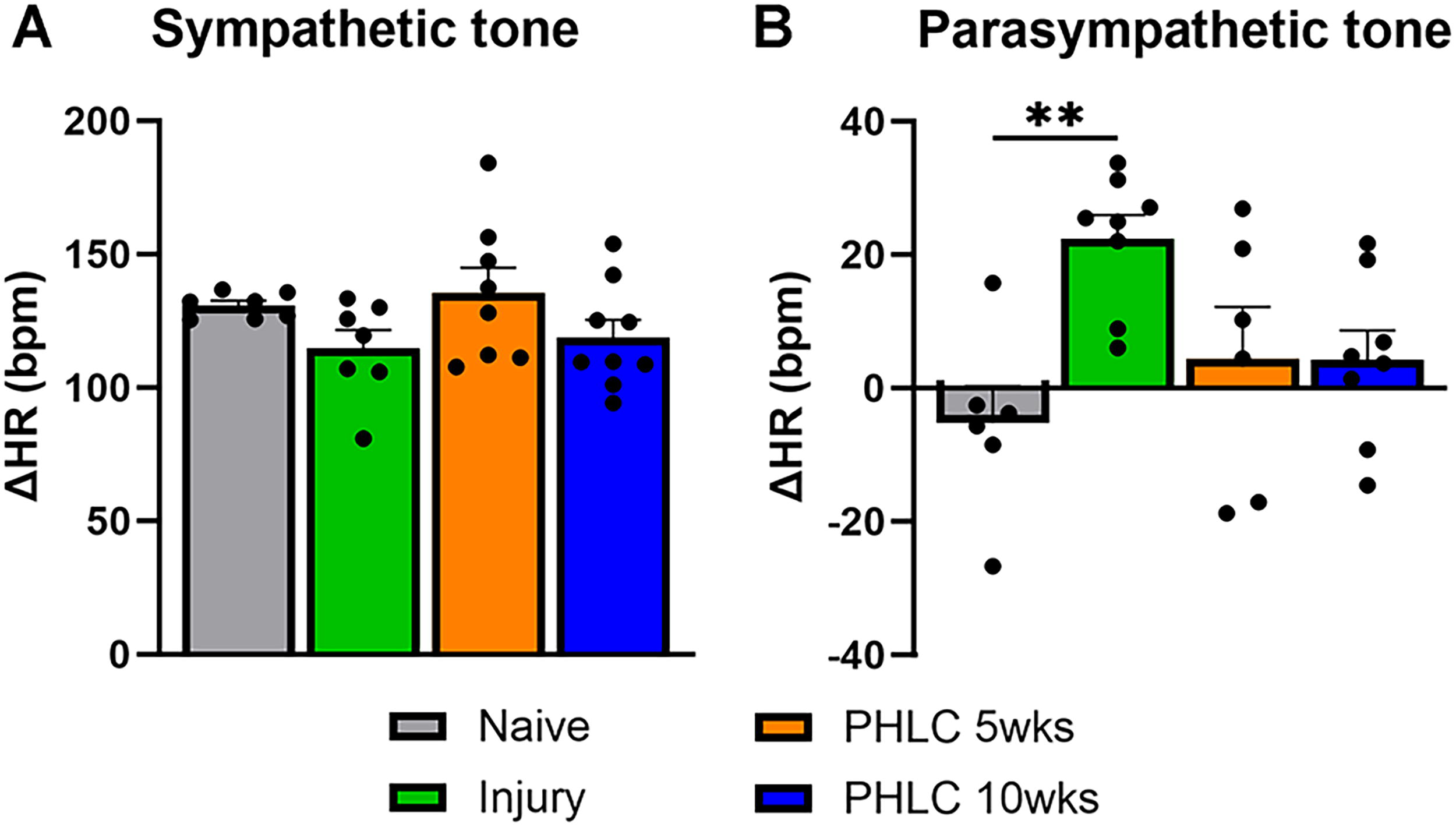
PHLC reduces unopposed cardiac parasympathetic tone. Pharmacological analysis reveals that following SCI,
Discussion
In the present study, we evaluated the effects of passive exercise on the development of cardiac conduction disorders following SCI. PHLC reduced the frequency of spontaneous autonomic dysreflexia while it did not change resting blood pressure and HR. The incidence of cardiac arrhythmias in animals with exercise training was decreased during either CRD-induced autonomic dysreflexia or DOB-mediated sympathetic stimulation to the heart. This effect could be attributed to the fact that PHLC reduces aberrantly increased cardiac parasympathetic tone in rats with SCI, which in turn improves the balance of autonomic regulation. In general, it appeared long-term PHLC had a better effect on the tolerance of cardiac electrical conduction than the short term.
As a noninvasive therapeutic intervention for SCI, exercise increases neural plasticity in the spinal cord and maintains body muscle mass by elevating levels of neurotrophic factors in the muscle and spinal cord tissue. At the molecular level, the mTOR is a key factor in an intracellular signaling pathway that regulates protein synthesis, cell growth, and proliferation. 32 Exercise affects the expression of PTEN, an upstream inhibitory mediator of mTOR, and in turn plays a role in many vital cellular processes, such as cell proliferation, motility and survival, and activity-dependent plasticity. 19 This eventually contributes to the improvement of sensorimotor functional recovery after SCI. The effect of exercise on the autonomic nervous system that regulates cardiovascular function is mediated via the muscle metaboreflex and mechanoreflex mechanisms, which primarily include central commands, exercise pressor reflex, and baroreflex. 33 In this process, several types of metaboreceptors are responsible for sensing metabolites elicited by muscle contractions. 34 In parallel, thin-fiber muscle afferent neurons sense mechanical distortion and deformation. The signal is conveyed as action potentials to the second neurons in the spinal cord, which in turn project to the nucleus tractus solitarius (NTS). Neurons within the NTS integrate the ascending sensory information and output the efferent signal to the sympathetic center, the rostral ventrolateral medulla, as well as parasympathetic nuclei, the dorsal motor nucleus of the vagus, and the nucleus ambiguous.35,36 As a result, this increases blood pressure and HR by activating the sympathetic system and inhibiting parasympathetic activity. Following SCI at a high-level, sympathetic activity often reduces, and parasympathetic activity increases. 37 When an SCI rat performs hindlimb cycling, the physical activity is not limited to the hindlimb muscle but the whole body, according to our observation. It means the activity stimulation can spread to the muscles above the lesion level, which mediates the effect through the mechano/metaboreflex mechanisms even though the spinal cord is interrupted. On the other hand, exercise maintains muscle mass and prevents vascular atrophy, beneficial to preserving peripheral structures.13,23 In addition, previous studies showed that PHLC affects spinal interneurons for plasticity, 17 which may also contribute to improving intraspinal sympathetic regulation. In the results, MAP and DBP during nocturnal rhythm were higher in animals receiving 10 weeks than those with 5 weeks of PHLC. However, both improvements did not differ from the injury control or reach the level in naive rats. This subtle improvement could be caused by elevated resting vascular sympathetic tone after exercise. Here, PHLC shows to decrease the unopposed cardiac parasympathetic tone, regardless of 5 or 10 weeks duration. This evidence supports the concept of exercise suppressing parasympathetic activity, leading to enhanced autonomic balance.
Both branches of the autonomic nervous system are activated during autonomic dysreflexia events in subjects with SCI. It is thought to have the most detrimental outcomes on patient health. Peripheral or visceral stimulation below the level of injury evokes high sympathetic discharge that manifests in episodic hypertension and subsequent baroreflex-mediated bradycardia. 38 This co-activation of these systems is known as “autonomic conflict,” which is thought to be proarrhythmogenic. 39 Specifically, the recurrence of autonomic dysreflexia episodes increases spatial dispersion of ventricular repolarization, perpetuating the incidence of cardiac arrhythmias. 40 The expression of cardiac calcium regulatory proteins that modulate electrical conduction of cardiac tissue changes following SCI, such as increased relative protein expression of sarco(endo)plasmic reticulum Ca2+ ATPase (SERCA2) and Na/Ca exchanger but decreased phospholamban. 41 These changes in regulatory proteins are associated with elevated electrophysiology parameters and reduced threshold to induce ventricular arrhythmias. 42 On the other hand, structural remodeling of cardiac tissue has been shown to occur after SCI. The prominence includes collagen deposition in the interstitial space and myocardial fibrosis, particularly in the left ventricle. 23 Increased collagen deposition plays a major role in abnormal electrical impulse initiation to facilitate cardiac arrhythmia generation. 43 Accordingly, the increased susceptibility for cardiac conduction disorders is a cumulative effect of a variety of functional, molecular, and structural changes to the cardiovascular system after SCI.
Though previous studies have demonstrated the occurrence of cardiac arrhythmias during autonomic dysreflexia, 44 there was a lack of a detailed analysis of types. Here, we demonstrated that CRD successfully induced arrhythmias in SCI rats during autonomic dysreflexia. Various arrhythmias were detected, e.g., AV block, PVC single, and sinus pause. These types of cardiac arrhythmias are particularly worrisome because they are severe, and if left untreated, they can progress into asystole, ventricular tachycardia, and induce cardiomyopathy. 45 PHLC maintained for 10 weeks can alleviate the occurrence of these life-threatening cardiac arrhythmias during CRD-induced autonomic dysreflexia, though the severity of dysreflexia was not improved. In addition, we found a significant reduction in the number of spontaneously occurring autonomic dysreflexia events over the course of the 24-h recording in animals receiving exercise compared with injury control animals. This suggests that an improved balance of sympathetic and parasympathetic activity attenuates the occurrence of autonomic dysreflexia. It is possible that, through improving the synchrony of the autonomic nervous system, long-term exercise can attenuate the development of cardiac conduction disorders after SCI. Both 5- and 10-week PHLC reduces the number of spontaneous autonomic dysreflexia events but not the severity of CRD-induced ones. Spontaneous autonomic dysreflexia is a naturally occurring event, and its improvement may be easily detected after exercise enhances multiple system activities, such as autonomic regulation and bladder reflex. In contrast, CRD is a noxious, severe, and strong artificial stimulation of pelvic visceral sensory nerves, potential improvements in hemodynamics could be masked under extreme responses accordingly.
DOB is a β1-adrenergic receptor agonist that is utilized to stimulate sympathetic activity and increase the rate of myocardial contractility, mimicking cardiac stress. In the clinical setting, DOB infusion is a standard procedure to assess cardiac load and identify heart disease. The use of DOB for such purposes has also been established in various rodent models of cardiac disease. More recently, the DOB stress test has been performed following high-level SCI to examine the role of sympathetic activation on the susceptibility of cardiac arrhythmias, in which DOB infusion significantly increases the occurrence of a variety of cardiac arrhythmias 12 and ECG markers associated with the risk for ventricular arrhythmias. 30 In the present study, all three doses of DOB triggered considerable events of arrhythmias after high thoracic SCI. A significant decrease or trend in arrhythmia generation was detected in animals receiving exercise for 5 or 10 weeks at the low and mid doses, indicating improved cardiac tolerance by PHLC training. The dampened sympathetic regulation to the heart following SCI can change the sensitivity and regulation of β1-adrenergic receptors on cardiac tissue, contributing to arrhythmia generation. 46 Since exercise has been shown to have beneficial effects on β1-adrenergic receptor signaling and responsiveness, 47 this is one of the possible mechanisms in addition to improved balance of autonomic activity by passive training.
For SCI subjects with lower limb paralysis, active upper-limb, and passive lower-limb exercise are two exercise interventions. DeVeau et al. previously compared them with examine how either exercise influenced cardiac contractile and volumetric responses in rats. 24 It was demonstrated that lower-limb exercise positively influenced flow-derived cardiac indexes, whereas upper-limb exercise did not. Moreover, neither intervention improves the cardiac contractile dysfunction associated with SCI. Thus, the advantage of utilizing PHLC over active exercise is not only its physical and economical feasibility for patients with limited lower extremity function but also its effect on cardiovascular performance. With sex as a biological variable, female rodents were predominately used in preclinical SCI studies due to the ease of bladder care. The influence of sex difference on outcomes following SCI remains controversial based on existing clinical and preclinical data. 48 In cardiovascular function, there is currently no definitive conclusion on whether sex influences exercise’s effect.
High-level SCI often causes cardiac atrophy, such as increased collagen deposition, myocardial fibrosis, and neural innervation alterations. 11 It is possible that PHLC may reverse or prevent these aberrant structural changes, which could be the morphological basis related to the improvement in cardiac electrical conduction in the present study. Due to technical limitations, we did not conduct gross cardiomyocyte histology to verify. However, a recent clinical report described there is a linear loss of left ventricular cardiac structure following SCI that is not attenuated by rehabilitative exercise practices. 49 This uncertainty needs further studies to be addressed.
Conclusion
PHLC significantly reduces the occurrence of cardiac arrhythmias during CRD-induced autonomic dysreflexia and DOB administration in rats with SCI. The effect is more noticeable in long-term rather than short-term exercise. This improvement is likely attributed in part to enhanced harmony of autonomic regulation of the heart in that aberrant parasympathetic predominance is decreased with PHLC training. Ultimately, the results provide insights into the use of exercise intervention to mitigate abnormalities in cardiac electrical conduction in subjects with SCI. In the next step, we will determine how to tailor the regimen, e.g., duration and intensity, for cardiac functional recovery.
Transparency, Rigor, and Reproducibility Summary
The study design and analytical plan were not formally pre-registered. The sample size was 7–10 based on previous studies. A total of 38 rats were randomly assigned to groups. Two rats were excluded due to high BBB scores, indicating incomplete injury. Although blinding fashion was difficult to be used for animal surgery and device implantation, data analysis was blindly conducted. Radio-transmitter Implantation was conducted one week before recordings so that the surgical effect faded when measuring physiological parameters. All drug doses were based on previously published literature. All reagents and drugs were commercially available. The spinal cord crush injury model, physiological recordings, and data analysis protocol were established standards in the field. Outliers in the dataset had been detected and excluded using the Inter-Quartile Range proximity rule. Appropriate one-way or two-way ANOVA followed by Tukey’s post hoc was used to analyze blood pressure and HR data. The number of arrhythmias that was usually not distributed normally was statistically analyzed using the non-parametric Kruskal–Wallis test followed by Dunn’s post hoc. Data from this study are not available in a public archive. The full content of the article, experimental data, and protocols will be available upon reasonable request.
Authors’ Contributions
S.H., V.J.T., and J.D.H. designed the experiments. M.C. and S.H. carried out the experiments, analyzed data, and prepared figures. M.C., V.J.T., J.D.H., and S.H. wrote the article. J.D.H. oversaw the project.
Footnotes
Acknowledgments
The authors are grateful for Trevor Smith’s technical help and thank Silvia Fernandes, Emily Taub, and Krupa Patel for providing animal care assistance.
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
This work was supported by NIH/NINDS R01 NS121336, Pennsylvania Commonwealth Universal Research Enhancement (SAP 4100083087), and the Missouri Spinal Cord Injury/Disease Research Program (SCIDRP) 2024 fund to S.H., and R01NS106908 and R01NS122371 to V.J.T.