
Abstract
Traumatic brain injury (TBI) is a major global health concern, contributing substantially to mortality and disability. While previous studies have reported the global and regional burden of TBI, few have explored its long-term trends, cause-specific burden, sociodemographic disparities, and future projections in a comprehensive framework. To address this gap, we conducted a retrospective analysis using the Global Burden of Disease 2021 data to estimate TBI incidence, prevalence, and years lived with disability across sex, age, and Sociodemographic Index (SDI) quintiles. We used average annual percent change (AAPC) to evaluate temporal trends from 1990 to 2021 and applied Spearman’s correlation to examine the association between age-standardized incidence rate (ASIR) and SDI. Projections of future trends were made using an autoregressive integrated moving average model. The results revealed that global TBI cases increased from 17.0 million in 1990 to 20.8 million in 2021, although the global ASIR decreased from 324.43 to 259.02 per 100,000, with an AAPC of −0.80%. The age-standardized prevalence rate (ASPR) also declined in high SDI locations, from 539.7 to 425.9 per 100,000 (AAPC: −0.76%), with similar declines observed in high-middle SDI locations. Southern Sub-Saharan Africa showed the largest reductions, whereas Oceania experienced a slight increase in ASIR, largely driven by falls and road injuries, with notable gender-specific patterns. By 2031, TBI incidence rates are projected to decline for both sexes, with falls remaining stable and road injuries decreasing. While the ASIR and ASPR of TBI have decreased, the absolute number of cases has risen, underscoring the need for public health interventions that consider regional differences in TBI trends and causes in order to effectively reduce the burden.
Introduction
Traumatic brain injury (TBI) is a major cause of injury-related deaths and disabilities worldwide, exerting profound impacts on global health care systems. 1 Global economic analyses reveal that TBI imposes substantial economic burdens globally, including direct costs such as acute medical care and rehabilitation, and indirect costs related to productivity losses and long-term community support, both of which have continued to rise. Recent estimates indicate that 50–60 million individuals sustain TBI annually, generating an estimated annual economic impact exceeding USD 400 billion worldwide. Among all common neurological disorders, TBI has the highest incidence and constitutes a major public health burden. In Europe, more than 2 million people are admitted to hospitals each year because of TBI, and about 82,000 die. 1,2 TBI presents a multifaceted challenge, marked by its diverse etiologies, complex mechanisms of injury, and the varying clinical outcomes. 3 Its burden varies significantly across regions and countries, with disparities in incidence and mortality rates often linked to differences in socioeconomic status, health care infrastructure, access to services, and public health policies. 4,5 These disparities underscore the necessity for a targeted and effective approach to tailored public health interventions across countries and regions.
Despite growing research on TBI, significant gaps remain. Although an increasing number of studies have begun to focus on the causes of TBI and its clinical outcomes, less attention has been given to the long-term burden and the cumulative effects of repeated injuries by regions and countries. 6 Furthermore, individuals in low-income and middle-income countries are particularly affected by TBI, and disparities in infrastructure development, pre-hospital emergency care, and post-acute care further exacerbate the burden of TBI in these regions. 7 This lack of detailed, regional or national, cause-specific data impedes the development of effective global strategies to prevent and manage TBI.
Recently, two Global Burden of Disease (GBD)-based studies outlined the TBI burden globally or regionally 8,9 and have generally focused on descriptive analyses. However, existing studies lack detailed investigation into cause-specific trends, sociodemographic disparities, and forward-looking projections—particularly for low- and middle-income countries. To address these gaps, we conducted an in-depth analysis of TBI burden from 1990 to 2021 using data from the GBD 2021 study. Our analysis was disaggregated by sex, age, Sociodemographic Index (SDI), region, and country, providing a multidimensional understanding of TBI trends. We applied a suite of advanced statistical approaches to achieve four main objectives: (1) to assess temporal trends in incidence, prevalence, and disability using average annual percent change (AAPC); (2) to examine the association between age-standardized incidence rate (ASIR) and SDI using Spearman’s correlation; and (3) to analyze burden patterns by cause and gender; and (4) to project future trends in TBI incidence through 2031 using an autoregressive integrated moving average (ARIMA) model. Collectively, these efforts provide a more comprehensive and policy-relevant evidence base to support the development of targeted strategies aimed at reducing the evolving global burden of TBI.
Methods
Research overview
This study utilized data from the GBD 2021, which provides comprehensive epidemiological estimates for 371 diseases and injuries across 21 GBD regions and 204 countries or territories from 1990 to 2021. Repeated cross-sectional data were obtained from the Global Health Data Exchange (GHDx) results tool, including annual patient cases and rates (per 100,000) of incidence, prevalence, mortality, and years lived with disability (YLDs) by sex, age, region, SDI, and country.
Data collection and processing
The GBD 2021 study model incorporates improved methodologies to enhance the accuracy of global health loss estimations. This includes the use of spatiotemporal Gaussian process regression for smoother data representation across locations and time, 10 as well as the use of DisMod-MR to ensure consistency and comparability across diverse data sources. 11 GBD 2021 rigorously quantified uncertainties, generating 95% uncertainty intervals (UI) for each metric, derived from the 25th and 975th values of 1000 simulations in the model’s posterior distribution.
Definition and classification of TBI
TBI is defined according to internationally recognized standards, utilizing clinical symptoms and Glasgow Coma Scale to classify injury severity. Although TBIs can result in death, they are not considered direct causes of death within the GBD 2021 framework; instead, injury causes leading to TBI (e.g., falls and road injuries) are recorded as causes of death. 12 Therefore, GBD 2021 focuses on estimating the non-fatal burden by reporting incidence, prevalence, and YLDs. 13 We investigated all level 3 causes associated with TBI as defined in the GBD framework, covering 16 different causes.
Analytical strategy
Our analysis began with descriptive statistical assessments of age-standardized rates (ASR) of TBI incidence, prevalence, and YLDs from 1990 to 2021, segmented by gender, subtypes, age, SDI quintiles, GBD regions, and countries/territories, along with corresponding AAPC. We subsequently concentrated on the etiological causes of TBI, estimating independent ASRs and AAPCs for all level 3 causes to gauge their impact and trends. Further analysis investigated the correlations between TBI metrics and SDI levels across different causes. Finally, ARIMA models were employed to forecast the incidence rates for all causes and the top three causes of TBI over the next decade, aiming to understand future changes in TBI burden. The utilization of de-identified public data did not necessitate additional ethical approval and was in compliance with GATHER reporting guidelines. 14
Software and statistical significance
Analysis was conducted using R software for data analysis, and Joinpoint software for calculating AAPC. Spearman’s rank correlation coefficient was used to assess the correlation between national ASIR and their corresponding SDI. A two-sided p < 0.05 was considered statistically significant.
Results
Incidence and prevalence
Globally, the number of TBI cases in 2021 reached 20,837,466, a notable increase from 17,001,269 in 1990 (Table 1). From an incidence rate perspective, the global ASIR of TBI showed an overall decline, decreasing from 324.43 per 100,000 (95% UI, 283.29 to 370.12) in 1990 to 259.02 per 100,000 (95% UI, 225.5 to 296.2) in 2021, corresponding to an AAPC of −0.80% (95% CI, −0.86 to −0.74). The ASIR in both genders exhibited similar decreases (Supplementary Figure A2), with male AAPC of −0.80% (95% CI, −0.85 to −0.75) and female AAPC of −0.77% (95% CI, −0.86 to −0.68). Marked differences in the incidence of TBI were observed across age groups (Supplementary Figure A3), with a consistent increase in TBI incidence observed among individuals aged 65 and older across both genders. This decreasing trend was also evident in age-standardized prevalence rates (ASPR), which declined across TBI subtypes, SDI quintiles, and several regions. For example, in high SDI quintiles, prevalence rates decreased from 539.65 per 100,000 (95% UI, 517.84 to 563.45) in 1990 to 425.88 per 100,000 (95% UI, 407.03 to 445.42) in 2021, with an AAPC of −0.76% (95% CI, −0.77 to −0.75). Similarly, ASPR in high-middle SDI quintiles dropped from 702.29 per 100,000 (95% UI, 676.46 to 733.40) to 543.29 per 100,000 (95% UI, 520.89 to 567.07), with a corresponding decline in ASIR, suggesting an overall reduction in the number of new cases and the total burden over time.
Trends in TBI Incidence Across Global, Gender, Subtype, and SDI Quintiles from 1990 to 2021
ASIR, age-standardized incidence rate (per 100,000); AAPC, annual average percentage change; TBI, traumatic brain injury; SDI, Sociodemographic Index.
Regionally, Southern Sub-Saharan Africa exhibited a significant reduction in both ASIR and ASPR. The ASIR fell from 357.97 per 100,000 (95% UI, 309.2 to 409.65) in 1990 to 248.70 per 100,000 (95% UI, 217.66 to 279.55) in 2021 (Supplementary Table A1), while ASPR showed a similar decline (Supplementary Table A2), with an AAPC of −1.54% (95% CI, −1.56 to −1.52). In contrast, Oceania presented a unique case where both ASIR and ASPR increased over the study period, indicating an ongoing or growing public health challenge in this region. ASIR in Oceania increased from 198.15 per 100,000 (95% UI, 176.46 to 220.84) to 228.96 per 100,000 (95% UI, 203.66 to 258.52), with an AAPC of 0.32% (95% CI, 0.08 to 0.55).
At the national level, China’s ASIR and ASPR remained relatively stable, with a slight increase in both metrics. The ASIR increased (Fig. 1A) from 258.53 per 100,000 (95% UI, 224.46 to 295.09) to 265.59 per 100,000 (95% UI, 226.84 to 308.75), while ASPR followed a similar trend (Fig. 1B), reflecting the country’s consistent burden over time. Conversely, the Federal Democratic Republic of Ethiopia demonstrated a significant decline in both ASIR and ASPR, highlighting effective public health interventions or other contributing factors. A few countries showed a significant increase in incidence and prevalence rates, such as the Islamic Republic of Afghanistan and the Republic of Yemen (Supplementary Table A1).

Temporal trends in AAPC of TBI from 1990 to 2021 across 204 countries and territories. Panel
Trends in YLDs
The trends in age-standardized YLDs rate (ASYR) closely followed the patterns observed in ASPR, mostly showing a downward trend (Supplementary Table A3). In high SDI quintiles, ASYR decreased in line with the reductions in ASPR, from 73.37 per 100,000 (95% UI, 51.66 to 98.57) in 1990 to 58.24 per 100,000 (95% UI, 40.87 to 78.36) in 2021, with an AAPC of −0.74% (95% CI, −0.75 to −0.73). In low-middle SDI quintiles, ASYR did not show any significant changes.
Southern Sub-Saharan Africa, with its significant decrease in ASIR and ASPR, also saw a corresponding reduction in ASYR, reinforcing the positive impact of decreasing new cases on overall disability burden. Oceania showed a slight increase in ASYR, with an AAPC of 0.56% (95% CI, 0.50 to 0.63), consistent with its trends both in ASIR and ASPR. Nationally, China’s stable ASYR mirror its consistent ASIR and ASPR trends (Fig. 1C), while the Republic of South Africa’s reduction in ASYR aligns with its overall decrease in TBI burden (AAPC: −1.82%; 95% CI, −1.84 to −1.81).
Leading causes of TBI incidence
In 2021, the global incidence of TBI was primarily driven by falls and road injuries, with distinct patterns observed between males and females (Fig. 2). Falls were the leading cause globally, with an incidence rate of 146.63 per 100,000 in males and 87.30 per 100,000 in females. Road injuries were the second leading cause, with incidence rates of 92.61 per 100,000 in males and 35.31 per 100,000 in females. Over the period from 1990 to 2021, the incidence of TBI from falls showed distinct gender differences, with a male AAPC of −0.06% (95% CI, −0.09 to −0.03) and a female AAPC of 0.18% (95% CI, 0.16 to 0.19). The incidence from road injuries decreased modestly, with a male AAPC of −0.99% (95% CI, −1.00 to −0.98), while females saw a more substantial decline, with an AAPC of −1.58% (95% CI, −1.60 to –1.57).
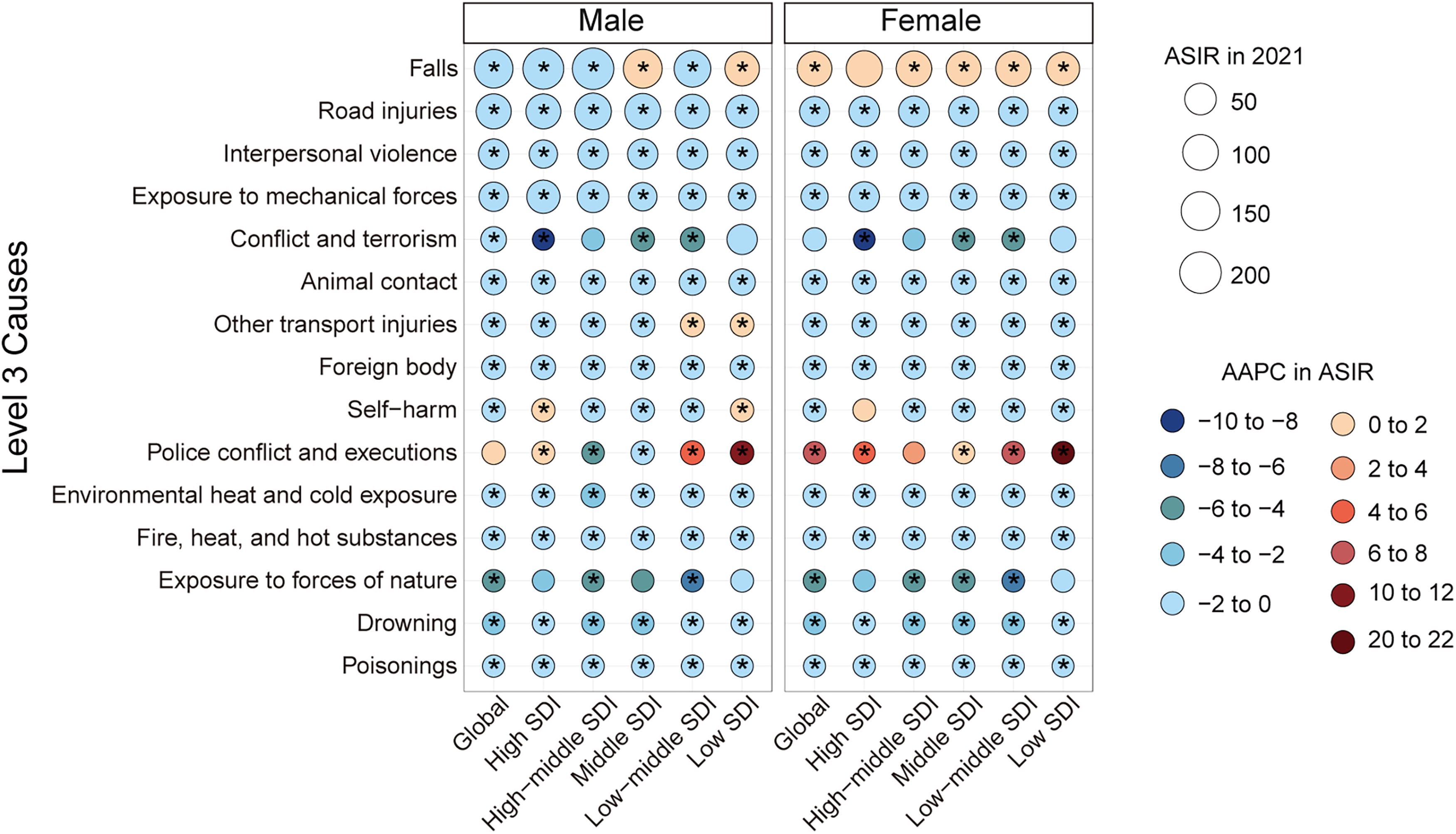
Global and SDI-stratified ASIR and AAPC by sex for level 3 causes of TBI in 2021. The size of each circle represents the ASIR of TBI for each gender within global and various SDI regions. Colors indicate different ranges of AAPC from 1990 to 2021. An asterisk (*) indicates a p value <0.05. ASIR, age-standardized incidence rate; AAPC, annual average percentage change; TBI, traumatic brain injury; SDI, Sociodemographic Index.
TBI incidence varied substantially across different SDI quintiles. Overall, the causes of TBI were similar across different SDI quintiles, but in middle SDI and low SDI quintiles, the male TBI incidence due to falls actually increased, while other SDI quintiles showed a decrease, and in all SDI quintiles, the incidence of falls in females showed a consistent increase. In addition, we observed a marked increase in the incidence of TBI due to police conflict and executions in low SDI quintiles, regardless of gender.
Similarly, the incidence of TBI exhibited considerable variability across different regions (Supplementary Figure A4). Although most regions had higher incidence rates of TBI due to falls, the trends from 1990 to 2021 showed considerable differences across regions. For example, Central Latin America had a male AAPC of −1.17% (95% CI, −1.22 to −1.13) showing a declining trend in males due to falls, while East Asia had a male AAPC of 1.23% (95% CI, 1.14 to 1.32) showing an increasing trend (Supplementary Table A4). In addition, some regions exhibited specific trends, such as Oceania, where the incidence of TBI related to interpersonal violence increased in both genders, and Eastern Sub-Saharan Africa, where the incidence related to police conflict and executions showed a marked increase.
TBI burden and relationship with SDI
Past studies found that in 2019, 204 countries or territories exhibited a low correlation between YLDs and SDI, 15 but considering that no distinctions were made for TBI subtypes and gender, we conducted a correlation analysis using data from 204 countries and territories in 2021. The results indicated that the overall male incidence rate (R = 0.51, p = 2.2e-15) and the overall female incidence rate (R = 0.55, p < 2.2e-16) both exhibited a correlation with SDI, and this correlation was further strengthened in minor TBI (Fig. 3A). However, prevalence (Fig. 3B) and YLDs (Fig. 3C) exhibited a weaker correlation, but this correlation was strengthened after subdividing TBI subtypes. For example, the overall female YLDs had a Spearman correlation coefficient of 0.44 (p = 2.1e-11) with SDI, while the female YLDs had a correlation of 0.65 (p < 2.2e-16) with SDI in minor TBI.
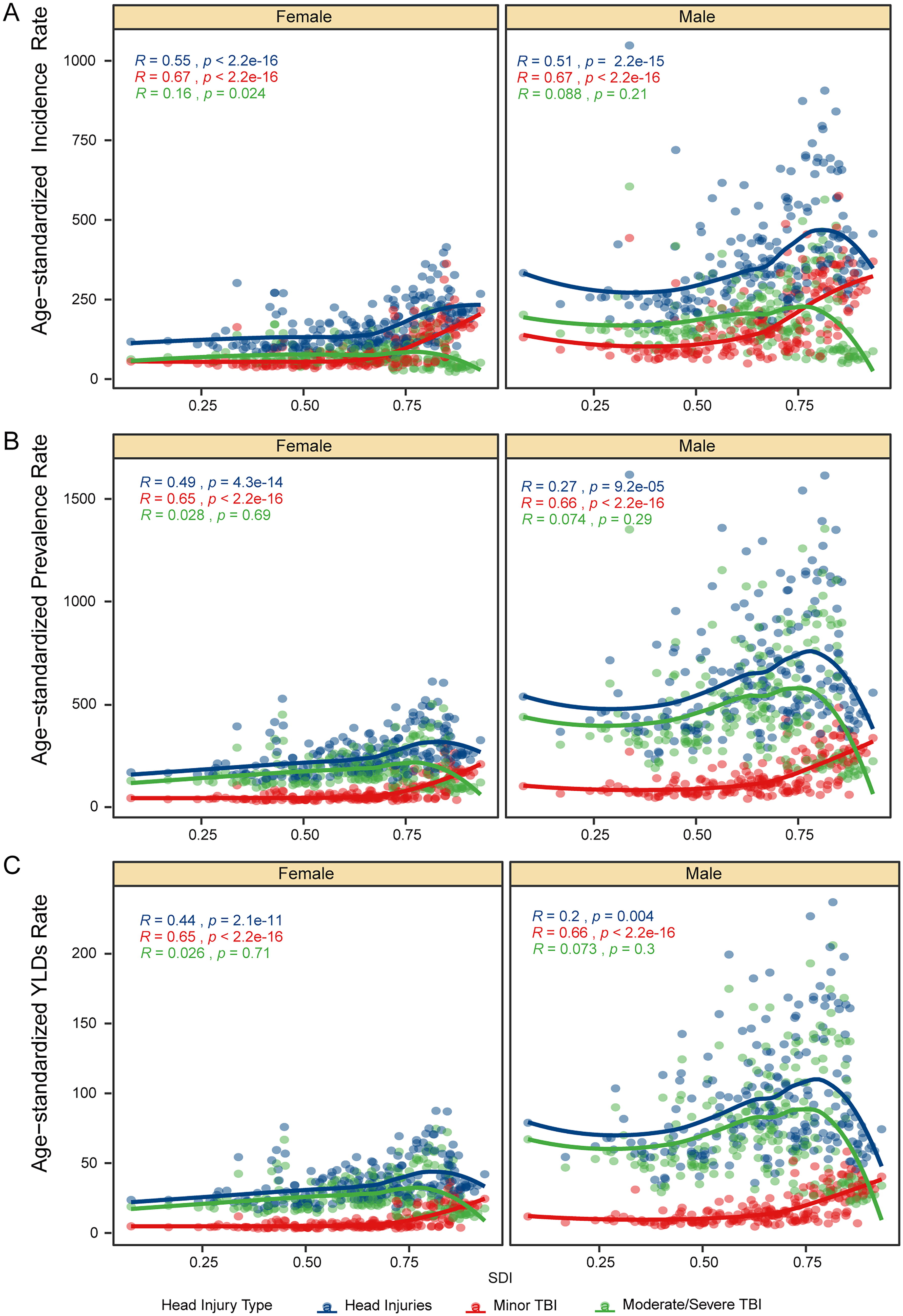
Spearman correlation between all-cause TBI burden and SDI in 204 countries and territories by gender in 2021. Panel
To further elucidate the specific relationship between causes of TBI and SDI, we conducted additional analyses. We found that falls, regardless of gender, exhibited the strongest correlation, and this correlation was further strengthened in minor TBI (Supplementary Figure A5). Particularly in males, the overall TBI, whether it was incidence, prevalence, or YLDs, had a correlation with SDI exceeding 0.7, and in minor TBI subtypes, the correlation exceeded 0.8. However, road injury did not exhibit a significant correlation in overall TBI (Supplementary Figure A6), but in minor TBI, both genders displayed a similar correlation in incidence, prevalence, and YLDs. In addition, other road injury-related TBI in males exhibited a higher correlation in incidence, prevalence, and YLDs with SDI than in females.
Ten-Year forecast of TBI burden
To estimate the TBI burden over the next 10 years, we employed an ARIMA model to project the incidence rate of TBI in males and females for the upcoming decade. It is projected that the overall male TBI incidence rate will decrease from 347.16 per 100,000 in 2021 to 315.30 per 100,000 in 2031, while the female rate will decrease from 169.87 per 100,000 to 153.75 per 100,000 (Fig. 4A). From a specific cause perspective, male TBI caused by falls is expected to remain stable, while female TBI will decrease from 87.30 per 100,000 to 82.43 per 100,000 (Fig. 4B). Unlike falls, the projected male road injury-related TBI incidence rate will decrease from 92.61 per 100,000 in 2021 to 80.84 per 100,000 in 2031 (Fig. 4C); similarly, the female rate is expected to decrease from 35.31 per 100,000 to 30.69 per 100,000 (Fig. 4D).
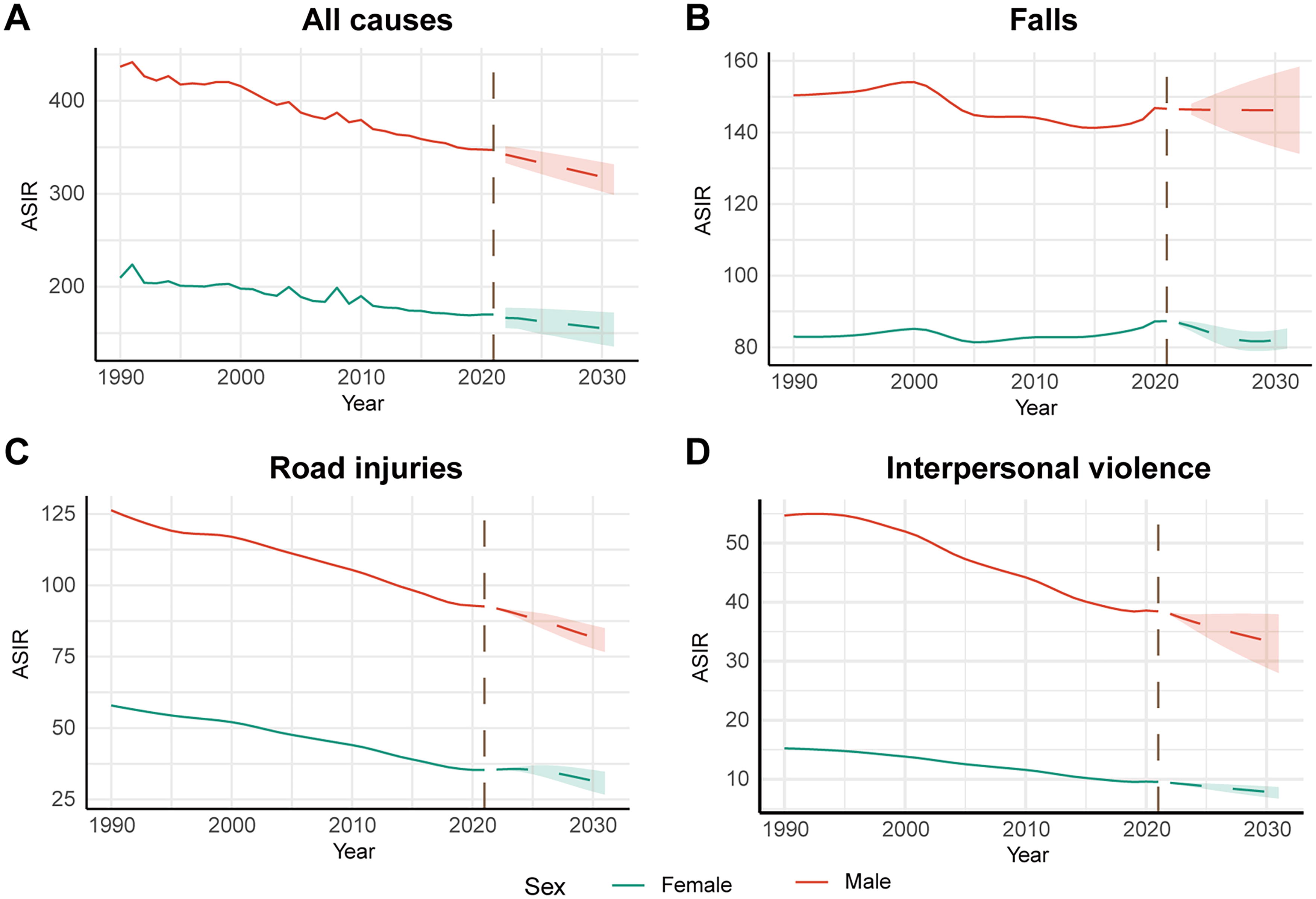
ARIMA forecast of TBI incidence changes over the next decade. Panel
Discussion
In this study, we employed the GBD framework to assess the burden of non-fatal TBI from 1990 to 2021. This analysis is the first to comprehensively evaluate these burdens across genders and ages on a global, regional, and national scale. Despite regional differences in TBI burden and causes, 1,16 –18 previous GBD-based studies have described the overall TBI burden and trends by country, they have not systematically examined how the burden of different causes of TBI—such as falls, road injuries, and interpersonal violence—has evolved over time. Our study fills this gap by analyzing long-term, cause-specific trends from 1990 to 2021, with additional stratification by sex and SDI. Moreover, by incorporating ARIMA-based projections, we extend the scope of prior research beyond retrospective description, providing forward-looking insights to support anticipatory public health planning. These contributions offer a more nuanced understanding of TBI epidemiology, especially in how distinct causes affect populations differently across time and development levels.
Between 1990 and 2021, the global ASIR of TBI declined, while the total number of cases increased, likely due to population growth and aging, particularly among individuals over 65. 19,20 However, in conflict-affected regions such as Yemen and Afghanistan, ASIR has continued to rise, highlighting the severe impact of ongoing instability on health care capacity, while countries like Iraq have seen improvements. These findings highlight the urgent need for targeted interventions in politically unstable regions to mitigate TBI risks. The regional disparities in TBI burden can be attributed to a combination of infrastructure, health care resources, and policy factors. In low- and middle-income countries, inadequate road safety infrastructure and weak traffic management contribute to higher rates of road injury-related TBI. In contrast, high-income countries have reduced TBI burden through advanced infrastructure and stringent traffic regulations. 21 In addition, the availability and quality of health care resources play a critical role; higher SDI countries benefit from better diagnostic capabilities and treatment facilities, leading to more effective management of TBI, particularly minor cases. 22 Policy interventions, such as Ethiopia’s targeted national health strategies, have demonstrated significant success in reducing TBI burden, whereas political instability in conflict-affected regions like Yemen and Afghanistan has exacerbated health care system failures, leading to increased TBI rates. 23 For example, in Central Sub-Saharan Africa, countries like South Sudan, the Central African Republic, and Libya have seen increased ASIR due to instability, while high-SDI countries in Central Europe, such as Lithuania, Hungary, and Estonia, have reduced TBI incidence through effective public health interventions. 24 China’s stable ASIR contrasts sharply with the significant decline observed in Ethiopia, where effective national health policies and interventions have played a critical role in reducing the TBI burden. Ethiopia’s success in implementing targeted strategies serves as a model for other nations seeking to achieve similar public health outcomes. 25,26
Falls and road injuries remain the leading causes of non-fatal TBI globally, with gender and age playing significant roles in the burden. 27 –29 In Eastern and Central Europe, both sexes have seen reduced fall-related burdens, while in Western Europe, men experienced a decline, but women saw an increase. To address the hazards caused by falls, the World Guidelines for Fall Prevention and Management for the Elderly, 30 introduced in 2019, mark a major milestone in global fall injury risk assessment and prevention, emphasizing the need for tailored strategies across different income regions. In response, researchers in Saudi Arabia have begun evaluating older women’s knowledge and perceptions of fall risks, assessing the feasibility of fall prevention interventions within the Saudi health care system. 31
Our analysis not only reveals correlations between TBI metrics and the SDI but also underscores their practical implications. Higher SDI is associated with better health infrastructure, leading to more effective TBI management, especially evident in minor TBI cases where enhanced diagnostic practices reflect higher health care quality. 32 –34 These insights suggest the need for interventions tailored to specific TBI causes and demographics; for example, robust SDI links with falls across genders advocate for socio-economically adapted prevention strategies, whereas weaker correlations with road injuries highlight the necessity of addressing cultural factors and enforcing traffic laws more rigorously. 18
Projections using an ARIMA model indicate a general decline in TBI incidence, driven by effective preventive measures. Emerging factors, such as population aging, urbanization, and changes in traffic policies, are likely to shape future TBI trends. Population aging, particularly in high-SDI countries, is expected to increase fall-related TBI among older adults. Rapid urbanization in low- and middle-income countries may exacerbate TBI burden due to overcrowded cities and insufficient road safety measures. However, advancements in traffic policies, including the adoption of autonomous vehicles and stricter enforcement of traffic laws, could significantly reduce road injury-related TBI. These emerging factors highlight the need for adaptive public health strategies that address the evolving landscape of TBI burden. However, the consistent rates of fall-related TBI in males, potentially due to demographic shifts like an aging population, call for refined strategies that accommodate specific gender and causal nuances. 35 The anticipated decrease in female fall-related TBIs suggests initial successes, contrasting with the urgent need for strengthened road safety measures, as evidenced by the slower reduction in road injury-related TBIs. 36
This study offers a comprehensive and in-depth analysis of the global burden of TBI over three decades, covering 204 countries and regions. It provides valuable insights into the nuanced drivers of TBI, and offers projections that equip policymakers with actionable insights for future planning, making the findings highly relevant for public health interventions and resource allocation. This study has several limitations. First, the reliance on GBD data may introduce biases and potential underreporting, particularly in low-income countries, due to disparities in health care access, the completeness of medical records, and reporting mechanisms. Second, although the GBD database integrates multiple data sources, its update frequency and timeliness may not adequately capture rapid changes in health conditions or interventions, potentially limiting the relevance of our findings for real-time policy and resource decisions. Lastly, inconsistencies in the classification and definition of TBI across jurisdictions may affect data comparability.
To address the limitations related to data quality and variability in TBI definitions, international collaboration and standardization efforts are essential. First, improving data quality can be achieved through enhanced global cooperation, such as establishing multinational data-sharing platforms that integrate hospital records, national surveys, and injury surveillance systems. These platforms should prioritize low- and middle-income countries, where underreporting and data gaps are most prevalent. In addition, capacity-building initiatives, including training health care professionals in data collection and reporting, can help improve the accuracy and completeness of TBI records. Second, standardizing TBI definitions globally is critical to minimizing variability in study outcomes. Organizations such as the World Health Organization and the Centers for Disease Control and Prevention could lead efforts to develop and promote a unified TBI classification system, incorporating clear diagnostic criteria and severity scales. This standardization would enable more accurate cross-country comparisons and facilitate the development of targeted interventions. By fostering international collaboration and adopting standardized definitions, the global health community can significantly enhance the reliability and comparability of TBI data, ultimately improving public health outcomes.
Conclusion
Our study provides a comprehensive, global assessment of TBI burden from 1990 to 2021, analyzing trends by age, sex, and SDI. We identified falls and road injuries as the leading causes of non-fatal TBI and projected future trends using ARIMA modeling, offering a foundation for targeted interventions. Distinct from previous studies that focused on regional snapshots or aggregate trends, our analysis dissects long-term patterns by injury cause, sex, and sociodemographic context, and uniquely adds predictive modeling to inform future public health planning. The use of ARIMA modeling for future projections provides actionable insights for long-term public health planning, setting this study apart from earlier research. These contributions advance TBI research and inform evidence-based strategies to reduce the global burden of TBI.
Transparency, Rigor, and Reproducibility
The study was based on secondary data from the GBD database, which is publicly accessible and therefore not pre-registered. The analysis plan was developed before data extraction, the data processing methods have been published in prior studies, 37 and the methodology for this study is comprehensively described in the Methods section. A total dataset covering the years 1990–2021 was analyzed, containing comprehensive data on TBI across various sociodemographic regions, ensuring >90% accuracy in estimating trends and projections for the primary outcomes with a p value <0.01. The dataset included all available records for head injury, with exclusions based on pre-defined quality criteria. The records were screened and provided comprehensive epidemiological estimates for 371 diseases and injuries across 21 GBD regions and 204 countries or territories from 1990 to 2021. Adequate data were obtained for gender, subtypes, age, SDI quintiles, GBD regions, and countries/territories after systematic quality assessment. No individual-level or patient-specific information was disclosed, as all analyses were conducted at an aggregate level. The analysis was conducted using R software (version 4.3.3) and followed the statistical and epidemiological standards established by the Institute for Health Metrics and Evaluation (IHME). All methods, including data cleaning, model assumptions, and sensitivity analyses, are described in detail in the supplementary materials. The primary data used in this study are available from the IHME GBD repository (https://ghdx.healthdata.org/gbd-results-tool). The analytic code used for this study is not publicly available but can be provided upon reasonable request by contacting the corresponding author. Scripts and methodological details will be shared to support replication and validation of the findings. This article will be published under a Creative Commons Open Access license (CC-BY 4.0) and will be freely available at [https://www.liebertpub.com/loi/neu] upon publication.
Footnotes
Acknowledgments
The authors sincerely thank the GBD team for allowing access to the comprehensive database.
Authors’ Contributions
L.G., L.Z., and C.L. designed and conceived the study, conducted the literature search, collated the data, acquired, analyzed, and interpreted the data, created the figures, and drafted the intellectual content of the paper. J.Z., L.J., C.J., Y.X., and J.Y. contributed to the study’s design and conception, analyzed the data, and revised the intellectual content of the paper. J.P. and Y.J. also contributed to the study’s design and conception, supervised the research, and revised the intellectual content of the paper. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved, read and approved the final article.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This work was supported by grants from the National Natural Science Foundation of China (82371310, 82271306, U24A20689), the Sichuan Science and Technology Support Program (2024ZYD0113, 2023YFH0069, 2023NSFSC0028), Scientific Research Project of the Sichuan Provincial Health Commission (23LCYJ040), Sichuan Provincial Cadre Health Project (ZH2024-1501), Luzhou Government-Southwest Medical University Cooperation Project (2024LZXNYDJ005) and Southwest Medical University Project (2021ZKZD013), and Luzhou Science and Technology Program (2022-JYJ-158).
Supplementary Material
Supplementary Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.