
Abstract
Abstract
The development of new therapeutic strategies, such as monoclonal antibodies directed against human epidermal growth factor receptor-2 (HER2), has offered new hopes for women with early breast cancer whose tumors overexpress HER2. We retrospectively analyzed the population-based data of Breast Cancer Registry of Palermo in 2004–2006, and selected 1401 invasive breast cancer cases, nonmetastatic at diagnosis, having HER2/neu oncogene expression determined. We have correlated this information to age, tumor stage at diagnosis (TNM), nodal involvement, and receptor status (ER and PgR). Survival analysis was conducted dividing the patients in two different groups according to date of diagnosis: one group diagnosed in 2004 and a second group in 2005–2006. In the 460 cases of 2004, nodal involvement, receptor status, age at diagnosis and TNM maintained a strong predictive value (p < 0.0001). In this group of patients, overall survival was significantly different according to the HER2 expression levels (p = 0.001). In the second group of patients (941 incident cases in 2005–2006) there was a statistically significant survival difference comparing patients with high levels of HER2 expression treated with trastuzumab versus those untreated (p = 0.006). Our data show that elevated levels of HER2 are a negative prognostic factor. In addition, patients overexpressing HER2 show a significant increase of overall survival when treated with trastuzumab.
Introduction
In Italy, breast cancer ranked first in number of cases newly diagnosed in 2003–2005, and it was the first leading cause of death from cancer in the female population. Incidence is increasing principally among young women but mortality declines with age (Epidemiologia e Prevenzione, 2009; http://www.epidemiologiaeprevenzione.it). Actually, about 50% of breast cancers are diagnosed at early stage (stage 0 or I) (Working AIRTUM Group, 2009). However, despite advances in early detection and in understanding the molecular bases of breast cancer, about 30% of these patients with early-stage breast cancer have a recurrent disease (EBCTCG, 2005; Piccart-Gebhart et al., 2005; Romond, 2005).
The development of new therapeutic strategies, such as monoclonal antibodies directed against human epidermal growth factor receptor-2 (HER2), holds new hopes for women with early and advanced breast cancer whose tumours overexpress HER2. The human epidermal growth factor receptor 2 (HER2) is an oncoprotein composed of an intracellular tyrosine kinase domain, a short transmembrane section, and an extracellular ligand-binding region (ECD, p105). Overexpression of the HER2 protein, which occurs predominantly through the amplification of the her-2/neu oncogene, is implicated in malignant transformation and is being found in 20–25% of breast cancers (Coussens et al., 1985; Slamon et al., 1987). Several studies have indicated that this alteration is associated with greater biological aggressiveness and poor prognosis of breast cancer (Slamon et al., 1989).
Trastuzumab, a humanized monoclonal antibody directed against HER2, has demonstrated antitumor activity in metastatic disease in breast cancer patients previously treated with chemotherapy (12–15% response rate). The addition of trastuzumab to chemotherapy, in the first-line setting, was also associated with a longer median survival time than chemotherapy alone (Joensuu er al., 2006). These results eventually led to an increased use of trastuzumab in clinical practice.
In this retrospective study we have evaluated, in a large group of breast cancer patients having HER2/neu oncogene expression determined (data from a population-based registry), the potential impact of trastuzumab addition to conventional therapy on the overall survival, and we have correlated these data with other clinical and biopathological variables.
Materials and Methods
Patients and methods
A total of 2057 breast cancer cases were collected from the database of the Palermo Breast Cancer Registry between January 2004 and December 2006 (follow-up at the first of January 2010).
Palermo Breast Cancer Registry (BCR-PA) is a population-based registry covering a population of about 1.2 million residents of the Palermo province in Italy. The BCR-PA is a “high-resolution” specialized registry whose information system couples active case ascertainment with extensive collection of clinico–pathological data [age, tumor stage at diagnosis (TNM), nodal involvement, and receptor status ER], as well as follow-up and survival information for each incident case.
For the purpose of this analysis we selected 1401 invasive breast cancer cases, nonmetastatic at diagnosis, having HER2/neu oncogene expression determined.
HER2 status of tumors was assessed using either an immunohistochemistry (IHC) method and/or a gene amplification method based on a fluorescent in situ hybridization (FISH) technique. Tumors were classified as HER2 positive if they had 3+ staining on IHC and/or gene amplification by FISH. Tumors were classified as HER2 negative if they did not exhibit either staining by IHC and or gene amplification by FISH. Tumors exhibiting 2+ staining by IHC that was not accompained by confirmatory FISH results were excluded from the analysis.
Statistics
The overall survival time was measured from the diagnosis of breast cancer to death from any cause and was estimated according to the Kaplan-Meier method. For all analysis, time was censored at the last follow-up date if no event/death was observed. Differences in time distributions were evaluated using the log-rank test (Kaplan and Meier, 1958). Patients were classified in two different groups: one group diagnosed in 2004 and a second group in 2005–2006 when the indications for the use of trastuzumab changed.
HER2-positive patients received trastuzumab treatment for an average of 12 months.
Results
Patients included in this study were retrospectively selected from the population-based incident cases of BCR-PA between January 2004 and December 2006 (n = 2057).
Cases with metastatic breast cancer at diagnosis (n = 154), cases who had HER2/neu oncogene expression not evaluated (n = 354) or tumors exhibiting 2+ (n = 148) HER staining by IHC that was not confirmed by FISH technique were excluded from the study.
The characteristics of the 1401 cases include in the study are summarized in Table 1.
Selected cases were classified in two different groups according to date of diagnosis: one group diagnosed in 2004 (n = 460) and a second group in 2005–2006 (n = 941), as reported above.
Data on adjuvant treatment are not reported but, all patients with HER2-positive disease who received first-line trastuzumab treatment received concurrent chemiotherapy.
Our data show that 80 (17.4%) patients diagnosed in 2004 and 214 (22%) diagnosed in 2005–2006, respectively, had a HER2-positive disease. Median age was similar among patients diagnosed in 2004, but was lower in patients diagnosed in 2005–2006 with HER2 positive disease who received first-line trastuzumab.
A higher percentage of stage III, estrogen receptor tumors negative and positive lymph nodes was found in patients who had HER2-positive disease respect to HER2-negative cases.
Table 2 shows the characteristics of 245 premenopausal patients (age <50) diagnosed in 2005–2006. In this group of patients HER2 expression and/or trastuzumab treatment are correlated with tumor stage (TNM) and receptor status (ER). The percentage of patients in advanced stage (II or III) who had HER2-positive disease treated with trastuzumab is higher in respect to patients who were HER2-positive untreated and negative. Also in this group the percentage of patients estrogen receptor negative who had HER2-positive disease is higher with respect to patients HER2-negative.
Survival analysis was conducted, in the 1401 cases, classifing the patients in the two groups according to the date of diagnosis.
In the 460 cases diagnosed in 2004, age at diagnosis, receptor status, nodal involvement, and TNM maintained a strong predictive value (p < 0.0001) (not shown). Moreover, in this group of patients, survival was significantly different according to the HER2 expression levels (p = 0.001) (Fig. 1). No patient of this subgroup received adjuvant trastuzumab.
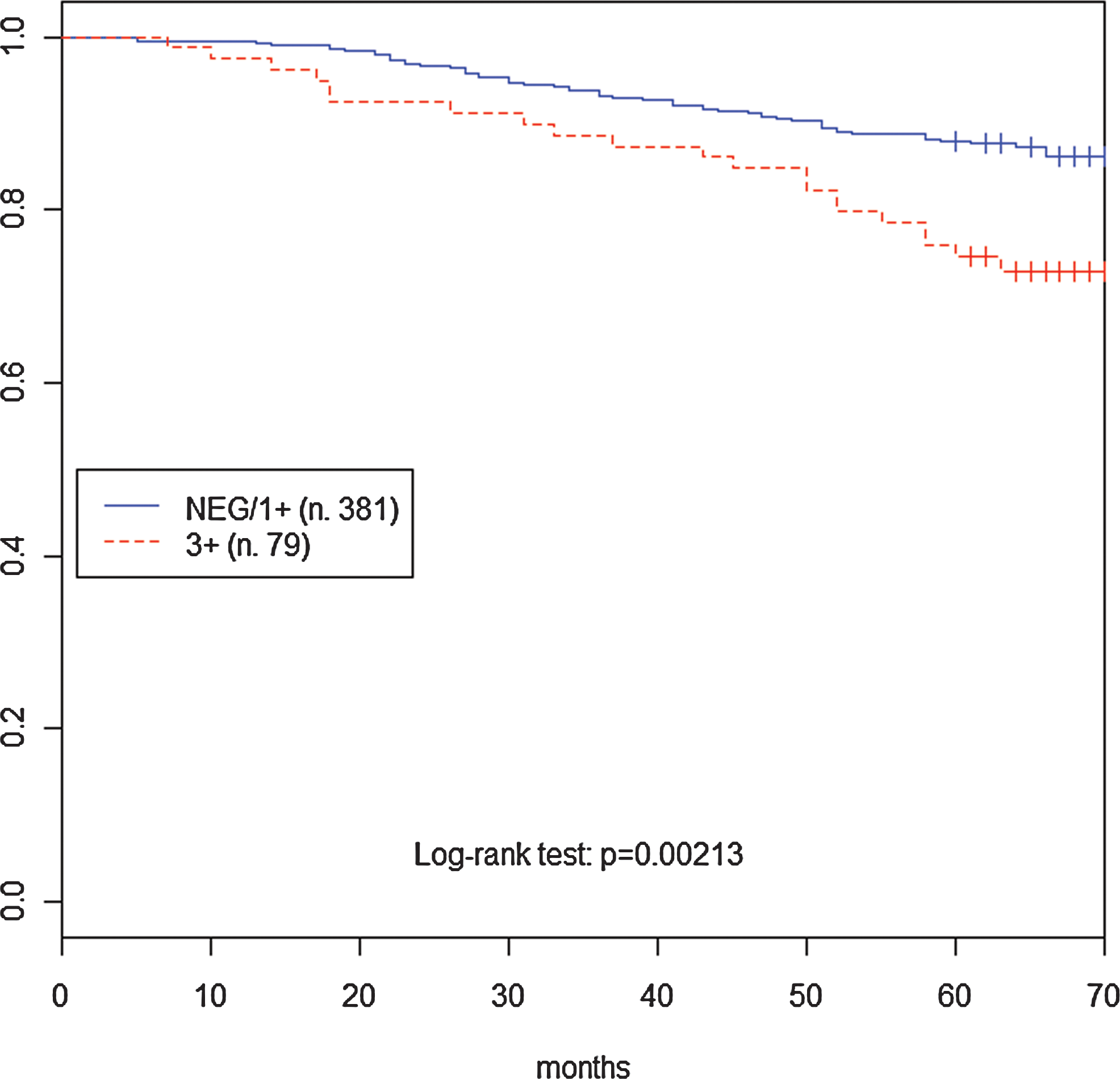
Overall survival of cases 2004 stratified by HER2/neu status.
Among the 941 incident cases diagnosed in 2005–2006 HER2-positive disease treated with trastuzumab showed a better survival with respect to untreated patients (p = 0.0036) (Fig. 2). Interestingly, patients with HER2-negative value had an intermediate survival.
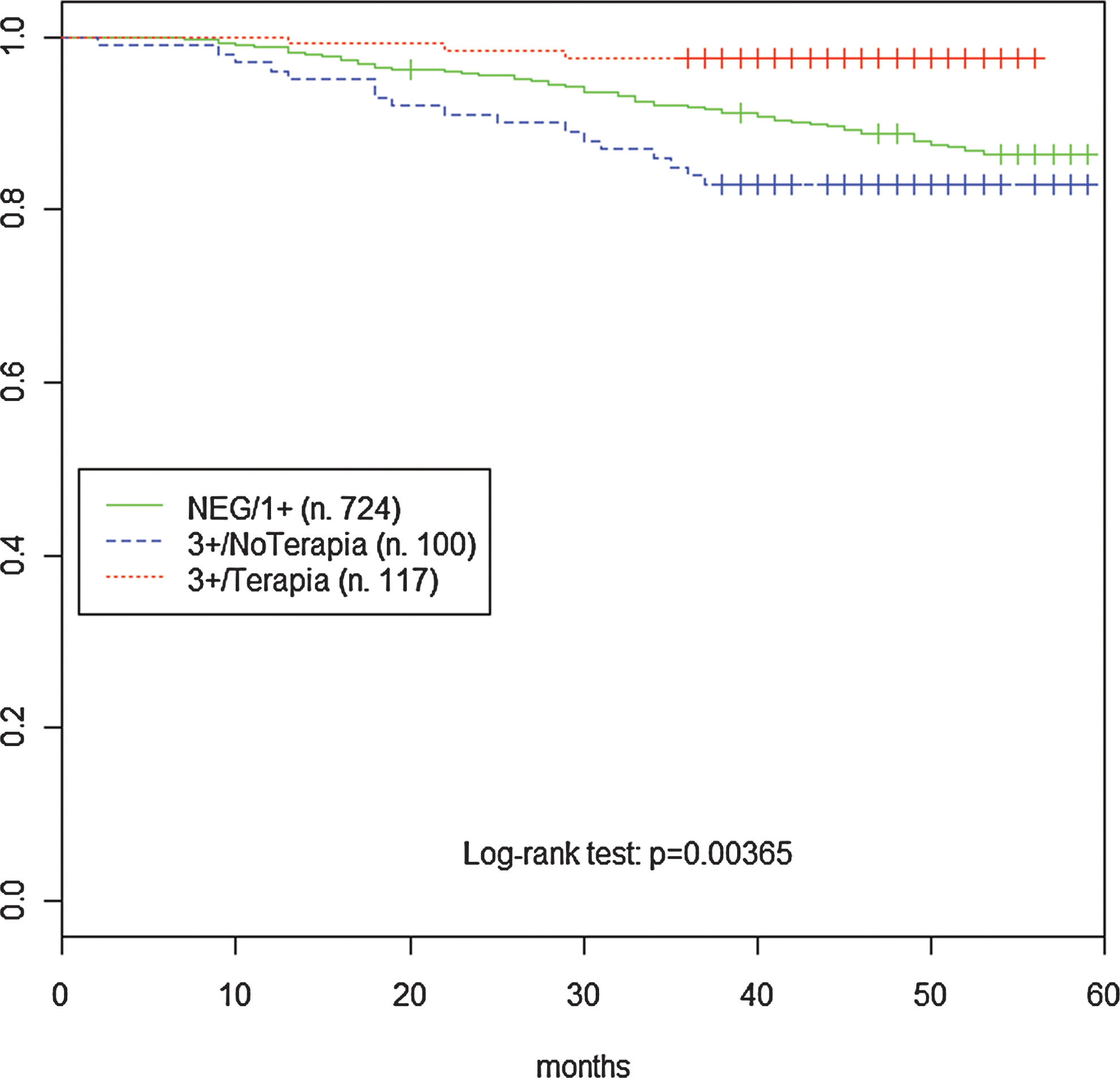
Overall survival of cases diagnosed in 2005–2006 stratified by HER2/neu status.
Treatment with trastuzumab improves survival of HER2-positive patients in all stages (not shown). Conversely, HER2-positive patients who did not receive trastuzumab showed a different survival according to TNM stage at diagnosis (Fig. 3).
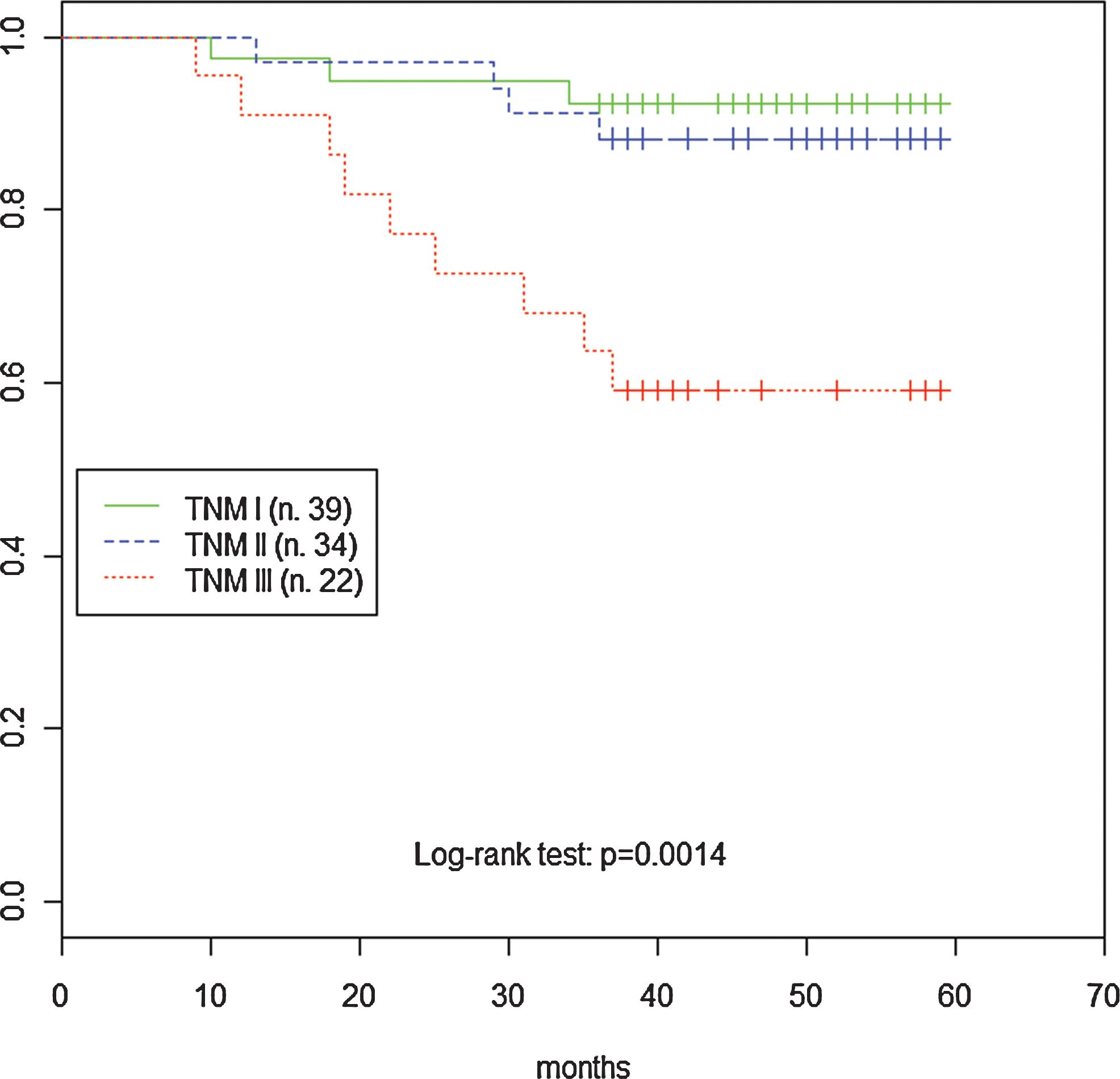
Overall survival of patients diagnosed in 2005–2006 who have HER2/neu positive but untreated with trastuzumab stratified by TNM status at diagnosis.
Finally, in a subgroup of patients with age <50 years overexpressing HER2 the effect of trastuzumab on overall survival was not observed (p = 0.185) (Fig. 4).
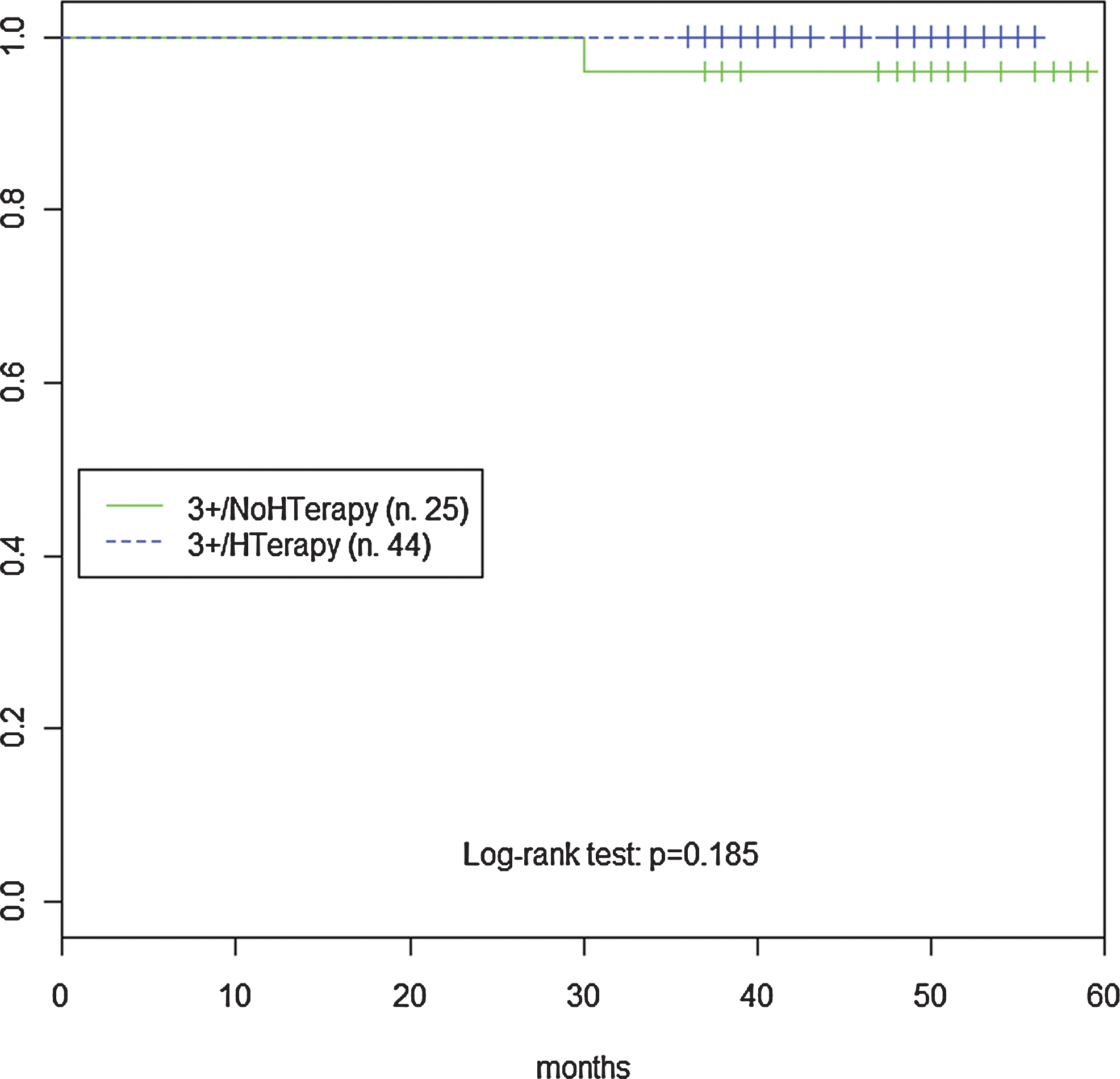
Overall survival of patients age <50 years with HER2/neu positive treated or untreated.
Discussion
This study confirms that HER2 overexpression affects the overall survival of patients with primary breast cancer. In our data, patients with HER2-positive tumors were associated with a worse prognosis compared to HER2-negative, in the population incident breast cancer diagnosed in 2004 (p = 0.001).
Data presented at the ASCO Annual Meeting have raised questions about the accuracy of current methods to assess HER2 status (acta ASCO 2007; http://www.asco.org/). On the other hand, recent studies show that not all HER2-positive patients respond to trastuzumab, presumably because not all patients who receive the treatment are truly overexpressing HER2, or because some proportion of those that do overexpress HER2 also signal through other pathways that are not effectively antagonized by trastuzumab. Interestingly, the percentage of HER2-positive breast cancer in the province of Palermo is lower than that reported by other studies on primary breast cancer (20 vs. 25%). A possible explanation for the lower percentage of HER2-positive tumors in our population comes from recent studies on the protective effects of Mediterranean diet, particularly the ability of EVOO-derived polyphenols, from the extra virgin olive oil, to inhibit HER2 activity by promoting the proteasomal degradation of the HER2 protein itself (Sant et al., 2007). As an alternative, this difference could be ascribed to a distinct selectivity of the analysis (immunohistochemistry and/or gene amplification) to determine HER status.
As expected, overexpression of HER2 is also associated with late stage at diagnosis, nodal involvement and ER status. These results are consistent with literature that reports an increased expression of HER2 as associated with a more aggressive phenotype in primary breast cancer (Sorlie et al., 2003; Zarcone et al., 2009).
The impact of trastuzumab therapy on overall survival is documented in 941 incident cases diagnosed in 2005–2006. In HER2-positive patients who received trastuzumab as adjuvant therapy we observed an increase in overall survival with respect to untreated patients (p = 0.0036). Despite trastuzumab treatment was associated with a longer overall survival in HER2-positive patients, we acknowledge that this evidence is weakened by a number of bias inherent with the retrospective nature of the study, includingthe short follow-up and an average age lower in women with HER2-positive who received trastuzumab than those with HER2-negative disease.
We also report that trastuzumab treatment does not affect survival in patients age <50 years overexpressing HER2. To explain this seeming discrepancy, many confounding factors can be taken into account, such as stage at diagnosis and/or the effect of combined use of tamoxifen and trastuzumab as reported in the literature (Bender and Nahta, 2008; Huang et al., 2010; Roukos, 2010), or an inadequate period of follow-up to discriminate a survival difference in younger patients.
Overall our data show that elevated levels of HER2 represent a negative prognostic factor. In addition, patients overexpressing HER2 show a significant increase of overall survival when treated with trastuzumab. Several questions, however, remain open on use of trastuzumab: high costs of treatment, side effects (cardiotoxicity), drug resistance and duration of treatment. Finally, longer clinical trials are needed to determine the incidence of brain metastases in primary breast cancer patients treated with trastuzumab.
Footnotes
Acknowledgments
We thank all the local institutions, physicians, and personnel who contributed to this work with the aim to achieve a deeper knowledge of breast cancer epidemiology in our region.
Author Disclosure Statement
No competing financial interests exist.