
Abstract
Abstract
Genomic Medicine aims to improve therapeutic interventions and diagnostics, the quality of life of patients, but also to rationalize healthcare costs. To reach this goal, careful assessment and identification of evidence gaps for public health genomics priorities are required so that a more efficient healthcare environment is created. Here, we propose a public health genomics-driven approach to adjust the classical healthcare decision making process with an alternative methodological approach of cost-effectiveness analysis, which is particularly helpful for genomic medicine interventions. By combining classical cost-effectiveness analysis with budget constraints, social preferences, and patient ethics, we demonstrate the application of this model, the Genome Economics Model (GEM), based on a previously reported genome-guided intervention from a developing country environment. The model and the attendant rationale provide a practical guide by which all major healthcare stakeholders could ensure the sustainability of funding for genome-guided interventions, their adoption and coverage by health insurance funds, and prioritization of Genomic Medicine research, development, and innovation, given the restriction of budgets, particularly in developing countries and low-income healthcare settings in developed countries. The implications of the GEM for the policy makers interested in Genomic Medicine and new health technology and innovation assessment are also discussed.
Introduction
P
Economic evaluation aims to assess whether the financial investment in specific health care interventions will provide “value for money” in terms of costs and therapeutic consequences of new versus existing interventions, and herewith inform decision makers on achieving policy aims within the healthcare system. So far, and for the policy makers to access the value of innovative interventions, the commonly used investigation is implemented via the determination of the incremental cost effectiveness ratio (ICER) (O'Brien and Briggs, 2002). ICER is the ratio of the average per-patient incremental cost (ΔC) of one intervention divided by an incremental health gain (ΔE), such as an additional stroke prevented, a case of cancer diagnosed, or gain of a Life Year (LY) or, primarily, an additional Quality Adjusted Life Year (QALY). Despite their shortcomings, QALY represents one of the widely accepted measures used to consider the ability of an intervention to extend life and to improve the quality of life for the patients.
In accordance with the current theory, if ICER is below a pre-determined amount a policymaker was willing to pay for an additional QALY, the new intervention is a “cost-effective option” and meets one of the criteria for reimbursement by the payers (McCabe et al., 2008) (Fig. 1). It must be highlighted that this amount of money is not fixed (and may vary within a specific range), when taken into account other criteria for the reimbursement process, such as the particular features of the condition, the availability and clinical effectiveness of other interventions, the size of population who will use the technology, the innovative nature of the technology, the wider societal costs and benefits, equity concerns, the culture of every country, and the available budget and, when appropriate, the reference to previous appraisals. Hence, it is known that it is necessary to consider the willingness to pay for a QALY in a disease and country-specific context, taking also into account the age and the gender of beneficiaries, their deservedness, and other ethical issues.
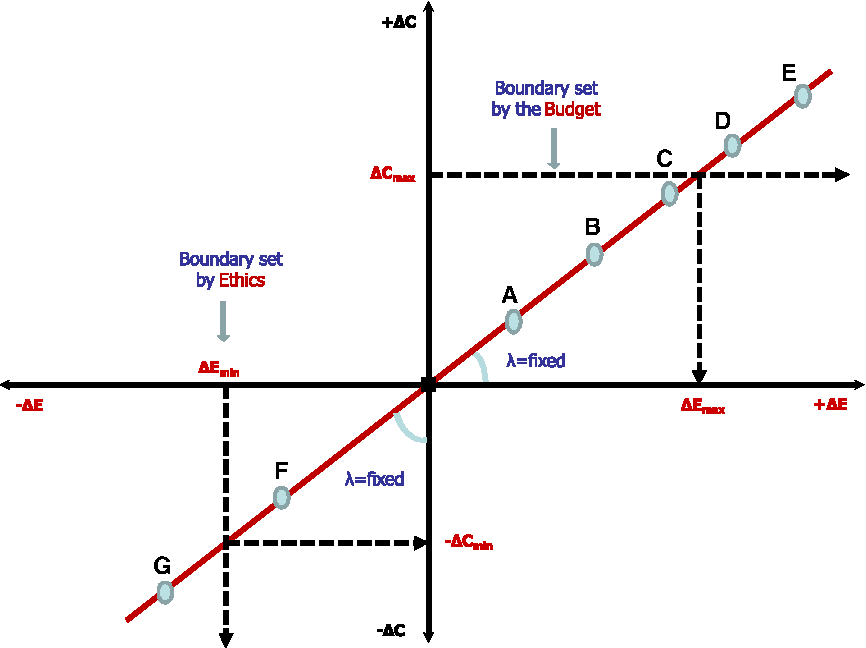
The basis of the proposed Genome Economics Model (GEM). The classical cost-effectiveness plane is depicted. Various health interventions are indicated as A–G, lie on the straight line, and can be all adopted and reimbursed by the national healthcare systems, in accordance to the classical model, which assumes unlimited budget availability. According to GEM, interventions such as “A” or “B” represent “average cases” with increased ΔE and reciprocally higher costs, which together with “innovative” technologies, such as “C” (e.g., those described in pharmacogenomics and Genomic Medicine, with a high ΔE), could be reimbursed by national healthcare systems. However, according to GEM, interventions with a much higher ΔE, such as “D” and “E” also bear higher costs, that make them unaffordable for adoption in a real-life situation, where unlimited budget availability is never the case. Similarly, interventions, such as “G”, represent probably a technology with a cost-saving profile, but also less effectiveness, which again make it ineligible for adoption.
Because the above approach does not incorporate affordability when making judgments about cost effectiveness, an additionally separated budget impact analysis should also be implemented to determine the economic burden of short and medium-term effects on budgets and other resources to reach a final conclusion. Nonetheless, a “cost-effective” intervention, determined by the approach described above, may not necessarily be affordable from an economic point of view and the criteria for the final verdict of adoption or rejection frequently remains unclear. In addition, other concerns have also been raised regarding the methodological limitations of the present analysis in this existing form ( Barton et al., 2008; Donaldson et al., 2002a; 2002b; Eckermann et al., 2008; Gafni, 1998; Whitehead and Ali, 2010).
One of the main concerns, amongst others, is the fixed threshold (even in a disease-specific context and/or determined in a range) approach might lead to controversial decisions (Birch and Gafni, 2006; Gyrd-Hansen, 2005; Sendi et al., 2002) and increased expenditures (Gafni and Birch, 2006). The classical theory assumes that all “cost-effective” interventions with increased effectiveness compared with the standard (conventional) intervention could or should be reimbursed by the payers. In that sense, the classical approach compares the ICER against the willingness to pay, a budget impact analysis is conducted independently, and an automatic/arbitrary adjustment of budget in the cost of new technology is assumed. In this case, there is not a clear linkage between the budget affordability of a health care system and the cost-effectiveness approach.
Nonetheless, even if the budget is not fixed, it is reasonable to assume that there is an actual boundary, indicative of the budget limit. On a pragmatic basis, for instance in the UK, the government could finally judge if a particular intervention is unaffordable for the system, even though it had been judged previously as a “cost effective” option. On the contrary, where a new technology is far less effective compared with the standard one, the classical model, at least in theory, assumes that “infinitively” less effective technologies could be adopted based only on cost criteria. Even in the case of developing countries, there are important moral and ethical issues in the treatment of patients. which make the possibility to adopt a new poor, in terms of effectiveness, technology unlikely, despite their cost-saving profile (Fig. 1).
To deal with this issue, a modified version of the classical model has been also proposed. Based on real life data, it has been estimated that the money which a society is willing to save in order to sacrifice a QALY is much greater than the willingness to pay for a QALY by 2–6 times on average (for details of this concept, see O'Brien et al., 2002). Even in this case, there should also be a boundary that prevents the adoption of a very poor technology in terms of effectiveness. Those boundaries described above are not formally taken into consideration in the classical model. In addition, the classical theory assumes that the willingness-to-pay for a QALY is independent of the actual difference in effectiveness between different health technologies even within the same disease-specific context. In that sense, economic evaluation does not differentiate between a truly innovative health technology, a “me-too” health technology, or even a generic health technology and reimburse proportionally equally each one of them.
Here, we provide an alternative, less restrictive model for economic evaluation for healthcare decision-making process, which takes into account the budget constraint criteria and relaxes the assumption that the willingness-to-pay is fixed and irrespective of the actual amount of incremental effectiveness among interventions. This model can be readily applicable for Genomic Medicine interventions and will be described hereafter as the “Genome Economics Model” (GEM).
Methods
Description and rationale of the model
The basic concept of GEM is presented in Figure 1. In accordance with GEM, a comprehensive decision-making process should formally take into account both the real therapeutic benefit in a patient's life and at the same time the payer's budget. Hence, technically, one should add in the decision-making process as regards the cost effectiveness of a new technology two boundaries: (a) the right boundary which is imposed by the budget constraint (Fig. 1; upper right quadrant) and, (b) the left boundary which is determined by ethics and standard medical practice (Fig. 1; lower left quadrant).
GEM implies that ΔCmax represents the maximum amount of money per patient that could be spent by the payers only if a certain therapeutic gain from an innovative health technology was met by health providers. It must be highlighted that this amount of money (or the range into which it is supposed to fall) has to be estimated based on: a) the prevalence and the incidence of the disease, b) the available total budget for a specific disease, and c) the estimated market penetration of the new technology in the future. Hence in our proposed GEM model, in contrast with the classical model, the society defines ex-ante
(a) what is expected to be the upper limit of “innovation” in terms of effectiveness gains,
(b) what is the lowest acceptable effectiveness that could be accepted and judge ex-post every new technology within two boundaries,
(c) the maximum amount of money is willing to invest or save within two boundaries. Furthermore, the GEM model, contrary to the classical model, does not conduct a separate cost-effectiveness and budget impact analysis, in order to avoid the problem of technologies that are “cost-effective” but not “cost-affordable.” Every cost-effective technology in the GEM model meets also the cost criteria.
As such, health technologies “D” and “E” do not represent a cost-effective option anymore according to the GEM model, unless the budget is expanded or the costs of those interventions are lowered to meet the cost threshold (Fig. 1). In addition, ΔEmin represents the lowest acceptable level of effectiveness that could be offered by a new health technology in order to be accepted by the healthcare system. Hence, option “G” will be also rejected, according to GEM. In addition to those described above, contrary to the classical economic evaluation model (for details, see Fragoulakis et al., 2015), the GEM presents the variability of the actual incremental effectiveness of a new intervention, in correlation with the willingness to pay for a QALY in a formal manner (Fig. 2). In this context, every potentially new unit of effectiveness that could be gained from future technologies has a different perceived value for the patients, the scientific community, and the stakeholders.

Cost Effectiveness Plane in the GEM versus the Classical Model. In the classical model, λ is constant, depicted as a straight line. However, in GEM, λ is variable, spanning from technologies with a very small innovation (“Me too”) with a reciprocal small average λ to very innovative technologies with a high average λ. ΔE = difference in the effectiveness between the standard and the new intervention, depicted in the horizontal axis; ΔC = the difference in the total cost between the standard and new intervention per patient, depicted in the vertical axis; ΔCmax = the maximum available budget (per patient) is willing to afford the budget holder to capture the maximum expected effectiveness that can be additionally reimbursed (= ΔEmax); “marginal utility” referring to the additional satisfaction the society gains from the production of one more unit of effectiveness.
For a very small difference between two health technologies (i.e., “me too” intervention), and without any meaningful differentiation from existing interventions, the average willingness to pay for a QALY is expected to be low (Fig. 3). For more innovative interventions with some differences in terms of effectiveness, (“small/fair” interventions), a higher average willingness to pay for a QALY (but also smaller than those offered by the classical model) can be expected, also in accordance to practical evidence (Kvamme et al., 2010). For innovative interventions with significant difference in terms of effectiveness, the average willingness to pay for every unit of QALY is expected to be very high in comparison with classical model.
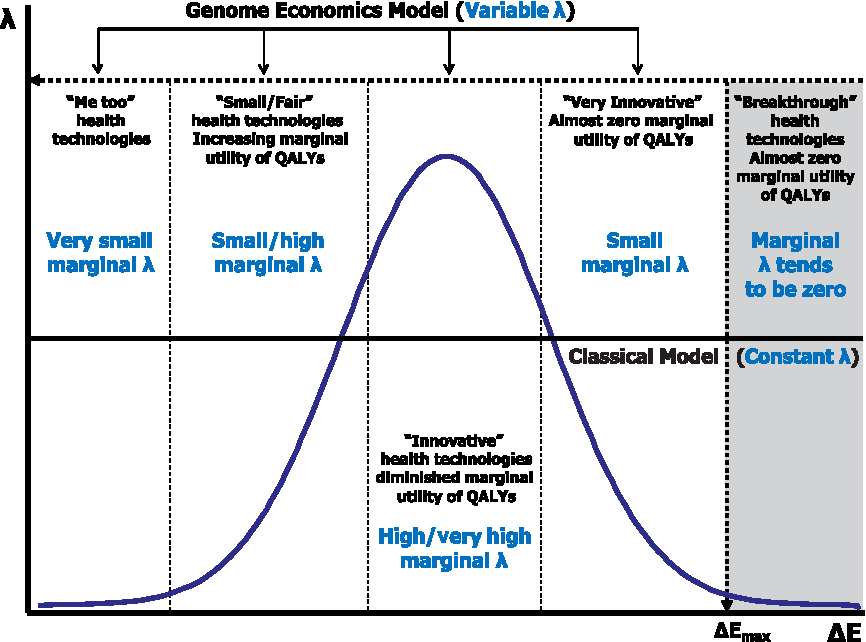
Willingness-to-Pay as a function of ΔE in GEM versus the classical model. In the classical model, λ is constant, depicted as a straight line. However, in GEM, λ is variable, and adopts a bell-shape appearance. Again, technologies with a very small innovation (“Me too”) have reciprocally a very small marginal λ compared with the classical model. Technologies with fair/small benefits have higher but also small marginal λ compared with classical model. In the same concept, innovative technologies have very high λ (determined by the difference in each point of the GEM minus the classical model), while very innovative technologies falls again to small marginal λ. As ΔE increases further, beyond the ΔEmax, λ tends to zero, since the available budget has been exhausted.
As the difference in effectiveness increases further (breakthrough technology), we meet the budget constraints criteria and, as such, we are unable to reimburse this technology further, the average willingness to pay is getting lowered, but the effectiveness of the adoption of this technology is offered by the health provider on behalf of the society. As such, the shape of willingness to pay for a QALY as the potential difference in effectiveness increases, resembles a bell-shape distribution, contrary to the classical model, in which willingness to pay is a straight line, determined by arbitrary assumptions, made by policy makers or the literature (Fig. 3).
Finally, the new model is different compared with the classical one, in the sense that it drives healthcare providers to increase the effort for favorable treatments, “punishes” the less productive ones, and “rewards” the true innovation, ensuring at the same time the sustainability of the healthcare system.
Implementation of the model
To demonstrate the usefulness of the proposed new model in pharmacogenomics and Genomic Medicine interventions, we have employed GEM to a recently published real-file example of pharmacogenomic (PGx)-guided versus non-pharmacogenomic (N-PGx)-guided warfarin treatment of elderly Croatian patients, who develop ischemic stroke predominantly due to atrial fibrillation (Mitropoulou et al., 2015). The model was populated with the cost data from the Croatian public tariff lists and current treatment guidelines on patient management. The main inclusion and exclusion criteria, the number or patients, and clinical features and genotyping are available elsewhere (Mitropoulou et al., 2015). The study was conducted in accordance with the Declaration of Helsinki, and all patients give written informed consent in order to participate in the study. The present model is only an indicative example, and has been used only for illustrative purposes.
Results
We have previously shown (Mitropoulou et al., 2015) using the classical economic evaluation model in a one-year time horizon, that the probability of PGx-guided warfarin treatment being cost-effective increases significantly at a willingness to pay threshold in the range of €40,000–€50,000 per QALY, used in many jurisdictions and, notably, at €60,000 per QALY, its probability of cost-effectiveness gets higher than 80% (Mitropoulou et al., 2015). In particular, our findings indicated that the total cost per patient was estimated at €538.7 for the PGx-guided group vs. €219.7 for the control group and total QALYs was estimated at 0.954 and 0.944 for the PGx-guided and the control groups, respectively (Mitropoulou et al., 2015). The incremental cost-effectiveness was estimated at €31,225/QALY (ΔC/ΔE = €319.4/0.01023). Based on data availability and related calculations, a specific cost-effectiveness acceptability curve for PGx vs. non-PGx intervention is produced (Fig. 4, depicted in blue).
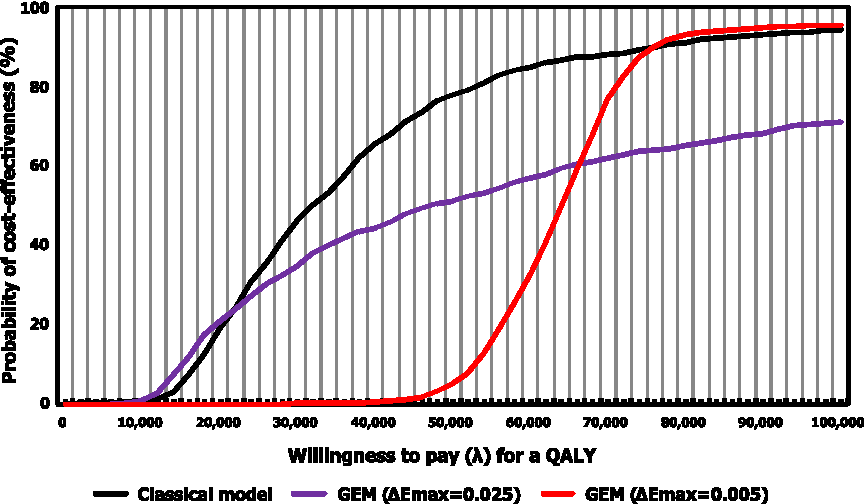
Cost effectiveness acceptability curve for PGx versus N-PGx guided treatment for the GEM and Classical Model for two different scenarios for ΔEmax. Cost effectiveness acceptability curve for PGx vs. N-PGx guided treatment for the classical model (depicted in black) and for two different scenarios for GEM, namely ΔEmax = 0.025 (depicted in red) and ΔEmax = 0.005 (depicted in blue). See also text for details.
In the case of the GEM, we assumed two hypothetical scenarios:
(a) ΔEmax = 0.025, and (b) ΔEmax = 0.005 (Fig. 4) lying at both sides of the actual difference (ΔEmax = 0.01023).
For illustrative purposes a third scenario with (c) ΔEmax = 0.01023 was also determined to indicate differences between the classical (scenario “c”) and the new (scenarios “a” and “b”) model, Fig. 5).
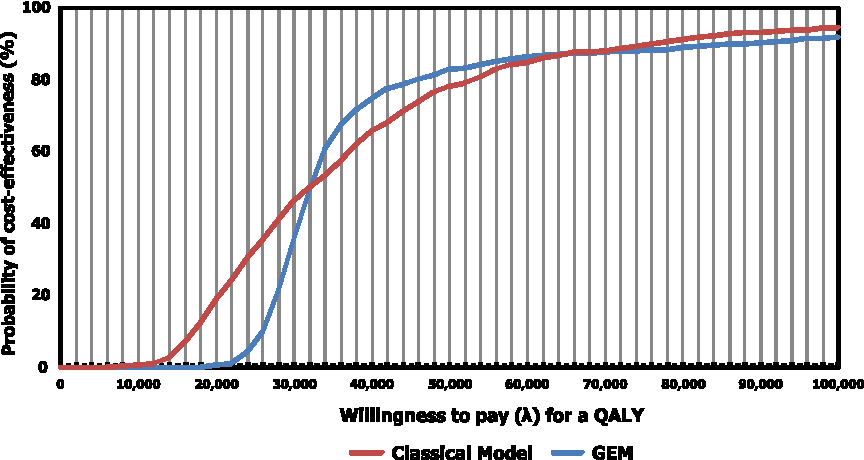
Cost effectiveness acceptability curve for PGx vs. N-PGx guided treatment for the GEM and Classical Model based on the main results of the Croatian population. Cost effectiveness acceptability curve for PGx vs. N-PGx guided treatment for the GEM and classical model for ΔEmax = 0.01023.
It must be noted that these figures are indicative to highlight that different acceptability curves could be produced based on different assumptions. These assumptions represent decisions adopted by the policy makers.
The scenario with ΔEmax = 0.025 represents an “ambitious” expectation and probably fits to the profile of the developing countries, since it requires that the PGx must have a fair difference in effectiveness (0.025 QALYs) gained against N-PGx in order to invest all the additional available amount of money. On the contrary, the scenario with ΔEmax = 0.005 represents a society with low expectations from future innovations, since the available amount of money will be all invested even if the new technology (PGx) has only an insignificant incremental difference of 0.005 QALYs gained against N-PGx.
The present analysis of GEM indicates that the probability of a new technology being cost-effective is a function not only of a disease-specific willingness to pay as previously mentioned by the literature, but also the willingness of the society to transfer resources (and to which extent) from “me-too” health technologies to truly innovative ones taking. into account the available budgets.
Discussion
As medical research is one of the leading priorities in the society, it is essential to improve the lives of patients and, at the same time, the economy as a whole. On the other hand, medical expenditure is expected to be covered by the Insurance Funds and usually leads to an uncontrolled growth in health care expenditure. In view of the limited resources, especially in developing countries and low-resource environments (Snyder et al., 2014), economic evaluation provides a criterion for the final decision concerning the adoption of certain new and innovative technologies. The classical approaches have, notwithstanding, some inconsistencies and drawbacks.
In this article, we propose an alternative methodological approach, taking into account the budget constraint, the effectiveness of a new technology, and social preferences expressed by the willingness to pay in a flexible way. There are some distinct differences between the proposed (GEM) and the classical models. In the case of GEM, the maximum effectiveness that could be accepted by payers for reimbursement is determined before any new technology is introduced in the healthcare system, which is logical, considering the fact that the budget constrains vary between different countries. The model presented here describes, in a dynamic manner, the link between the willingness to pay threshold towards the budget limit. Thus, our model enables, at the same time, the combination of cost-effectiveness and budget impact analysis.
In an attempt to describe the real world situation practically, the GEM relaxes the “fixed” and/or disease-specific assumption of willingness to pay for a QALY, allowing a flexible, upper bounded, budget. Furthermore, the model encourages the determination of willingness to pay to be different across different treatment areas, taking into account the differences in “production” of a QALY amongst patients groups (e.g., cardiovascular patients, oncology patients), and even among the same patient groups but different healthcare systems. This argument of specific context and varying determination of willingness to pay is also in accordance with related literature (Bridges et al., 2010; Zhao et al., 2011). This model and its whole concept shares the basis of methods used in the microeconomic theory, where the budget constraints and the preferences combined simultaneously at the same model.
However, GEM is also a simplification of the process it tries to emulate, and it is therefore necessary to make assumptions and to accept limitations, which is common in similar models. For instance, the model demands the explicit mapping of preferences in a disease-specific context to reach some meaningful conclusions. Inevitably the problem becomes much more complex when taking into account the uncertainty of variables. Thus, further uncertainty is evident, concerning for instance the market penetration rate of innovative technology and the prevalence of a specific disease today and in the future. In addition, GEM assumed that the budget is exogenous and was set by the budget holders. Indeed, budget allocation lies on historical and political background in each country, and the optimal reallocation across healthcare sections or is not always desirable, when sacrifices the transparency or consistency of decision making, the equality, or other ethical issues (Schwappach, 2002). In that sense, the present model does not address the question of how to allocate available healthcare resources to different diseases based on a common measure for health. In order to do so, several limitations must be addressed, which have already been mentioned in the literature and is out of the scope of the present work (Birch and Gafni, 2006; Sendi et al., 2002).
In this article, our model is based on the economic evaluation of a specific disease context and for innovative interventions with greater effectiveness compared with the standard ones, when considering the introduction of a new treatment, while the case of decrementally cost-effective medical technologies, which is probably of particular interest in developing countries, is still missing. It must be highlighted that the clinical determination of the “innovation” is beyond the scope of this article and this term is used only from a technical point of view, to indicate health technologies that provide greater effectiveness based on statistical measurements. The whole concept of innovation is controversial and still scientifically open (Vernon et al., 2009) and several attempts have been made to provide an overview of how innovation is currently valued amongst health care systems today.
Thus, the solution of GEM only offers a local maximum determined by the de facto budget availability in a specific disease context. The aggregate sum of costs and effectiveness across several disease areas does not necessarily represent the overall maximum, as the perceived importance by policy makers and society for different QALYs have not been fully addressed and the budget cannot be fully reallocated automatically across different therapeutic areas. Nonetheless, we argue that the “health optimization problem given a fixed budget” for the entire society, despite appealing as a mathematical problem in theory, cannot be so easily addressed in a real world setting.
Uncertainty (Ramsey et al., 2005), lack of data or knowledge for preferences (Weyler and Gandjour, 2011), lack of training of policy makers (Veney et al., 1997), established status quo, and other policy and public health-related issues, make the quantitative determination of constraints and the application of prominent instruments, such as mathematical programming, more difficult than GEM (Flessa, 2000). In this context, it must be noted that the determination of a general willingness to pay for a QALY irrespective of the disease as representative of social preferences, requires not only a scientific approach to evaluate the opportunity cost between comparable treatments, but also the knowledge of societal utility function and the knowledge of different weights for different QALYs as mentioned before (Wailoo et al., 2009).
If, and only if, the above prerequisites were satisfied, one could estimate the true value of willingness to pay and the desired maximization treatment mix across several disease-specific areas. Despite the fact that mathematical programming could incorporate, in a quantitative form, some restrictions referred to ethical issues, exogenous (not scientific-based) information for the amount of this budget allocation must be also provided by the policy makers as an input in these kind of models.
Implications for policy makers
Based on the GEM model, a simple practical solution for policy makers in our context is outlined in the next steps with a view to GEM's applications:
a) To determine (based on prevalence, incidence, market penetration and the available total budget for a disease), the maximum amount of money that could be invested per patient in the future only in case of specific requirements, in terms of effectiveness, are met; b) To determine the amount of greater-than-the-standard effectiveness, which differentiate amongst “me-too,” “fair,” “innovative,” “very innovative,” and “breakthrough” technologies; c) To determine the maximum amount of effectiveness, which could be sacrificed in the future for cost-saving purposes, compared with the current medical standard, d) To define the amount of money that are willing to save from the least effective but also the least costly option; e) To determine in a quantitative manner the proportional rule for reimbursement across the above-mentioned technologies (even those with greater or less effectiveness). For those technologies with greater effectiveness, the society is f) To assess every future technology in terms of (b) and (c); g) To reimburse these technologies in terms of (e); h) To update periodically all the above when new data becomes available.
It must be highlighted that the actual issue of financial resource management, in practice, is primarily a political issue and requires a knowledge of the politics and sociology of technology and innovation-in-society (Nowotny, 2015; Sclove, 1989). Unfortunately, quantitative methods or logical approaches as those described above are not always adequate to resolve such issues by themselves, and, in many cases, the translation of a theoretical model into a political decision involves other factors that lie mostly outside the province of the academic community. Nonetheless, scientists and technology-driven academic communities can still play valuable roles in shaping the knowledge trajectories from lab to innovation-in-society through greater transparency and a sociological read of the scientific laboratory and practices. In this regard, the readers are referred to the biography and contributions of the Nobel Laureate Frederick Soddy for his works to better understand the science and technology futures (Sclove, 1989), as well as the recent analysis of scientific uncertainty by Helga Nowotny (Nowotny, 2015).
In this context, we argue that decisions as those describe in the abovementioned steps must be carefully assessed from a large panel of experts, including the medical community, the patients, and the governmental stakeholders. The latter is of utmost importance in the case of Genomic Medicine interventions, where policy makers with high power of intervention, such as the Ministry of Health and Payers are often skeptical to adopt such innovative approaches due to the high anticipated costs (Mitropoulou et al., 2014).
It must be also noted that the numerical example presented herein refers to a specific group of patients suffering from a specific disease (atrial fibrillation) and in a specific setting (Croatia). Despite the fact that the results of the analysis only showed a marginal difference in QALYs between PGx- vs. non PGx-guided interventions, intermediate results (percentage of major/minor bleeding, etc.) demonstrated a statistical significant difference in favor of PGx-guided warfarin treatment, at least in terms of effectiveness. Also, a broader time horizon than the one used in the original analysis (1 year) could further (slightly) impact on the results in favour of the PGx-guided treatment group.
Our alternative model, described herein, attempts to unify cost-effectiveness, budget impact analysis, ethical issues, and preferences into a same equation, improving some core drawbacks of the classical model. It must be noted that the potential added-value and novelty of the GEM approach presented in this article can only be understood if compared to other approaches to overcome similar problems (Asaria et al., 2016; Cleemput and Van Wilder, 2009; Culyer et al., 2007; Devlin and Parkin, 2004; Gandjour, 2015; Perleth et al., 2009; Rawlins and Culyer, 2004; Thokala et al., 2015).
The validation of GEM and the estimation of the coefficients with real data sets might be some of the future avenues of research. Finally, although originally proposed for Genomic Medicine interventions, GEM might also be applicable for medical and health interventions other than genomic technologies that warrant further research and consideration.
Footnotes
Acknowledgments
This work was endorsed by the Genomic Medicine Alliance Economic Evaluation in Genomic Medicine Working Group.
Author Disclosure Statement
Nothing contained in this paper is intended to guarantee the appropriateness of any medical treatment or to be used for therapeutic purposes or as a substitute for a health professional's advice. The authors declare no conflict of financial interests.