
Abstract
Abstract
Rheumatoid arthritis (RA), a systemic, chronic, and progressive inflammatory autoimmune disease, affects up to 1.0% of the world population doubling mortality rate of patients and is a major global health burden. Worrisomely, we lack robust diagnostics of RA and its remission status. Research with the next-generation biomarker technology platforms such as glycomics offers new promises in this context. We report here a clinical case–control study comprising 128 patients suffering from chronic RA (80.22% in remission, 19.78% active clinically) and 195 gender- and age-matched controls, with a view to the putative glycan biomarkers of RA as well as its activity or remission status in Han Chinese RA patients. Hydrophilic interaction liquid chromatography–ultra-performance liquid chromatography (HILIC-UPLC) was used for the analysis of IgG glycans. The regression model identified the glycans that predict RA status, while a receiver operating characteristic (ROC) curve analysis validated the sensitivity and prediction power. Among the total 24 glycan peaks (GP1–GP24), ROC analysis showed only GP1 prediction to be highly sensitive with an area under the curve (AUC) = 0.881. Even though GP21 and GP22 could predict active status among the RA cases (p < 0.05), they had lower sensitivity of prediction with an AUC = 0.658. Taken together, these observations suggest that GP1 might have potential as a putative biomarker for RA in the Han Chinese population, while the change in IgG glycosylation shows association with the RA active and remission states. To the best of our knowledge, this is the first glycomics study with respect to disease activity and remission states in RA.
Introduction
R
Although the etiology of RA remains elusive (Majithia and Geraci, 2007; Plenge et al., 2007), genetic predisposition (Eyre, 2012; Goeldner et al., 2010; Majithia and Geraci, 2007; Scott et al., 2013), environmental influences (Majithia and Geraci, 2007; Scott et al., 2013), and lifestyle (Lauc et al., 2010) have been linked to the pathogenesis of RA. Additionally, individual differences in IgG glycosylation pattern have been shown to contribute to the disease manifestation (Menni et al., 2013; Pučić et al., 2011; Zhang, 2006). Minute changes in glycan conformations have been linked to a variety of human autoimmunities such as Wiskott–Aldrich syndrome, cancer, diabetes, cardiovascular, congenital infections, acquired immune deficiency syndrome (AIDS), and immune-related diseases (Menni et al., 2013; Pučić et al., 2011; Zhang, 2006), making glycans as positional prognostic and diagnostic biomarkers due to their variability and innate sensitivity to the physiological changes (Lauc, 2012; Lu et al., 2011) especially in detecting changes in inflammatory diseases such as RA (Lu et al., 2011).
In this study, we quantified plasma IgG N-linked glycans from RA patients and ethnicity-, age-, and gender-matched controls and examined the changes affected by individual glycans (GP1–GP24), their derived traits, and difference in mean glycosylation patterns in RA patients of Han Chinese descent, aiming to ascertain a potential glycan biomarker for RA, with special reference to active and remission states.
Materials and Methods
Participant recruitment
Blood samples were obtained from 128 RA patients (85.16% females with a mean age of 50.39 years; 14.84% males with a mean age of 54.79 years) of Han Chinese residing in Tangshan, Hebei Province, China, who fulfilled the American College of Rheumatology (ACR) classification criteria for RA (Aletaha et al., 2010). We excluded 37 cases (28.91%) who had missing information regarding their disease status from the analysis. The included cases were classified as active RA (19.78%) and remission (80.22%). Remission was defined as <2.6 on the 28-joint Disease Activity Score (DAS28) and was associated with slow or no radiological progression on X-ray/ultrasound/MRI, as suggested by the criteria for remission proposed by the American Rheumatism Association (ARA) (Arnett et al., 1988). Participants for controls were recruited from individuals who underwent routine health checkups at the Jidong Oilfield Hospital, Tangshan, China.
All participants met the following inclusion criteria: (1) no history of somatic and psychiatric abnormalities as registered in their medical records and (2) no history of taking any medication for the past 2 weeks. Participants comprised 195 individuals free from RA (87.69% females with a mean age of 44.58 years; 12.31% males with a mean age of 46.83 years). Individuals suffering from any of the severe diseases, such as cardiovascular, respiratory, genitourinary, digestive, hematic, osteoarthritis, and cancer, were excluded from the analysis.
This study was approved by the Ethics Committee of Capital Medical University, and written informed consents were obtained from all participants before blood sampling.
Analysis of IgG glycans
The N-linked IgG glycan analysis was performed by isolating IgG and then releasing and analyzing the Fc and Fab glycans by hydrophilic interaction liquid chromatography–ultra-performance liquid chromatography (HILIC-UPLC), which was described in detail previously (Huffman et al., 2014). The released glycans were separated into 24 chromatographic peaks (GP1–GP24) (Novokmet et al., 2014). Each peak was then quantified and assigned individual glycan structures (Novokmet et al., 2014). Along with the 24 peaks, an additional 40 derived traits, which represent the average glycosylation features, such as galactosylation, sialylation, and fucosylation, were calculated (Vučković et al., 2015). Normalization and batch correction of UPLC data were detailed in a study by Vučković et al. (2015).
Statistical analyses
Multivariate logistic regression was used to determine association between the 24 GPs and the derived glycan traits (that measure bisecting GlcNAc in core-fucosylated, sialylated, and galactosylated glycans) with disease manifestation after controlling for both age and gender, as well as with active and remission statuses, while controlling only for gender.
A receiver operating characteristic (ROC) curve analysis was performed on each glycan structure individually to validate its sensitivity and prediction power. The benchmark for ROC curve analysis cutoff point was based on the accuracy of the diagnostic test where the measure of 80% and above is a good test (Ebell, 2016; Tape, 2016). In our analysis of active RA state, only gender was controlled as a confounder as it had been shown that remission is associated with gender, but not with age (Cutolo, 2009; Forslind et al., 2007; Saber et al., 2010; Sokka et al., 2009).
Finally, the box plots were used to show the mean difference in IgG glycosylation and derived traits between cases and controls, as well as those between active and remission states.
All statistical analyses were performed using IBM SPSS Statistics for Macintosh (Version 20.0 from IBM Corp, Armonk, NY, USA). All reported p values were two tailed and considered to be statistically significant at p < 0.05.
Results
RA cases and controls
Among the 24 GPs, GP1, GP2, GP22, and GP24 were found to be significantly related to RA status after performing logistic regression. The analysis showed that GP1 (adjusted odds ratio [AOR] 3.49 × 1016; 95% confidence interval [CI] 2.9 × 108–4.2 × 1024; p < 0.001), GP2 (AOR 1.02 × 102; 95% CI 2.79–3.71 × 103; p = 0.012), and GP24 (AOR 5.21 × 102; 95% CI 9.68–2.80 × 104; p = 0.002) had a higher likelihood of occurrence in RA cases, whereas GP22 (AOR 0.02; 95% CI 0.01–0.23; p = 0.039) was less likely to occur in RA cases after controlling for age and gender (Table 1). In the presence of fucosylation in RA, the derived trait Fn total that measures total core fucose had higher odds of outcome in cases than in controls (AOR 1.41 × 106; 95% CI 0.76–7.71 × 1015; p = 0.216) (Table 2), while the trait FBS2/(FS2+FBS2) that measures bisecting N-acetylglucosamine (GlcNAc) in all fucosylated disialylated structures showed the largest likelihood of occurrence in RA cases (AOR 3.29 × 1085; 95% CI 0.09–2.55 × 10185; p = 0.093) (Table 2). Of the four major glycans comprising bisecting GlcNAc (GP6, GP10, GP19, and GP24) (Vučković et al., 2015) and of the three regular sialylated glycans (GP17, GP19, and GP24) (Vučković et al., 2015), GP24, which likewise shares features with both structures, showed significant occurrence in RA cases.
 , N-acetylglucosamine;
, N-acetylglucosamine;  , Mannose;
, Mannose;  , Galactose;
, Galactose;  , sialic acid;
, sialic acid;  , Fucose.
, Fucose.
95% CI, 95% confidence interval; AOR, adjusted odds ratio; GP, glycan; GP, glycan peak; RA, rheumatoid arthritis.
GlcNAc, N-acetylglucosamine.
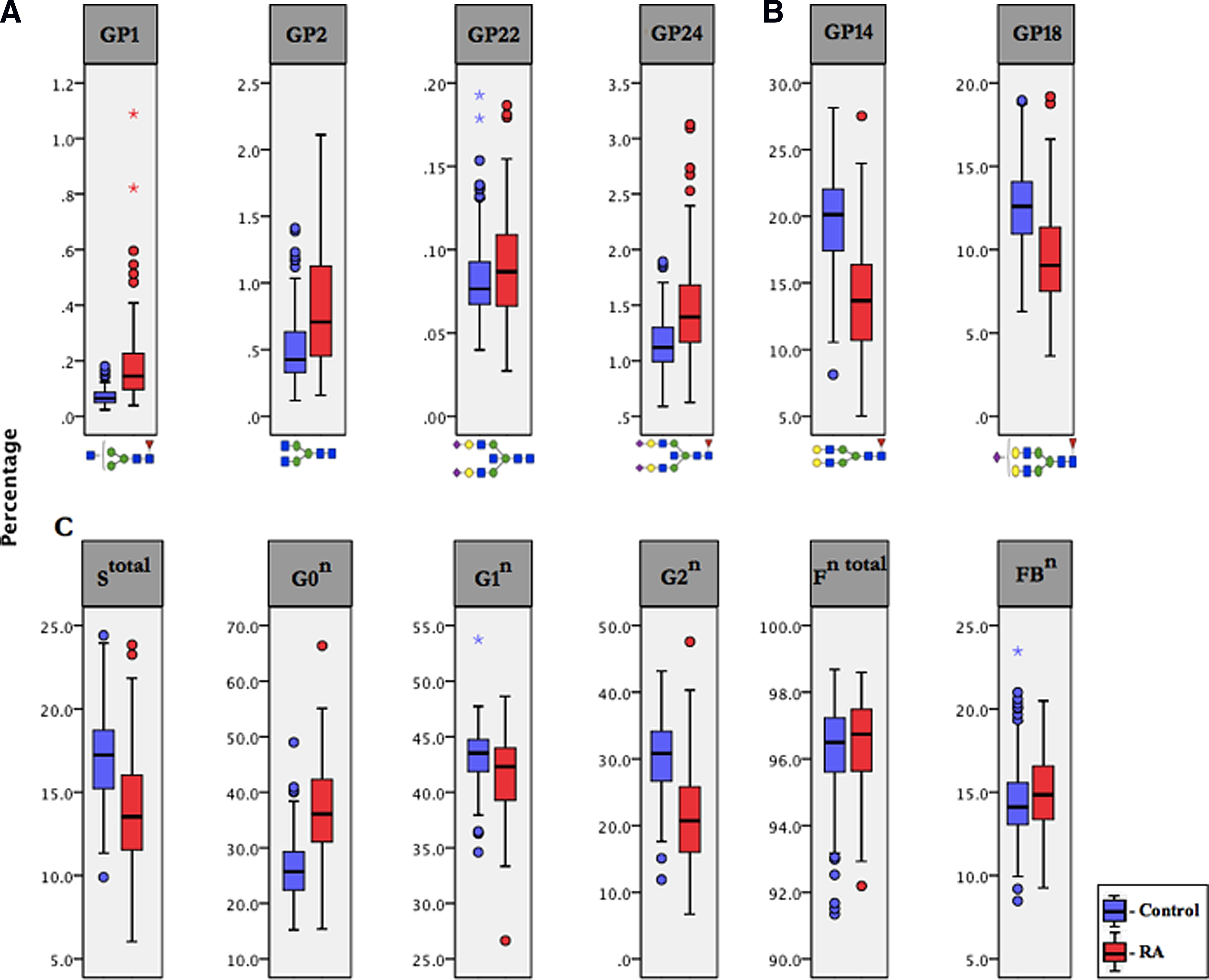
When the ROC curve analyses were performed on the four glycan structures that were found to be significant in the logistic model, we found that the area under the ROC curve (AUC) was 0.881, 0.717, 0.571, and 0.734 for GP1, GP2, GP22, and GP24, respectively. All the four GPs combined had an AUC of 0.928 (Fig. 1). From the box plot analysis, directly measured glycan structures in cases showed marked distinctions in the mean difference of GP1, GP2, GP22, and GP24 (Fig. 2A), whereas the mean of GP14 and GP18 demonstrated striking differences in IgG glycosylation in the control group (Fig. 2B). The mean difference of IgG glycosylation in the derived traits displayed a noticeable increase in Stotal (sialylation) and G2n (galactosylation) for controls and G0n (galactosylation) for RA (Fig. 2C).
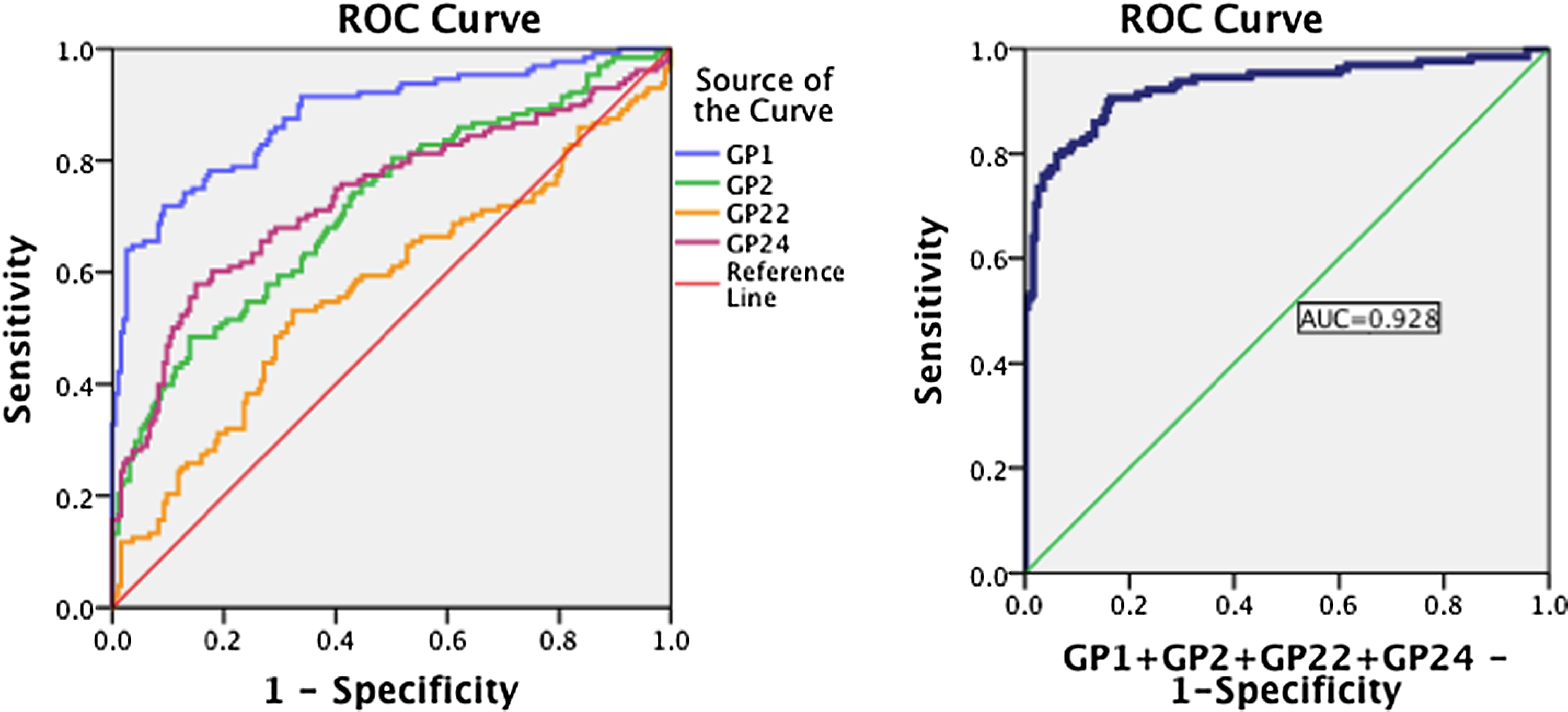
ROC curve analysis in regard to binary logistic regression in the prediction of disease in RA patients and controls. RA, rheumatoid arthritis; ROC, receiver operating characteristic.
Active and remission status
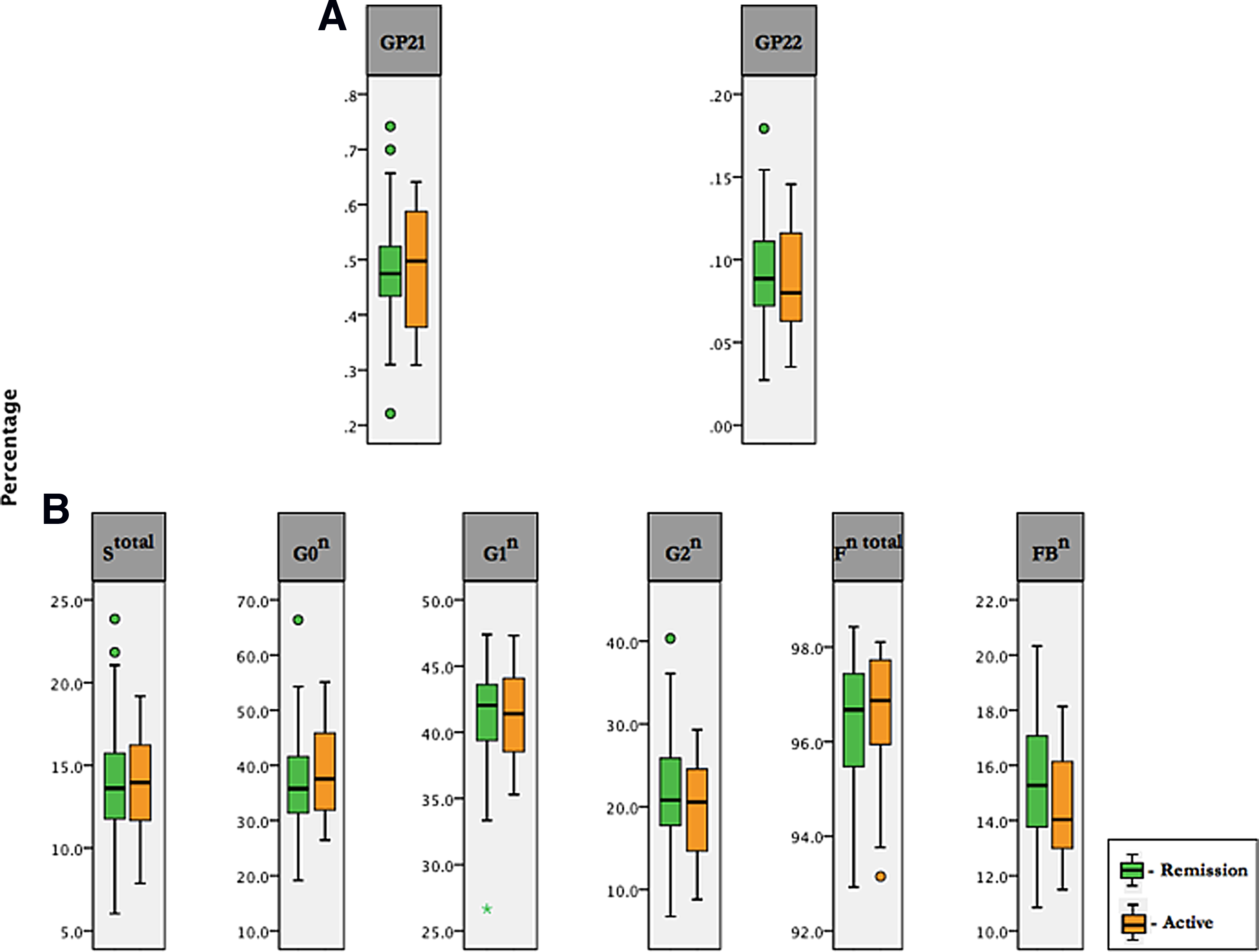
Two glycan structures (GP21 and GP22) were found to be statistically significant after the performance of logistic regression. The analysis indicated that GP21 (AOR 1.85 × 1010; 95% CI 82.53–4.16 × 1018; p = 0.016) had higher odds of occurrence in the active status than remission, whereas GP22 (AOR 0.03; 95% CI 0.01–0.05; p = 0.024) was less likely to occur in active status (Table 3). Of the four major glycans comprising bisecting GlcNAc, and of the three regular sialylated glycans, GP19, which shares similar features with both structures, indicated a likelihood of being present in active status rather than remission (AOR 87.73; 95% CI 0.30–2.59 × 104; p = 0.123) (Table 3). The combined ROC curve for GP21 and GP22 presented an AUC = 0.629 in the model; but the addition of gender into the model displayed an AUC of 0.658 (Fig. 3). The box plot analysis revealed that the directly measured glycan structure of GP21 showed an increased mean difference in the active status, while GP22 showed an increased mean in the remission status (Fig. 4A). There was a slight increase in the mean of Stotal, G0n, and Fn total in the active state and an increase in FBn in the remission state (Fig. 4B).
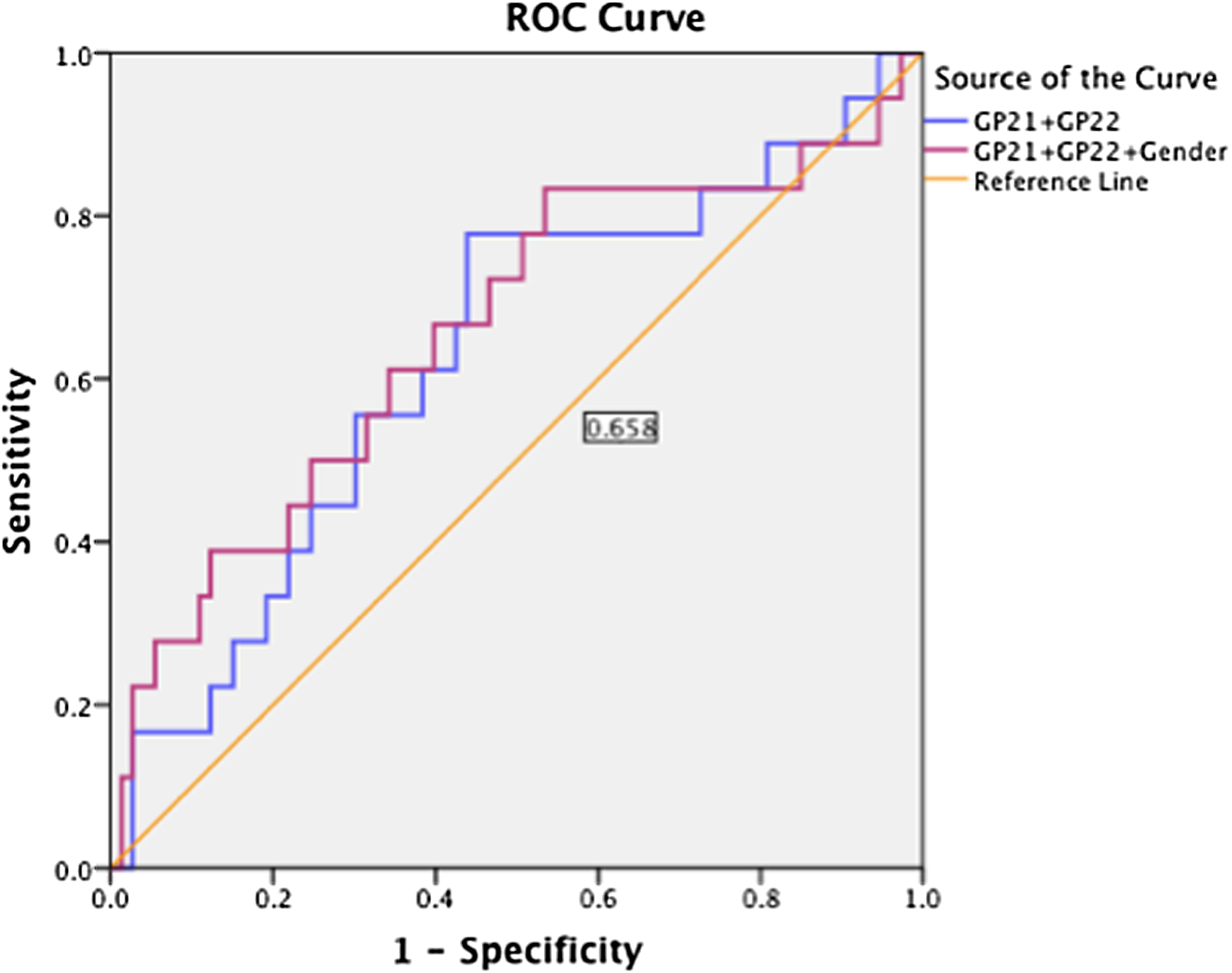
ROC curve analysis in regard to binary logistic regression in the prediction of active status in RA patients.
Discussion
In recent years, with the advancement of technology and the development of new therapeutic strategies, remission is the ultimate target of disease activity in RA (Aletaha et al., 2005; Forslind et al., 2007). Therefore, in an attempt to achieve a remission-like state as a potential therapeutic outcome in the future, we sought to discover potential glycan biomarkers in the active state of RA. To the best of our knowledge, this is the first attempt conducted on glycans with respect to active and remission statuses in RA. The study investigated the difference of altered states of N-linked glycans, their derived traits, and glycosylation patterns between cases and controls and between active and remission statuses while seeking to establish a glycan profile as potential biomarkers for both RA and active status in the Han Chinese population.
Our study shows that given the presence of the glycan structures GP1, GP2, and GP24, there is higher likelihood of occurrence of RA, but the presence of GP22 is less likely to result in occurrence of the disease. GP1 and GP2 are both agalactosylated glycans and share the derived trait G0n, which includes all glycans without galactose (GP1–GP6). Under steady-state conditions, 25–35% of serum IgG glycans are agalactosylated; however, this increases significantly in human autoimmune diseases such as RA, systemic lupus erythematosus, inflammatory bowel disease (Karsten et al., 2012), juvenile chronic arthritis, sarcoidosis, tuberculosis, active Crohn's disease, and Lyme disease, with RA being the most prominent in its increase of agalactosylated levels (Ercan et al., 2012). This is in agreement with our study, which showed an exponential increase of agalactosylated glycans in our RA cases.
Studies showed that there is a correlation between disease activity with decrease in the amount of galactose moieties, whereby the IgG glycans have both terminal galactoses (G0) missing (Gornik et al., 1999). Galactosylation of IgG had also been shown to play a role in anti-inflammatory activity (Lauc et al., 2014; Theodoratou et al., 2014). Autoantibody inflammation is suppressed when IgG antibodies convert from proinflammatory mediators to anti-inflammatory agents by the addition of galactose at the Fc glycan terminal (Abès and Teillau, 2010; Ercan et al., 2012; Shade and Anthony, 2013). When IgG is agalactosylated, the glycan is unable to bind to FcγRs and thus is not able for C1q to initiate antibody-dependent cell-mediated cytotoxicity (ADCC) and complement activation (Abès and Teillau, 2010). Hence, according to our results, it is probable that the exponential increase in agalactosylated glycans contributes to the pathogenesis of RA cases by inhibiting the initiation of ADCC and complement activities, while decreasing the immunosuppressive potential of IgG and resulting in a proinflammatory activity.
In addition, GP1 is an agalactosylated glycan with fucose moieties, while GP2 is an agalactosylated glycan lacking fucose moieties. When fucose is lost, steric hindrance is reduced and binding between afucosylated Fc and FcγRIIIA, natural killer (NK) cell-mediated ADCC, and antiviral activity measured by antibody-dependent cell-mediated virus inhibition assays is increased (Abès and Teillau, 2010; Shade and Anthony, 2013). When just one fucose residue is removed from the Fc portion of the glycan, IgG potency increases 50- to 100-fold in its initiation of ADCC (Shade and Anthony, 2013). Consecutively, studies conducted on mouse models in vivo suggest that potency of ADCC increases in the presence of afucosylated IgG (Pučić et al., 2011; Shade and Anthony, 2013). This would suggest that the addition of GP1 fucose moieties would contribute to the reduction of ADCC activity. As such, coinciding with our results, the combined exponential increase of GP1 as an agalactosylated fucosylated proinflammatory agent by 3.49 × 1016 times and its stark presence in an inflammatory environment in our RA cases strengthen our suggestion of GP1 as a potential diagnostic biomarker.
Both GP22 and GP24 are bisected digalactosylated, disialylated, biantennary N-linked glycans, while GP24 has fucose moieties, whereas GP22 lacks fucose moieties. In a bisected glycan structure, continued processing is suppressed as elongation of the N-glycan is terminated (Takahashi et al., 2009). Studies have shown that if bisecting GlcNAc is added to the core fucose, there is higher affinity of binding of IgG to FcγRIIIA since the presence of bisecting GlcNAc inhibits the addition of fucose preventing fucosylation (Lauc et al., 2013; Vučković et al., 2015) and increasing ADCC activity by up to 10–20 times (Takahashi et al., 2009). Fucosylation of glycans determines the degree at which ADCC is regulated (Shade and Anthony, 2013). Uncontrolled regulation of ADCC leads to increased ADCC resulting in autoimmunity, whereas inefficient ADCC results in cancer (Lauc et al., 2014).
Several studies showed that when a fucose residue is added to the glycan core (core fucose) of the N-acetylglucosamine, the Fc region is so altered that it is unable to bind to FcγRIIIA—a CD16 receptor expressed on NK cells that activate the Fc region-terminating initiation of ADCC (Lauc et al., 2014; Lauc, 2012). When core fucose is lost, IgG glycans increase clinical efficacy of monoclonal antibodies and ADCC activity is enhanced 100 times over (Lauc et al., 2013, 2014; Pučić et al., 2011). The increase of GP24 as a major bisecting GlcNAc by 521 times in our RA cases implies that the inhibition of fucose has occurred, which results in low levels of fucose and therefore enhances ADCC activity. Conversely, GP24 adds fucose moieties and reduces the activity of ADCC. This by extension leads to the uncontrolled regulation of ADCC, suggesting the contribution to the resultant inflammatory activity.
However, GP24 is also a regular sialylated glycan, which means increase in sialylation activity has occurred as well. Several studies have shown that sialylation of the IgG glycan Fc portion leads to the conversion of proinflammatory molecule to an anti-inflammatory agent (Ercan et al., 2012; Kaneko et al., 2006; Lauc et al., 2014; Lauc, 2012; Novokmet et al., 2014; Pučić et al., 2011) and that the addition of terminal α2,6-sialic acid residues greatly reduces the presence of ADCC both in vitro and in vivo (Kaneko et al., 2006; Shade and Anthony, 2013). In contrast, we found an increase of GP24 in the presence of proinflammatory activity. A possible explanation might be that the presence of bisecting GlcNAc and its increased levels in RA might have overlapped and superimposed the actual impact of the sialylation that had occurred, allowing for uncontrolled regulation of ADCC instigating inflammation.
The odds of disease occurrence in the presence of GP22 are low. In a study on parasites, there have been suggestions that the property of GP22 is capable of inducing a cross-reactive immune response with other antigens, which protects the host from reinfection (Petzke et al., 2000). The authors suggested that GP22 in humans shares similar characteristics of protective ability with the rat IgG2a, which is associated with resistance to infection through complement activation or ADCC, and hence also expresses protective capacity (Petzke et al., 2000). As such, absence of fucose moieties on GP22 suggests enhanced activity and potency of ADCC. Coupled with the implication above, this could explain why the occurrence of GP22 in the presence of inflammatory activity is least likely to transpire in our RA cases.
Taking into account all four significant glycan structures from our regression model, the ROC curve analysis was performed to account for the sensitivity of the glycan structures and their diagnostic power of prediction as a potential biomarker. Comparatively, our study found GP1 to be sensitive in predicting our RA cases. Thus, the presence of GP1 in the inflammatory environment of our RA cases coupled with the diagnostic power of prediction at a precision of 88.1% suggests that GP1, which has a higher accuracy of association with RA occurrence, could be considered as a potential diagnostic biomarker for RA cases of Han Chinese ancestry.
In the active state, exposure of the glycan structure GP21 indicates that occurrence of disease activity had a higher likelihood of outcome, whereas GP22 is less likely to cause disease activity. GP21 is found on the surface of antigens where it not only facilitates envelope trafficking and membrane targeting (Mota-Miranda et al., 2014) but also acts as a protective antibody neutralizing agent (Sundaram et al., 2004) that contributes to immunosuppression by apoptosis (Ruegg et al., 1989). Herman et al. (2009) reported that the immunosuppressive effect of methotrexate (MTX) on CD4+ (a glycoprotein on the surface of T-helper cells) is found in active RA patients, whereas immunostimulation by MTX is exhibited in remission patients in vitro. If we then consider that the properties of GP21 imitate that of MTX, an immunosuppressive drug for RA, consequently an increase in GP21 would lead to uncontrolled inflammation and disease activity in an RA patient. However, GP21 is not a suitable predictor of active status in RA patients due to its lower sensitivity value in the ROC curve analysis. This lower sensitivity could be explained by patients in remission phase who are associated with the progressive reduction of the inflammatory process (Lin and Li, 2010).
Our findings should be interpreted considering several limitations. First, case–control analysis does show association, but does not allow us to determine cause–effect relationship of IgG glycosylation and RA disease status. Second, the relatively small sample size could not allow us to draw robust conclusions on GP1 as a potential diagnostic biomarker as well as the effects of IgG glycosylation on the active and remission statuses. Therefore, a larger sample size would warrant the validation of our results along with the comparison of glycosylation patterns between active and remission statuses of the disease in RA patients. Finally, as this study represents and is concentrated on Han Chinese ethnicity, case–control or cohort studies with different ethnic participants are recommended for comparison and corroboration purposes.
Conclusions
Taken together, these observations suggested that GP1 might have potential as a putative biomarker for RA in the Han Chinese population, while the change in IgG glycosylation shows association with the RA active and remission states. To the best of our knowledge, this is the first glycomics study with respect to disease activity and remission states in RA.
Footnotes
Acknowledgments
This work was supported by grants from the Australian National Health and Medical Research Council and National Natural Science Foundation of China (NHMRC-APP1112767-NSFC 81561128020), National Natural Science Foundation of China (NSFC-81370083, 81273170, 81573215), Australia–China International Collaborative Grant (NH&MRC-APP1112767-NSFC 81561128020), the National Key Technology Support Program, China (2012BAI37B03), and EU-fp-7 Pain-Omics (602736). A.S., M.A.A., C.O.A., X.Y, and S.G are supported by the China Scholarship Council (CSC-2015); M.S. is supported by the Importation and Development of High-Calibre Talents Project of the Beijing Municipal Institutions (ICIT&TCD201404185); and Y.W. is supported by the Beijing Higher Education Young Elite Teacher Project (YETP1671) and the Beijing Nova Program (Z141107001814058).
Author Disclosure Statement
The authors declare that no competing financial interests exist.