
Abstract
Abstract
In modern healthcare systems, the available resources may influence the morbidity, mortality, and—consequently—the level of healthcare provided in every country. This is of particular interest in developing countries where the resources are limited and must be spent wisely to address social justice and the right for equal access in healthcare services by all the citizens in economically viable terms. In this light, the current allocation is, in practice, inefficient and rests mostly on each country's individual political and historical context and, thus, does not always incorporate decision-making enabled by economic models. In this study, we present a new economic model, specifically for resource allocation for genomic medicine, based on performance ratio, with potential applications in diverse healthcare sectors, which are particularly appealing for developing countries and low-resource environments. The model proposes a new method for resource allocation taking into account (1) the size of innovation of a new technology, (2) the relative effectiveness in comparison with social preferences, and (3) the cost of the technology, which permits the measurement of effectiveness to be determined differently in the context of a specific disease and then to be expressed in a relative form using a common performance ratio. The present work expands on previous work for innovation in economic models pertaining to genomic medicine and supports translational science.
Introduction
G
Economic evaluation aims to assess whether a new healthcare technology or intervention provides “value for money” in terms of costs and therapeutic consequences compared to existing interventions (Fragoulakis et al., 2016). The most common research approach used by policy makers to assess the value of innovative technologies and/or interventions is the determination of the incremental cost effectiveness ratio (ICER) (O'Brien and Briggs, 2002), defined as the ratio of the average per-patient incremental cost (ΔC) of one intervention divided by an incremental health gain (ΔE), determined, according to the medical specialty, for instance, an additional stroke prevented, a case of cancer diagnosed, or gain of a life year (LY) or, primarily, an additional quality adjusted life year (QALY).
In other words, ICER represents the difference in costs between a new intervention under consideration for adoption and the current approach to dealing with the same clinical problem/client group (the incremental cost) divided by the difference in outcomes between the new intervention and the current approach (the incremental effects). If ICER is below a predetermined amount, a policy maker is willing to pay for an additional unit of effectiveness (the desirable medical outcomes), the new intervention called a “cost-effective option,” and meets one of the criteria for reimbursement by the payers. In the latter case and despite its shortcomings, QALY represents one of the widely accepted measures used to consider the ability of an intervention to extend life and to improve the quality of life for the patients.
Until recently, the decision-making process was supported by the classical concept of cost-effectiveness analysis (Fragoulakis et al., 2015). In accordance with this theory, cost-effectiveness analysis represents a tool which has been used to maximize health gains from the use of available resources, and this appears to reflect the needs of the decision makers. However, this type of analysis has been criticized and has some distinct drawbacks in practical terms. A key concern is that this threshold approach might lead to controversial or contested decisions and increase further the expenditures in a healthcare system as mentioned by Gafni and Birch (2006). Indeed, the classical theory assumes that all “cost-effective” interventions with increased effectiveness compared with the standard (conventional) intervention could or should be reimbursed by the payers.
In that sense, the classical approach assumes silently an arbitrary adjustment of budget in the cost of new technologies and, thus, unlimited budget availability. Hence, the above approach of cost-effectiveness does not incorporate the ability of a healthcare system to reimburse a new health technology and, thus, in practice requires an additional, and different, type of analysis to determine the economic burden of short- and medium-term effects on budgets and other resources to reach a final conclusion. This type of analysis is called “budget impact analysis” (Goettsch and Enzing, 2014), but its criteria for the final verdict concerning the adoption or rejection of a new health technology remain unclear.
In addition, there are other drawbacks in this analysis. First of all, to adopt a new intervention the decision maker must withdraw some existing interventions to find enough resources to support the new ones. However, in practice, very few, if any, economic evaluations state explicitly which specific health technologies and/or interventions must be withdrawn to meet the budget criteria (Birch and Gafni, 2006). In addition, the classical theory assumes that all decrementally cost-effective options (less costly, less effective but within the willingness-to-pay threshold) (Nelson et al., 2009) could be reimbursed based on cost criteria.
However, it is obvious that there are important moral and ethical issues in the treatment of patients which make the possibility to adopt an alternative “very poor,” in terms of effectiveness, technology and/or intervention highly unlikely, despite their cost-saving profile. Furthermore, the classical model assumes that the willingness to pay for a unit of effectiveness is independent of the actual difference in effectiveness between different health technologies and, thus, does not differentiate among a new truly innovative health technology, a similar-with-the-current health technology, or even a generic health technology and reimburse proportionally equally each one of them based on an arbitrary willingness to pay (Bridges et al., 2010; Cleemput et al., 2011). To deal with these drawbacks, a modification of the present theory has to be conducted.
In this article, we present a new economic model, specifically designed for resource allocation in genomic medicine, based on performance ratio, with potential applications in genomic medicine and also in other healthcare sectors.
Methods
Where we stand: the Genome Economics Model
Based on the above consideration, we have recently proposed a new model to resolve these aforementioned drawbacks (Fragoulakis et al., 2016). Genome Economics Model (GEM) implies that there is a maximum amount of money per patient that could be spent by the payers only if a certain therapeutic gain from an innovative health technology was met by health providers. As such, in sharp contrast with the classical cost-effectiveness approach, under the GEM approach, the insurance funds define ex-ante what is expected to be the upper limit of “‘innovation” in terms of effectiveness/QALY gains, what is the lowest acceptable effectiveness that could be accepted, and judge ex-post every new technology within two boundaries.
In addition, GEM defines the maximum amount of money willing to be invested or save the budget holder within two boundaries. Furthermore, the GEM, contrary to the classical model, does not conduct a separate budget impact analysis, as—by definition—every cost-effective technology in the GEM meets also the cost criteria. GEM was developed to be sensitive of the actual incremental effectiveness of a new intervention, in correlation with the willingness to pay for a QALY in a formal manner [for mathematical details see Yin et al. (2003)]. In this context, every potentially new unit of effectiveness that could be gained from future technologies has a different perceived value by policy makers. For a very small difference between two health technologies, the average willingness to pay for a QALY is expected to be low due to low additional value. For more innovative interventions with some fair differences in terms of effectiveness, a higher average willingness to pay for a QALY (but also smaller than those offered by the classical model) can be expected (Kvamme et al., 2010).
For innovative interventions with significant difference in terms of effectiveness, the average willingness to pay for every unit of QALY is expected to be higher in comparison with classical model. As the difference in effectiveness increases further (breakthrough technology), we meet the budget constraints criteria and, as such, we are unable to reimburse this technology further and the average willingness to pay is getting lowered. The shape of willingness to pay for a QALY resembles, as the potential difference in effectiveness increases, a bell-shape distribution, contrary to the classical model, in which willingness to pay is a straight line, determined by arbitrary assumptions, made by policy makers or the literature (Fragoulakis et al., 2016).
Despite these appealing aspects, GEM does not address the very important issue of health resource allocation problem. Indeed, in this model a far less ambiguous approach was adopted to estimate the local equilibrium which is driven by the de facto budget availability in a disease-specific context without taking into account QALYs from different therapeutic areas. Hence, all conclusions and contributions of the GEM were referred to a specific disease context without any comparisons with other therapeutic areas. To deal with such challenges, the identification of effectiveness, and consequently, the amount of willingness to pay, could be attained/determined by ranking the available interventions for all diseases under a resource constraint with the use of a mathematical programming-type technique (Sendi et al., 2002).
Rationale and description of the model
The aim of the present model is to propose an alternative method for resource allocation taking into account (1) the incremental innovation of a new technology, (2) the relative effectiveness in comparison with social preferences, and (3) the cost of the technology, while permitting the measurement of effectiveness to be determined differently in the context of a specific disease and then to be expressed in a relative form through a common performance ratio.
Contrary to GEM, the present new model aims to provide a practical solution for resource allocation in entire healthcare sector and to go a step further in the decision-making process. In practice, the scope of the present model was to determine an alternative and most precise way to share the available resources, maximizing a specific utility function in the same spirit as GEM. The model in the present form simplifies the complexities of real life and, thus, does not take into account the uncertainty of variables (Briggs et al., 1994) and, consequently, determines its results in a deterministic way. In addition to that, the model is particularly applicable to developing countries, as it assumes that the introduction of new innovative technologies improves the current medical practice, and thus, it is connected with fewer adverse events and greater effectiveness compared with the technologies which are currently in use. Hence, the case of decrementally cost-effective choices is not taken into account in this form. Below we describe the main steps for the construction of the new model.
Methodological approach
The model is developed in a six-step approach (Fig. 1). First of all, the decision makers must identify all the available health technologies (comparators) within different disease-specific areas. These choices must include the “most expensive,” the “least costly,” and the “gold standard” intervention, which must be set in accordance with the standard medical practice, the literature, and the current scientific research (Drummond et al., 1997). It must be noted that specific attention has to be given to this step, since some healthcare technologies are frequently presented as a “cost-effective choice” assuming that all available knowledge has been incorporated in the evaluations, while in practice this term refers only to some of the available options, which dominate the market share.
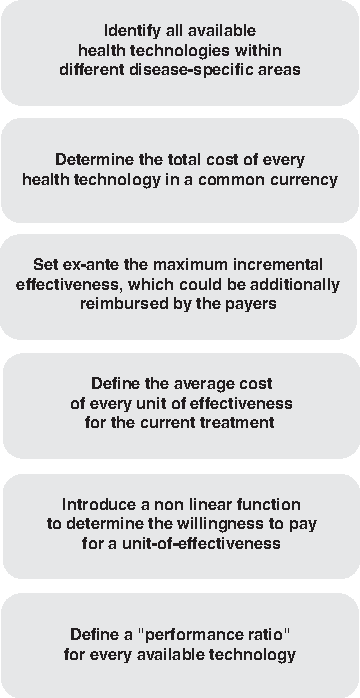
A step-wise approach for the proposed model for resource allocation and decision-making in genomic medicine.
Second, the total cost of every health technology must be determined in a common currency (e.g., € or $). Cost determination must be in accordance to the current standards used in sound economic evaluations (Husereau et al., 2013). Subsequently, the decision maker has to define how effectiveness in its separate disease-specific context needs to be determined. For instance, in GEM, there is no mandatory rule to express the effectiveness through the common measure of QALY, to avoid problems which are connected with this instrument (Schwappach, 2002). Thus, several different disease-specific (but one-dimensioned) formulae must be used in each area.
For instance, in oncology, it might be possible to use the “Progression Free Survival,” as it defines the period over which the patient is free from disease progression, but must be used carefully in economic evaluation, since the correlation of this tool with the prolongation of life or improved quality of life is not always clear (Sullivan et al., 2011). Similarly, other specific tools have to be used for the other therapeutic areas. When all the available health technologies are expressed (as “Cost” [€, £, $], “Effectiveness” [PFS], etc.), then the second step of the model is completed.
The third step in the alternative model, proposed herein, is to set ex-ante what could be considered in the near future as the maximum incremental effectiveness (denoted as “ΔEmax”), which could be additionally reimbursed by the payers. This effectiveness expresses the most ambitious scenario in terms of effectiveness gains, which the policy makers are willing to additionally reimburse and must be set in every therapeutic area by the corresponding scientific and medical societies. This “ΔEmax” has to be expressed, as mentioned, in the terms of this particular tool used in every area.
It must be noted that in a developing country with few available resources, the amount of ΔEmax is expected to be relatively low, since the marginal utility of the limited resources is high. It must also be noted that the determination of ΔEmax might be a multicriteria process, which has to take into account how a new technology has better effectiveness, how it affects patient quality of life, and if it is easier to administer or safer to use and with fewer side effects. In addition to that, its therapeutic properties and mechanism of action must be taken into account, if (1) it constitutes a sound alternative enabling greater precision to individual patient needs, (2) and to which extent improves patient compliance through better dosage and administration mode, and (3) it extends the indications and gives multiple options in the same therapeutic class and/or reduces or substitutes other forms of therapy (www.who.int/medical_devices/innovation/en; accessed on October 9, 2016).
The fourth step is to define the average cost of every unit of effectiveness for the current treatment and this cost to be projected through a linear function form to meet the maximum incremental effectiveness. This step follows a similar concept of the “proportional rule” used by the German Organization of Health technology assessment (IQWIG) (Lubbe, 2010), based on which every new health technology must provide at least a proportionally equal increase in percentage of effectiveness for an x% increase in the total cost of a technology.
In other words, an increase in cost at x% must be followed (at least) with an x% increase also in effectiveness. It must be stressed that the average cost per unit of effectiveness in each specific disease area will be different, which is logical, as the effectiveness in each area follows a different pattern concerning the cost and the effectiveness. For instance, it is much more difficult to produce a life month gain for an oncology patient than a cardiology patient, and this feature is taken into account with our new model. This concept of a hypothetical example with two diseases is depicted in Figure 2.
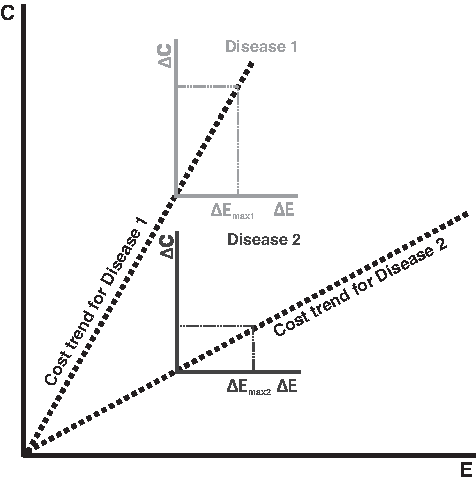
Average cost and linear trend in a disease-specific context. For every different disease (“disease 1,” “disease 2,” etc.), we estimate the average trend for cost (based on the available historical data) and then we project it in the short term, to meet maximum additional effectiveness we are willing to reimburse in a finite future (ΔEmax).
The fifth step, borrowed from the previous model described in Fragoulakis et al. (2016), is to introduce a nonlinear function, which determines the willingness to pay for a unit of effectiveness in correlation with the actual difference produced by every new health technology. This nonlinear function for willingness to pay drives healthcare providers to increase the effort for favorable treatments, “punishes” the less productive ones, and “rewards” those technologies which provide significant incremental innovation with viable economic terms (Fig. 3).
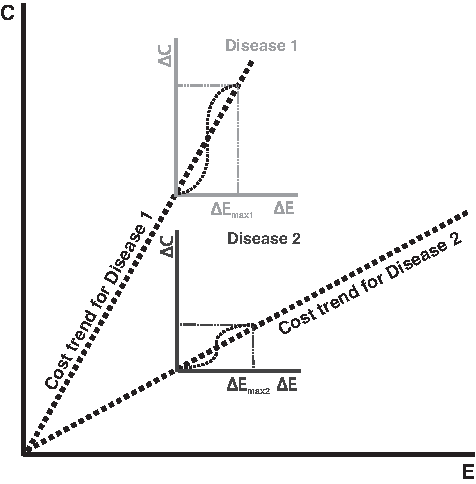
Willingness to pay for a unit of effectiveness in a disease-specific context. Further to Figure 2, for each disease, we introduce also a nonlinear curve, which determines the willingness to pay for an additional unit of effectiveness based on the projected cost and the ΔEmax.
Finally, the proposed new model defines a “performance ratio” for every available technology, which is determined by the “one minus the ratio of the actual incremental cost of a new technology divided by the willingness to pay for the actual effectiveness gained” by this specific technology. If this ratio is negative, the policy makers are not willing to adopt and rejects this technology, since the cost of adoption is greater than what they are willing to invest. Of course, the most prominent options will be those technologies that will have the higher performance ratio (near to one), as they have the biggest surplus. This concept on how to determine the results of each technology is depicted in Figure 4.

Definition of performance ratio, which determines the relative performance of a healthcare technology based on a relative basis. For instance, a 20% performance indicates that the cost of a technology is only 80% (100%–20%) of the total cost that the Insurance Funds are willing to invest to gain the specific effectiveness this technology offers. When performance ratio equals 100%, this indicates that the new technology is offered in the same cost with the standard technology and, thus, represents a dominant choice. A negative performance ratio indicates technologies which have to be rejected by the healthcare system.
Finally, as a rule, the available resources will be spent for those technologies which provide the most attractive performance across the healthcare sector with a mathematical programming type of analysis until the budget is exhausted (Flessa, 2000). This model assumes that the policy makers are willing to maximize this performance ratio of health gains and not to maximize QALYs as it is normal (Weinstein et al., 2009).
Hence in this model, the aspect of innovation has two different and distinct dimensions as follows: (1) the actual difference in effectiveness which is on behalf of the patient in correlation with what is expected to be the true innovative health technology and (2) the containment of cost expenditures, which plays an important role for all modern healthcare systems. With this model, all health technologies (“me-too,” “fair,” “innovative,” “very innovative,” and “breakthrough”) in all specific areas become comparable through the “performance ratio,” and thus, the model provides a ground for comparisons (and reimbursement) among them. Of course, to meet meaningful conclusions, the model requires the explicit mapping of preferences through the nonlinear forms of willingness to pay in a quantitative form.
It must be noted that in accordance with the maximization rule of the performance ratio, the model gives a “premium” in innovative technologies and permits them to absorb proportionally higher amount of budget in comparison with a simple linear approach of classical model. In other words, for innovative interventions (in terms of effectiveness), there is a higher reimbursement as a reward for the successful research and development process, while the model is more strict in “me-too” technologies, since it expects only a marginal additional cost burden from them.
Results and Discussion
Understanding the relative benefits and drawbacks of alternative strategies for resource allocation is important to ensure that patients receive not only effective but also economically efficient care and that healthcare systems have the chance to stay sustainable in the future (Sendi and Briggs, 2001). It is well known that every developing country is crucial to establish a well functioning healthcare system, to invest the necessary funds, and to follow the major planning priorities for each country (Okebukola and Brieger, 2016).
In this study, we have proposed an alternative methodological concept for resource allocation, which represents the generalization of a previously published work (Fragoulakis et al., 2016), which can be particularly useful not only for developed but also more importantly for developing countries. In particular, the healthcare budget is more restricted in developing countries, which make economic evaluation more vital. The economic model described herein allows for greater flexibility in determining the quality of life, as it offers a different means of representing the performance of a health technology through the performance ratio as a measuring scale and not QALYs. Moreover, in developing countries, it is often more difficult to find specific evidence for measuring effectiveness, for example, EQ5D questionnaires measuring quality of life, which are necessary for QALY-based economic evaluation.
In the present work, it has been argued that “innovation” must be set as a priority and this term might also include the following: (1) the absolute benefit on behalf of the patients and (2) the ratio of cost and effectiveness in terms of “social consumer surplus.” To avoid theoretical issues with the use of QALY, which is still under consideration (Baker et al., 2010; Lancsar et al., 2011; Wailoo et al., 2009), the present model uses a new index called “performance ratio,” which determines the proportional increase in effectiveness (the relative effectiveness as percentage) in accordance with social preferences. In this light, we have avoided the use of QALYs, despite the fact that it is possible to be also used as the variable which can be maximized. In that sense, the model maximizes a unified theoretical and abstractive index, which takes into account three different “variables” namely the cost, the effectiveness and its size, and the social preferences.
It must be noted that many countries, both developed and developing, face two distinct and important issues, which represent highly important political decisions. On one hand, in the view of the scarcity of resources, many countries face hard budget constraints and, thus, attempt continuously to implement austerity measures for healthcare services. On the other hand, the technology evolution might potentially provide policy makers with a plethora of many alternative healthcare technologies, which have to be assessed economically and from a medical standpoint and then to be adopted and reimbursed in each country.
In this light, the scope of the economic models, in general, and in genomic medicine, in particular, is to (1) provide systematic evaluation of the total cost, (2) determine the outcome (benefit) in comparison with the cost measured for all alternative choices, (3) determine the incremental cost in comparison with the incremental outcome for standard and innovative technologies, and (4) to determine the economic implications in terms of financial affordability for each healthcare system. Given that the applications of genomic medicine might provide a fair therapeutic gain in several areas, it is also of primary interest to (1) assess the exact therapeutic gain of these genomic technologies in general, (2) determine the potential benefit for different group of patients and of different ethnicities, where applicable, etc., (3) thoroughly assess all the available techniques, interventions, etc. and how they can be translated in meaningful practices, and (4) predict the potential future benefits from the technologies which are still under consideration.
In addition to that, since the nature of the information which can be provided by whole genome sequencing for a patient/individual's future health decisions is substantial, it is also of primary interest to develop new economic models to address this area as well, which might be the scope of future research, particularly since traditional economic models investigate the value for money in a static manner. As a general comment, it is also not only worth mentioning that budget availability determines, to some extent, the social reward of innovation but also is worth considering how the investors may restrict their scientific research only to those areas which could potentially offer a significant return on investment in financial terms. Given that genomic medicine is a relatively new domain, it is crucial to remain “free” of this kind of “profitable opportunities” and must be judged precisely and objectively on behalf of the patients and the society as a whole.
Every model is by necessity a simplification of the process which tries to investigate, and this model is not an exception. First of all, from a technical viewpoint, the present analysis pays particular attention only to deterministic results assuming that the cost and effectiveness are point estimates. In practice, due to limited knowledge, all these variables represent distributions and even the budget is not necessarily strictly defined in each country. Hence, to solve the problem in a probabilistic way, a much more complex mathematical procedure must be implemented.
It must be noted that the potential value of the present model must be judged in comparison with similar attempts previously made (Eckermann et al., 2008) (see also www.york.ac.uk/che/pdf/mathprog.pdf). In most of the cases, the analysis of this “maximization problem” has two more distinct drawbacks. First of all, it is highly technical and uses advanced mathematical techniques to deal with all issues involved in this type of analysis under several different assumptions. Frequently, these different assumptions might alter the conclusion of an analysis and must be judged carefully. In addition to that, the model implies a complex process in which formulae need to be created for every disease and effectiveness needs to be evaluated over a long time period, meaning that it is not always easy to implement. This sort of evaluation would be costly and, therefore, might limit the usefulness of the present model.
Also, an additional restriction of our model is that it takes into account and incorporates all ethical and political issues in a subjective manner. Nonetheless, as previously mentioned, economic evaluation represents a useful tool, but despite the attractive veneer of objectivity given by the concise and elegant mathematical nomenclature, the actual subject of financial resource management is in practice a fundamentally political problem (Fragoulakis et al., 2015).
In essence, this alternative model provides a further insight in the decision-making process in genomic medicine and an improved management tool for the policy makers, particularly for developing and resource-limited countries, which warrant practical implementation. In summary, the main methodological differences among our previously proposed model (GEM) and the new one presented herein are described in Table 1. Despite the fact that this model is primarily meant for genomic medicine, it might also be used in other healthcare sectors, and the exploration of this model in practical applications could be the scope of future research.
Although not necessary.
It is general model.
GEM, Genome Economics Model; QALY, quality adjusted life year.
Footnotes
Acknowledgments
This work was partly funded by a European grant (UPGx; H2020-668353) and the Golden Helix Foundation and endorsed by the Genomic Medicine Alliance Economic Evaluation in Genomic Medicine Working Group.
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.