
Abstract
Abstract
Telomere length (TL) is an important biological variable that can influence a variety of disease-related complex traits as well as host–environment interactions such as drug and nutritional responses. Chronic kidney disease (CKD) is a common global health challenge especially with the currently aging world population. We conducted a PubMed database search according to the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines for systematic reviews. Studies in adults (18 years and above) in which TL was determined and correlated with CKD, renal traits, and function were included, while animal model studies were excluded. Nine studies comprising 7829 participants, published between 2005 and 2016, met the inclusion criteria. These included eight observational studies (six being prospective), and one clinical trial. Participants in two studies were diabetic patients with varying stages of CKD, and nondialysis chronic glomerulonephritis CKD patients in two other studies. TL measurements used polymerase chain reaction in five studies, terminal restriction fragmentation in three studies, and quantitative fluorescence in situ hybridization in one study. Short TL was independently associated with increased risk of prevalent microalbuminuria in diabetic men with CKD (p = 0.007). Among CKD patients with heterogeneous etiologies, however, there was an unadjusted lower risk (p < 0.001). Short TL was significantly associated with CKD progression among smokers (p = 0.001) and diabetic patients (p = 0.03). On the other hand, long TL was paradoxically associated with longer diagnosed duration of moderate CKD. We postulate that shortening TL might be associated with CKD prevalence/occurrence or declining kidney function, but this association is likely offset by the cellular telomere reparative process in those surviving longer with CKD. This systematic review underscores the need for future omics and human genetics research to delineate the contribution of TL to CKD, renal dysfunction, and related health outcomes. Telomeres and telomerase activity hold great promise for CKD risk stratification and personalized medicine.
Introduction
C
Telomeres are chromosomal protective caps consisting of aggregates of TTAGGG repeats that serve to prevent the loss of deoxyribonucleic acid (DNA) during cell division (Verdun and Karlseder, 2007). In healthy human populations, the length of telomeres is heterogeneous, ranging between 5 and 15 Kb (Samassekou et al., 2010). Telomere length (TL) shortens with each replicative cell cycle until a critical TL is reached when further cellular replication ceases and the cell enters into senescence, a process known as replicative senescence. Cells can, however, also be forced into premature senescence under stressful conditions such as oxidative stress (stress-induced premature senescence) (Chen and Ames, 1994; Kaneko et al., 2001). Senescent cells, although viable, undergo phenotypic and functional changes, which ultimately influence the function of organ systems (Tsirpanlis, 2008). Telomeres therefore play a pivotal role in determining cellular biologic age and continued function. Laboratory and clinical data have emerged, demonstrating the association between cellular senescence (TL shortening) and several cardiovascular risk factors such as insulin resistance, cigarette smoking, impaired glucose tolerance, diabetes mellitus, and hypertension (Adaikalakoteswari et al., 2007; Demissie et al., 2006; Gardner et al., 2005; Sampson et al., 2006; Valdes et al., 2005).
Among hemodialysis patients, accelerated telomere attrition as well as reduced telomerase activity have also been demonstrated (Ramirez et al., 2005; Tsirpanlis et al., 2006). However, in the hemodialysis population, exposure to the dialyzer membrane as well as other aspects of this extracorporeal technique contributes an added inflammatory response beyond the inflammatory milieu associated with nondialytic CKD and may thus promote telomere attrition (Jofre et al., 2006). There is a gap in the literature on systematically synthetized evidence on associations between telomere attrition or telomerase activity and the nondialytic stages of CKD. An understanding of the role(s) of telomere attrition in the occurrence and progression of CKD can provide insights for development of new prevention and intervention strategies in CKD management. We report here a systematic review of the literature in adult CKD patients to assess the association between TL and CKD or markers of kidney dysfunction.
Materials and Methods
Database search strategy
This systematic review was conducted using the preferred reporting items for systematic reviews and meta-analyses (PRISMA) framework (Supplementary Table S1). We searched the PubMed-MEDLINE database for eligible studies using a combination of search terms and key words (Supplementary Table S2). Searches were restricted to studies on adult subjects (age ≥18 years), published in English or in French language, and without limitation to the date of publication. In addition, we searched the reference list of selected articles for citations meeting the systematic review's criteria. Opinion leaders and experts in the field of genetics and telomere medicine were also consulted for possible known, but unindexed, publications relevant to the systematic review.
Selection of studies
Two reviewers (O.I.A. and I.G.O.) independently conducted the database searches, screened titles, and abstracts of potentially relevant studies, as well as conducted detailed full-text reviews of selected publications. Instances in which an agreement could not be met on a study's inclusion or exclusion, a third reviewer (A.P.K.) independently assessed eligibility. Included studies were original published studies conducted among adult human subjects, regardless of gender or language of publication. We included cross-sectional and prospective studies among adults in whom TL was determined and correlated with the presence of CKD, or renal traits. Studies in animal models of CKD, narrative reviews, letters, opinions, and commentary articles, were excluded. The process of study selection is depicted in Figure 1. The Cochrane Bias Methods Group assessment tool was used to evaluate the risk of bias in the selected randomized clinical trial, while the Newcastle–Ottawa Scale was utilized for the selected observational studies (Table 1).
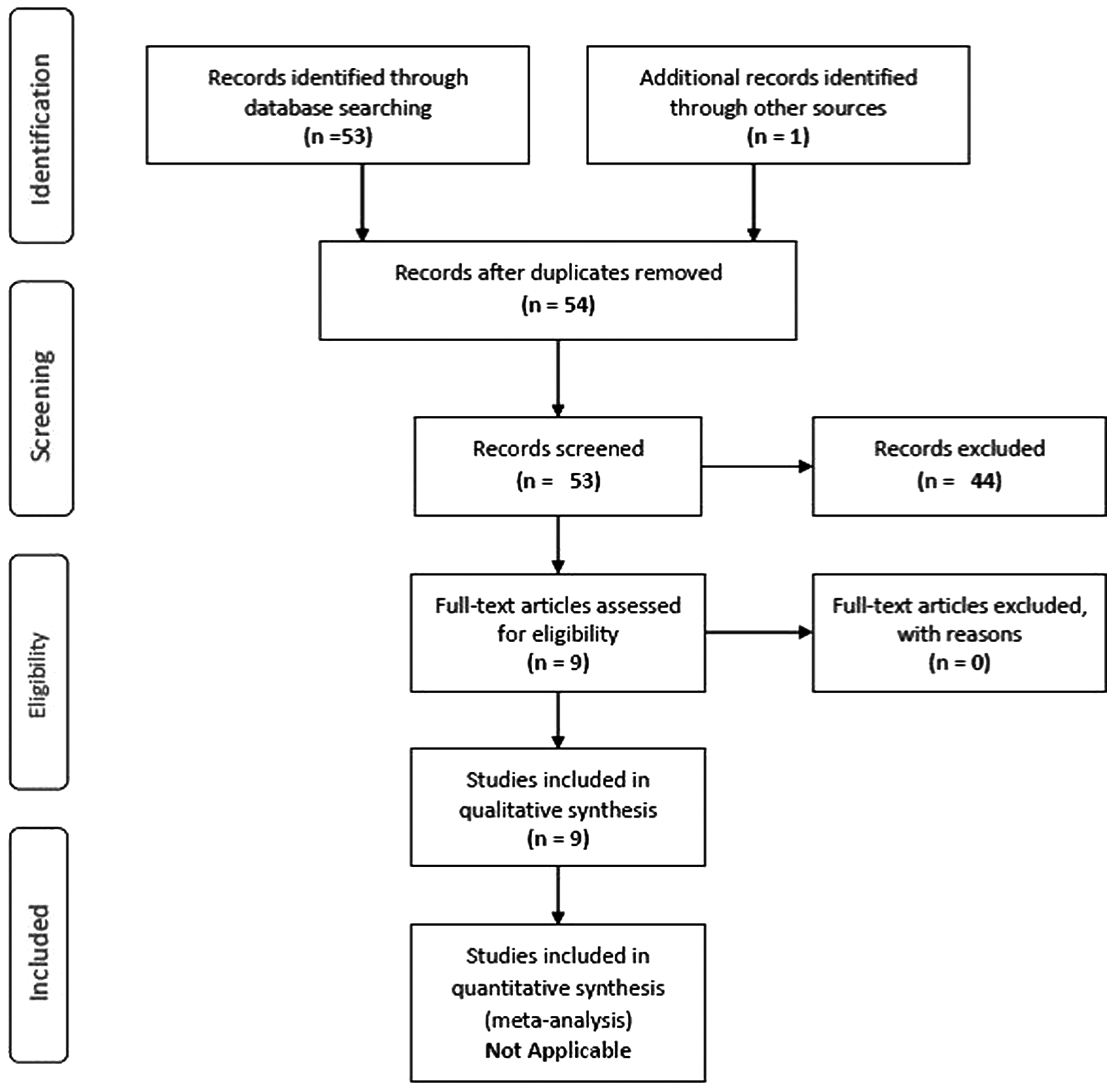
PRISMA flow diagram. PRISMA, preferred reporting items for systematic reviews and meta-analysis.
Only assessment criteria with
Given the continuous nature of the exposure reviewed, that is, TL and the fact that a state of no TL does not exist, we could not assess nonexposure in the cohort studies;
Ascertainment of exposure was considered determined by secure record and rated
CI, confidence interval; CKD, chronic kidney disease; TL, telomere length.
Data extraction, synthesis, and analysis
Data extracted from eligible studies included the study characteristics (i.e., first author, year of publication, study design, study population, sample size), demographics and clinical characteristics of the study population (mean age, gender distribution, body–mass index [BMI]), indicators of kidney function (estimated glomerular filtration rate [eGFR]) (and estimator used), urinary albumin excretion, definition of CKD, mean TL, and the method of TL determination, and indicators of the association between TL and kidney function and CKD (mean differences or p-value for means comparison, correlation coefficients, regression coefficients).
For studies reporting on a continuous association between TL and indicators of kidney function in the form of correlation coefficients or regression coefficients, we noted whether the study reported the accompanying p-value or the 95% confidence interval (CI) around the estimate to determine if the association was significant or not. We further noted the direction of the effects as well as the confounding factors adjusted for in linear regression. For studies comparing mean (or median) TL in participants with and without CKD (or across other groupings based on levels of indicators of kidney function), or conversely, the distribution of levels of indicators of kidney function (or prevalent CKD) across subgroups defined by levels of TL, we noted if p-values, CIs, or other dispersion characteristics were reported to assess if differences were statistically significant, and determine the direction of the effects.
For studies reporting on logistic regressions, or time-to-event analyses on the effect of TL on prevalent or incident CKD, we noted the covariates included in regression models and whether the measure of the association (odds ratio, hazard ratio [HR], and relative risk) was reported with the accompanying p-value or CI to determine if the effect was significant and in which direction.
Given the heterogeneity in both the number and the nature of measures of association across studies as well as in the study designs, biological specimen evaluated, and methods for quantifying TL, a meta-analysis (i.e., statistical pooling of estimates) was not performed. We conducted a systematic review of the evidence instead.
Results
General characteristics of the studies
Fifty-three studies were identified from the PUBMED database search, while one additional study was identified from reference list searches of studies identified from PUBMED (Fig. 1). Eight studies fulfilled the eligibility criteria after a review of the identified studies, with one of the eligible studies comprising two substudies, thus making a total of nine reviewed studies. Eight (89%) (Bansal et al., 2012; Fyhrquist et al., 2010; Hoefield et al., 2010; Lu et al., 2014; Raschenberger et al., 2015a, 2015b; Szeto et al., 2005; Tentolouris et al., 2007) of the selected studies were observational in design, while one (Barden et al., 2016) was a randomized clinical trial; six (67%) studies (Bansal et al., 2012; Barden et al., 2016; Boes et al., 2006; Fyhrquist et al., 2010; Hoefield et al., 2010; Szeto et al., 2005) were prospective observational in design (Table 2).
Baseline mean eGFR using the CKDEPI estimating equation.
AER, albumin excretion ratio; CKDEPI, chronic kidney disease epidemiologic collaboration; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; g/24 h/1.73 m2, grams per 24 hours per 1.73 m2 body surface area; mL/min/1.73 m2, milliliters per minute per 1.73 m2 body surface area; NKF, National Kidney Foundation.
The study population in two (22%) of the studies (Fyhrquist et al., 2010; Tentolouris et al., 2007) consisted of diabetic patients with varying stages of CKD, while another 22% were nondialysis chronic glomerulonephritis CKD patients; only one (11%) study (Bansal et al., 2012) was carried out in known coronary artery disease (CAD) patients with CKD.
Included studies were published between 2005 and 2016 from the following countries: Australia (one study), Germany (two studies), United Kingdom (one study), China (two studies), United States of America (one study), Finland (one study), and Greece (one study). One study was multinational comprising patients from Germany, Austria, and Italy, while there was no study from Africa or South America.
TL determination
A total of 7829 patients with CKD stages 1–5 had TL determination (Table 3). TL was determined utilizing peripheral blood DNA as the substrate and polymerase chain reaction (PCR)-based quantification methods in 7311 participants (five studies), peripheral blood DNA and terminal restriction fragmentation (TRF)-based quantification methods in 216 participants (two studies), and urinary leukocyte DNA and TRF methods in 15 participants (one study), while a cell-based technique (quantitative fluorescence in situ hybridization) was employed in 287 patients (one study) (Table 3).
CRISIS, chronic renal insufficiency standards implementation study; Kb, kilobase pairs; MMKD, mild to moderate kidney disease study; qFISH, quantitative fluorescence in situ hybridization; qPCR, quantitative polymerase chain reaction; TRF, terminal restriction fragment.
Assessment of renal function and definition of CKD
Renal function was assessed in 6/9 studies (66.7%) utilizing creatinine-based eGFR equations. The modification of diet in renal disease equation (MDRD) was employed in 3/6 studies (50%), and the chronic kidney disease epidemiologic collaboration (CKDEPI) equation in 3/6 (50%). Two of the selected studies (2/9, 22%) had determined glomerular filtration rate (GFR) based on clearance techniques, that is, creatinine and iohexol clearances. Bansal et al. (2012), in addition to determining GFR and eGFR with creatinine clearance and a serum creatinine-based equation, respectively, determined eGFR utilizing a serum cystatin C-based estimating equation.
The case selection of CKD patients was made based on eGFR categories in five studies; two (Raschenberger et al., 2015b; Tentolouris et al., 2007) of these utilized the degree of albuminuria/proteinuria in addition to eGFR. In two studies (Raschenberger et al., 2015b; Tentolouris et al., 2007), the 2012 kidney diseases–improving global outcomes (KDIGO) definition of CKD was used, while two studies (Boes et al., 2006; Hoefield et al., 2010) used the National Kidney Foundation's (NKF) case definition of CKD. The selection of CKD cases was based on the prior histologic diagnosis of glomerular damage, that is, glomerulonephritis in two studies (Lu et al., 2014; Szeto et al., 2005).
Association between duration of CKD and TL
One study (Raschenberger et al., 2015b) examined the relationship between the duration of CKD and TL in a heterogeneous group of >5000 CKD patients categorized by CKD duration (<6 months, 6 months to <5 years, and ≥5 years). Patients with the shortest duration of disease, however, had the longest TL. A U-shaped age-, sex-, and eGFR-adjusted association was, however, demonstrated across categories with the shortest relative TL reported among patients with intermediate CKD duration of 6 months to <5 years (mean 0.937, 95% CI: 0.929–0.944). This was significantly shorter in comparison with patients with CKD duration <6 months (mean 0.962, 95% CI: 0.943-.98, p = 0.017). Paradoxically, relative TL was significantly longer among CKD patients with the longest duration of the disease (i.e., ≥5 years) than among patients with intermediate CKD duration (mean 0.954, 95% CI: 0.946–0.961 versus mean 0.937, 95% CI: 0.929–0.944, p = 0.002). This association remained after further adjustment for albumin–creatinine ratio, prevalent cardiovascular disease, diabetes mellitus, educational, and smoking status.
Association between TL, urinary albumin excretion, and microalbuminuria
As shown in Table 4, Raschenberger et al. (2015b) found a paradoxically positive association (ρ = 0.068 p < 0.0001) between the TL and the degree of microalbuminuria in univariable analysis in a heterogeneous group of CKD patients. In an unadjusted analysis among type 1 diabetics, Fyhrquist et al. (2010) demonstrated no significant difference in mean TL between microalbuminuric diabetics and healthy controls (8.1 ± 0.5 Kb versus 8.5 ± 0.9 Kb) nor among macroalbuminuric diabetics and healthy controls (8.4 ± 0.7 Kb versus 8.5 ± 0.9 Kb).
Telomere length associations derived from baseline values only.
8-OHdG, 8-hydroxy-2′-deoxyguanosine; ACE, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; BMI, body–mass index; CoQ, coenzyme Q; CVD, cardiovascular disease; GLM, generalized linear model; HOMA-IR, insulin resistance assessment by homeostatic assay; HR, hazard ratio; hsCRP, high-sensitivity C-reactive protein; LTL, leukocyte telomere length; MAP, mean arterial pressure; n-3F, n-3 fatty acids; PWVcf, pulse wave velocity carotid-femoral segment; UACR, urine albumin–creatinine ratio.
Tentolouris et al. (2007) (Table 4), however, showed that among type 2 diabetic men, quantitative microalbuminuria (β = −0.007, p = 0.007) as well as the microalbuminuric state (β = −0.605, p = 0.004) was associated with shorter TL in univariable analysis and after adjustment for potential confounders, such as BMI, waist circumference, hypertension, smoking status, mean arterial pressure, plasma lipids, duration of glycemia, degree of glycemia, type of antidiabetic treatment, eGFR, insulin resistance assessment by homeostatic assay, use of angiotensin-converting enzyme inhibitors, use of angiotensin receptor blockers, use of statins, pulse wave velocity carotid-femoral segment, pulse pressure, high-sensitivity C-reactive protein, protein carbonyls, 8-hydroxy-2′-deoxyguanosine (8-OHdG), and thiobarbituric acid-reactive substances.
Association between TL and CKD progression
Three studies (Boes et al., 2006; Fyhrquist et al., 2010; Hoefield et al., 2010) evaluated the association between TL and the progression of CKD (Table 4). In the two subcohorts reported by Raschenberger et al. (2015a), there was no significant difference in TL between CKD patients with progressive disease and those without. In the mild to moderate kidney diseases (MMKD) subcohort, those who had CKD progression had a shorter TL compared with those without CKD progression; however, the difference was not statistically significant (0.70 versus 0.77; p = 0.11). A similar trend was reported among a heterogeneous group of CKD patients (including diabetic CKD) in the chronic renal insufficiency standards implementation study (CRISIS) subcohort with TLs of 0.80 and 0.86 in progressors versus nonprogressors, respectively, p = 0.26.
A pooled analysis of the subcohorts demonstrated a trend toward an association between baseline TL and the likelihood of CKD progression after adjustment for age, gender, proteinuria, and GFR (HR per 0.1 decrement in TL = 1.07, 95%CI: 1.00–1.15, p = 0.06). The demonstrated trend was significantly modified by smoking status. Current smokers with shorter TL had a 44% increased risk of progression (HR 1.44, 95% CI: 1.16–1.81, p = 0.001) against a nonsignificant 3% increased risk of progression (HR = 1.03, 95% CI: 0.95–1.11, p = 0.49) in ex- and nonsmokers.
A significant statistical interaction by diabetes status was also apparent in the CRISIS subcohort where TL shortening was associated with a 16% higher risk of progression in diabetes participants (HR per 0.1 unit decrease in TL 1.16, 95% CI: 1.01–1.34, p = 0.03) against a nonsignificant 4% lower risk (HR 0.96, 95% CI: 0.86–1.07, p = 0.47) in nondiabetics (interaction p = 0.09). Fyhrquist et al. (2010) established a protective association between an increase in mean TL and progression of diabetic nephropathy in type 1 diabetic patients with an 81% reduction in the risk of progression (HR 0.190, 95% CI: 0.065–0.558, p = 0.0025) for every Kb increase in TL after adjustment for gender, systolic blood pressure, glycated hemoglobin, smoking status, and duration of diabetes. Similarly, the multivariable model had demonstrated a significant association between the proportion of short telomeres and progression of CKD with an 11.5% increased risk of progression for every percentage increase in proportion of short telomeres (HR 1.11, 95% CI: 1.039–1.195, p = 0.0023).
Szeto et al. (2005), utilizing urine sediment cells for telomere determination, described a significant negative correlation (r = −0.699, p = 0.004) between TL and CKD progression in patients with IgA nephropathy.
Association between kidney function and TL
Only one study (Bansal et al., 2012) evaluated the longitudinal relationship between baseline renal function and subsequent telomere attrition. In the univariable analysis of 608 CKD patients with established CAD, 5 mL decrease in baseline eGFR was associated with statistically significant attrition in TL after 5 years. This univariable association was demonstrable across 3 different measures of kidney function, that is, eGFRCKDEPI (β = −10.8; 95% CI: −17.3 to −4.3; p < 0.05), eGFRcystatin (β = −9.7; 95% CI: −15.5 to −3.9; p < 0.05), and 24-hour creatinine clearance (β = −3.6; 95% CI: −7.8 to −0.1; p < 0.05). This association was not sustained in an age-adjusted model [eGFRCKDEPI (β = −0.4; 95% CI: −7.4 to 6.7), eGFRcystatin (β = −3.4; 95% CI: −9.4 to 2.5), and 24-hour creatinine clearance (β = 1.2; 95% CI: −2.8 to 5.1)].
Discussion
The pivotal biologic role telomeres play in maintaining continued cellular replication and function, as well as the association between premature cellular senescence and human diseases, is well known. In this systematic review of nine studies evaluating the association between aspects of kidney dysfunction (namely albuminuria, eGFR), CKD, and TL, we found an inconclusive association between TL and microalbuminuria status, a significant association between TL and eGFR, and an association between telomere attrition and increased risk of CKD progression—this association was borderline in CKD of heterogeneous etiologies and significant in smokers as well as patients with type 1 diabetes. Finally, a U-shaped association was apparent for TL in relation to diagnosed duration of CKD, with telomere attrition present in participants with intermediate duration relative to those with shorter or longer diagnosed duration of CKD.
The relationship between TL and microalbuminuria/proteinuria had been evaluated in a heterogeneous group of CKD patients as well as a cohort of type 2 diabetic patients in two cross-sectional studies (Raschenberger et al., 2015b; Tentolouris et al., 2007). While a significant univariable positive association (i.e., increasing microalbuminuria associated with longer TL) was found in the heterogeneous CKD group, a significant negative association (i.e., shorter TL with the occurrence of microalbuminuria) was demonstrated among the cohort of type 2 diabetic patients. The positive association reported by Raschenberger et al. goes against the currently held paradigm of shorter TL in disease states. There is, however, emerging evidence to suggest that the reparative telomere lengthening system is a biologic process with an oscillating, rather than a fixed and unidirectional, dynamic. Indeed, as shown by Huzen et al. (2014), increased TL was observed among at least a third of adults from a general population followed up a median of 6.6 years. This phenomenon has also been demonstrated in another general population observed over a 10-year period among whom 44% gained TL (Weischer et al., 2014).
As only a univariable association was reported by Raschenberger et al. (2015b), it remains unclear if the reported direction of the association would have been sustained with adjustment for potential confounders. The influence of confounders on the TL-microalbuminuria relationship as explored by Tentolouris et al. (2007) could therefore explain the completely opposite association between TL and the microalbuminuric state and microalbuminuria in quantitative terms. Another probable reason for the opposing associations could be differences in the techniques utilized in TL determination. While both methods employed (quantitative polymerase chain reaction [qPCR] and TRF) measure the mean TL from pooled DNA, qPCR (by Cawthon's technique) is fraught with an inherent methodological measurement imprecision of varied amounts of DNA in test wells (Cawthon, 2009; Montpetit et al., 2014). This is a known methodological shortcoming of qPCR that has subsequently been improved upon by monochrome multiplex qPCR (Cawthon, 2009).
Raschenberger et al. (2015b) had additionally assessed the cross-sectional relationship between baseline TL and eGFRCKD-EPI and found a positive, although weak, correlation of longer TLs with higher eGFR. This association would appear to validate the conventionally known relationship between TL and cellular/organ function, that is, longer TL indicating a lesser degree of cellular senescence and hence better cellular function (typified by eGFR in the reviewed study). Given the eGFR criterion for CKD case selection (eGFR 30–60 mL/min) as well as the mean age of participants in the study (60 years), it remains unknown if this relationship holds true across all eGFR stages of CKD as well as for younger CKD patients. Additionally, the varying morbidity and mortality risk profiles of individuals with eGFR, 30–60 mL/min, have been variously documented and also recognized by the current KDIGO staging of CKD. With the mean eGFR of 49 mL/min reported by Raschenberger et al. (2015b), a survival bias could be contributing to the findings.
A cardinal strategy in management of CKD patients is the retardation of the progression of disease. The search, identification, and understanding of previously unknown factors contributing to CKD progression are therefore important. From the reviewed studies, we found that among a heterogeneous group of CKD patients, telomere attrition could possibly contribute to CKD progression, although among CKD patients who were current smokers, the contributory role of telomere attrition to the progression of disease was significantly more demonstrable.
Smoking is indeed known to be independently associated with rapid telomere attrition (Huzen et al., 2014). The role of smoking as a risk factor for renal disease as well as its role in the progression of CKD is well known (Bleyer et al., 2000; Ejerblad et al., 2004; Orth and Hallan, 2008; Yamagata et al., 2007). While a number of hemodynamic and nonhemodynamic mechanisms of smoking-induced renal injury have been elucidated, we postulate that smoking also induces renal damage as well as CKD progression through telomere attrition and premature cellular senescence (Orth and Hallan, 2008). An independent contributory role of telomere attrition to CKD progression was also observed among type 1 diabetic CKD patients. Fyhrquist et al. (2010) demonstrated that TL attrition played a role in eventual diabetic CKD progression among type 1 diabetic patients after accounting for diabetes duration and glycemic control. The hyperglycemic state of diabetes mellitus is one of pervasive oxidative stress, which is known to play a causative role in all diabetic complications (Giacco and Brownlee, 2010). Premature cellular senescence induced by the oxidative stress environment may therefore account for the higher risk of CKD progression observed.
Conventionally, peripheral blood cells (PBCs) have been the substrate for TL determination, but there is a dearth of literature to show that mean TL in PBCs reflects the mean TL in component cells making up the various organs within the human body. Szeto et al. (2005) found a significant correlation between urinary sediment mean TL and serum creatinine and the degree of proteinuria, while no significant correlation was found between the PBC mean TL and these measures of renal function/dysfunction. Although the study may not have been adequately powered for the reported observation, it highlights a valid scientific question as to what cell types to utilize for TL determination in patients with kidney diseases. While a kidney biopsy for the sole purpose of determining mean TL from constituent renal cells may not be ethical, the biopsy sample may be a veritable substrate in the kidney disease patient in whom a renal biopsy is indicated.
The uremic milieu in CKD is one of chronic inflammation and oxidative stress. The uremic environment is thus the perfect setting for accelerated telomere attrition and premature cellular senescence. A cross-sectional evaluation of the possible role of the uremic milieu on telomere shortening in one of the reviewed articles demonstrated that while overall TL attrition did occur with longer duration of CKD, individuals categorized with long duration of disease (≥5 years) gained TL when compared with those categorized with intermediate duration disease (6 months to <5 years) (Raschenberger et al., 2015b).
As discussed above, the bidirectionality of telomerase activity is becoming increasingly recognized. The authors (Raschenberger et al., 2015b), however, rightly point out that selection bias may have been at play, specifically a survival bias in which individuals with the longer TL outlived individuals with shorter telomeres. Indeed, the study was conducted in participants with rather moderate CKD (30 mL/min≤ eGFR <60 mL/min or eGFR ≥60 mL/min and proteinuria) with similar average eGFR across categories. In a typical population of CKD patients with variable disease duration, the disease is expected to be much more severe (greater decline in eGFR and attendant complications) in those with longer duration and therefore more likely to be associated with telomere attrition. In addition, duration of CKD had been self-reported by study participants and based on artificially created duration categories.
These artificial categories had the undesirable effects of creating an imbalanced distribution of participants across CKD diagnosed duration groups, with the upper duration group (>5 years) alone comprising nearly half of the participants. This excessive statistical power in the upper duration group alone could distort the relationship and explain the observed U-shaped curve.
Indeed, the relationship of mean TL with duration of CKD was mostly in the expected direction (downward trend) across all lower duration strata. A more rigorous approach would have consisted of collecting the duration data as a continuous variable, then categorizing participants by percentile of diagnosed CKD duration (to allow for a balanced distribution of participants across subgroups), and formally statically testing the departure from linearity of the relationship against the alternative shape. Appropriate statistical algorithms could also have been used to carefully examine the true shape of the association on a continuous scale.
The uremic milieu-TL relationship was also longitudinally assessed by Bansal et al. (2012) who showed that patients with reduced renal function assessed with six different indices of renal function (serum creatinine, creatinine clearance, eGFRCKDEPI, log cystatin C, eGFRcystatin, and log urine albumin–creatinine ratio) had greater reduction in TL when compared with patients with less severe renal dysfunction. The observed confounding effect of age on this longitudinal relationship supports the prevailing role of the natural aging process in ultimate organ dysfunction.
TL has emerged as a novel biomarker of biologic age, cardiovascular risk, and chronic medical diseases, but its role in CKD has not been extensively described. In this systematic review, we have methodically reviewed the available literature to describe the role of TL in the occurrence, duration, and progression of CKD. Heterogeneity of the reviewed studies was a major limitation of this review and precluded a meta-analysis of estimates reported.
Conclusions and Outlook
The findings from the available studies suggest a reciprocal relationship between TL and CKD risk. These include, on the one hand, an association between the presence of CKD or declining kidney function and accelerated telomere attrition, mostly reflecting the confounding effect of the aging process, and, on the other hand, a seemingly conflicting association between TL and CKD, comprising both a protective and deleterious effect of telomere attrition on the risk of CKD. In the context of the available evidence, these mixed associations reflect among others the heterogeneous spectrum of CKD among existing studies, differing biological specimen and methods for quantifying TL, and the probable cellular reparative process of telomerase activity activated by telomere shortening. We postulate that shortening TL is associated with CKD prevalence/occurrence or declining kidney function, but this association is offset by the cellular telomere reparative process in those surviving longer with CKD.
Telomeres and telomerase activity hold great promise for CKD risk stratification and treatment. CKD patient with shorter lengths may constitute a group of patients who might presumably require more aggressive clinical management, while telomerase activation may become a therapeutic approach in retarding CKD progression. Further omics and human genetics research are, however, first needed to delineate the contribution(s) of TL to renal dysfunction, CKD, and related health outcomes.
Footnotes
Acknowledgment
No funding was received for this systematic review.
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.