
Abstract
Abstract
While drugs remain the cornerstone of medicine, herbal medicine is an important comedication worldwide. Thus, precision medicine ought to face this clinical reality and develop “companion diagnostics” for drugs as well as herbal medicines. Yet, many are in denial with respect to the extent of use of traditional/herbal medicines, overlooking that a considerable number of contemporary therapeutic drugs trace their discovery from herbal medicines. This expert review underscores that absent such appropriate attention on both classical drug therapy and herbal medicines, precision medicine biomarkers will likely not stand the full test of clinical practice while patients continue to use both drugs and herbal medicines and, yet the biomarker research and applications focus only (or mostly) on drug therapy. This asymmetry in biomarker innovation strategy needs urgent attention from a wide range of innovation actors worldwide, including governments, research funders, scientists, community leaders, civil society organizations, herbal, pharmaceutical, and insurance industries, policymakers, and social/political scientists. We discuss the various dimensions of a future convergence map between herbal and conventional medicine, and conclude with a set of concrete strategies on how best to integrate biomarker research in a realm of both herbal and drug treatment. Africa, by virtue of its vast experience and exposure in herbal medicine and a “pregnant” life sciences innovation ecosystem, could play a game-changing role for the “birth” of biomarker-informed personalized herbal medicine in the near future. At this critical juncture when precision medicine initiatives are being rolled out worldwide, precision/personalized herbal medicine is both timely and essential for modern therapeutics, not to mention biomarker innovations that stand the test of real-life practices and implementation in the clinic and society.
Introduction
M
Although the use of herbal medicine reportedly exceeds >80% worldwide (Ekor, 2014; Oyebode et al., 2016), presents with large person-to-person and between-population differences in response, there is no commensurate research funding for clinical validation and policy attention. Many modern-day physicians upon induction and training in medicine do not acquire the knowledgebase or fully appreciate the societal dynamics and values that drive herbal medicine, regardless of close family members and friends regularly using herbal medicine.
From a standpoint of history and sociology of medicine, the African born, raised, and eventually western medicine-trained physicians have considerable subconscious exposure to herbal medicine by being born within systems practicing or using herbal medicines. Thus, Africa is anticipated in the near future to have a critical mass of African-born, raised, but Western-trained scholars. In such an innovation ecosystem that embodies both local and global educational forces and research practices, an inside conflict might emerge on what the full spectrum of medicine should be.
Moving forward in precision medicine, there is a need to balance the acquired western knowledge with expectations and realities in local communities in Africa and worldwide. These, often silent, but powerful conflicts in the collective psychology with regard to attitudes toward use/benefits of herbal medicine might now be harnessed constructively at a time precision medicine is emerging and being rolled out worldwide. Some of the initiatives to bolster the significance of herbal medicine are coming through its recognition by international health bodies, such as the World Health Organization (WHO).
The WHO correctly identified the importance of herbal medicines by proclaiming an annual traditional medicine day (which incorporates herbal medicine). This move by the WHO, in our view, helps traditional and herbal medicine to come out of the closet. However, if herbal medicine is to contribute the mainstream medical therapeutics, biomarker research and its applications toward personalized herbal medicine could serve as important catalysts and “open up” avenues for broader life sciences innovation, and address negative thinking and lack of interest toward herbal medicine in mainstream medicine. Africa, by virtue of its vast exposure and experience in the use of herbal medicine and a diverse, ready-to-tap, life sciences innovation ecosystem, could play a game-changing role for the “birth” of biomarker-informed personalized herbal medicine.
This expert review underscores that absence of appropriate attention to both classical drug therapy and herbal medicines, precision medicine will likely not realize its full potential, given that there are many diseases without adequate treatment and the wide co-use of herbal medicine, yet the current biomarker research and applications focus only (or mostly) on conventional drug therapy. This asymmetry in biomarker innovation strategy needs urgent attention from a wide range of innovation actors, including governments, research funders, scientists (including social commentators), community leaders, herbal, pharmaceutical, and insurance industries, and policymakers (Slob, 2012). We conclude with a set of concrete strategies on how best to integrate biomarker research with medical drug treatment.
Precision for Drugs and Herbal Medicines
Highlights from precision medicine for drugs
The term “precision medicine,” is recent and has replaced “personalized medicine,” and these terms are sometimes used interchangeably. Precision medicine refers to a form of medicine that uses an integrated approach utilizing a patient's genomic information, proteomics, metabolomics, and environment (including microbiome profile) to prevent, diagnose, and treat disease (Collins and Varmus, 2015; Day et al., 2017; Lin et al., 2017).
Although there have been many advances in our understanding of genomes and environmental factors (including structural changes on the genomes such as epigenetics and use of herbal medicines), there still remains a challenge in this equation—calling a definitive phenotype. However, with the ever-developing technological advances, there is hope for the development of therapeutic plans devised from mathematical algorithms to adapt interventions to specific/particular patients, resulting in targeted therapy and dosing (Andre et al., 2014).
It is important to note that precision medicine is already in practice, especially in cancer, where specific information about a patient's tumor is being used to diagnose and plan treatment. For example, the drug imatinib (Gleevec) is an ideal candidate for molecularly targeted therapy as its drug target is a fusion protein produced by the BCR/ABL fused genes found in chronic myelogenous leukemia and absent in nonmalignant cells (Marcucci et al., 2003).
The drugs trastuzumab (Herceptin), lapatinib, and capecitabine are humanized antibodies approved for treatment against breast cancer presenting with human epidermal growth factor receptor 2 (HER2)-positive genetic profile (Geyer et al., 2006; Piccart-Gebhart et al., 2005; Romond et al., 2005; Slamon et al., 2001). Lung cancer patients with a positive epidermal growth factor receptor (EGFR) mutation in their tumors have been shown to respond better to the drugs gefitinib (Iressa) and erlotinib (Tarceva), which specifically target this mutation, while colon cancer patients positive for a mutation in KRAS do not benefit from cetuximab (Erbitux) and panitumumab (Vectibix) (Comis, 2005; Greenhalgh et al., 2015). Thus, genomic information is driving research in the development of targeted treatment strategies that will help in achieving therapeutic efficacy.
Targeted dosing is another core practice of precision medicine. For example, warfarin, a common anticoagulant, is now having its doses guided by genomic information with respect to CYP2C9 and VKORC1 genes (Kimmel, 2015; Pirmohamed et al., 2013). Thiopurine drugs, such as 6-mercaptopurine, azathioprine, and thioguanine, prescribed for the treatment of various diseases, including hematologic malignancies, inflammatory bowel disease, and rheumatoid arthritis, and acting as immunosuppressants in solid organ transplant, are affected by genetic variation in thiopurine methyltransferase (TPMT) gene (Nguyen et al., 2011), and this information is now integral in treatment decision-making.
Precision medicine relies heavily on bioinformatics integrating an individual's molecular profiles (-omics), and environmental exposures to bring about a holistic understanding of the best possible intervention. This makes the use of high-throughput technologies such as microarray panels and next-generation sequencing highly essential in achieving precision medicine (Dong et al., 2015; Gagan and Van Allen, 2015; Guo et al., 2013; Ventola, 2013). Another essential step for precision medicine is proteomics and understanding the pathways for protein interactions so as to identify multiple molecular regulatory points for unique therapeutic intervention (Urban, 2015; Zollars et al., 2016).
While acknowledging the significant contribution of genomic knowledge, integration with other -omics could be the panacea to our understanding of complex diseases such as cancer, non-insulin-dependent diabetes, and autoimmune diseases. Thus, proteomics adds an additional layer of refining information critical to the success of precision medicine (Britton et al., 2014; Eckhard et al., 2016; Zhou et al., 2016).
Metabolomics has a role to play in precision medicine (Clish, 2015; Wishart, 2016). The development of chromatography coupled to mass spectrometry (MS) and nuclear magnetic resonance (NMR) spectroscopy such as GC-MS/LC-MS/UPLC-MS has advanced the profiling of thousands of metabolites in biological systems with a very short time (Cajka and Fiehn, 2014; Fiehn, 2016; Pan et al., 2010). With the use of commercially available databases, spectra data generated can be annotated and processed, linking metabolite and metabolomic biomarker to ultimately come up with individualized response profiles, helping achieve precision medicine.
Toward “Precision Herbal Medicine”
The evolving examples of precision medicine for drug treatment underscore using “omics” and “multi-omics” approaches (e.g., genomics, proteomics, and metabolomics) (David et al., 2015; Kurnat-Thoma, 2011). Yet, the concept of precision medicine must be defined in a broader and holistic manner to be able to bring real-life health transformation to suit an individual's needs. Environmental and lifestyle intervention factors are also important in achieving precision medicine (McGill, 2015).
An example is the notable decline in breast cancer rates/incidence and associated improvement in quality of life in the United States since 2002, which have been attributed to reduction in postmenopausal hormone (Sprague et al., 2011) and not attributable to “targeted therapy” or “targeted dosing.” Precision medicine therefore can be viewed more broadly as an inclusive, prospective approach to preventing, diagnosing, treating, and monitoring disease in ways that achieve optimal efficacy in relation to an individual's healthcare needs. This definition often has become a healthcare paradigm shift that is frequently called preventive medicine.
The omics application focus on herbal medicine could therefore help profile drug targets, compounds, and metabolites to prospect for new treatment options, to achieve effective therapy for conditions of public health concern, where current treatments are not adequately effective, and this could include known and documented herbal medicines. For example, St. John's wort (SJW, Hypericum perforatum) is one of the most widely studied and herbal medicines used for the treatment of depression. It was profiled using HPLC-MS and found to contain significant amounts of naphthodianthrones and phloroglucinols, which give it antidepressant properties, among other pharmacodynamic properties (Vacek et al., 2007). Several studies have shown interindividual variability and interaction with other medications, including antiretrovirals (ARVs), midazolam, and digoxin (Imai et al., 2008; Johne et al., 1999).
A clinical trial involving SJW found no statistically significant difference between SJW and placebo (Grobler et al., 2014; Sarris et al., 2012); however, SJW monotherapy for mild and moderate depression was found to be superior to placebo in improving depression symptoms (Apaydin et al., 2016). A “personalized herbal medicine” initiative involving SJW will be apt where multi-omics technologies targeting components of therapeutic value and focusing on biomarker development will be implemented to maximize the incorporation of SJW into clinical practice. The strategic application of “-omics” tools and technologies will allow the achievement of “personalized herbal medicine” intervention and incorporation into precision medicine from indigenous knowledge systems (IKS) (Fig. 1).
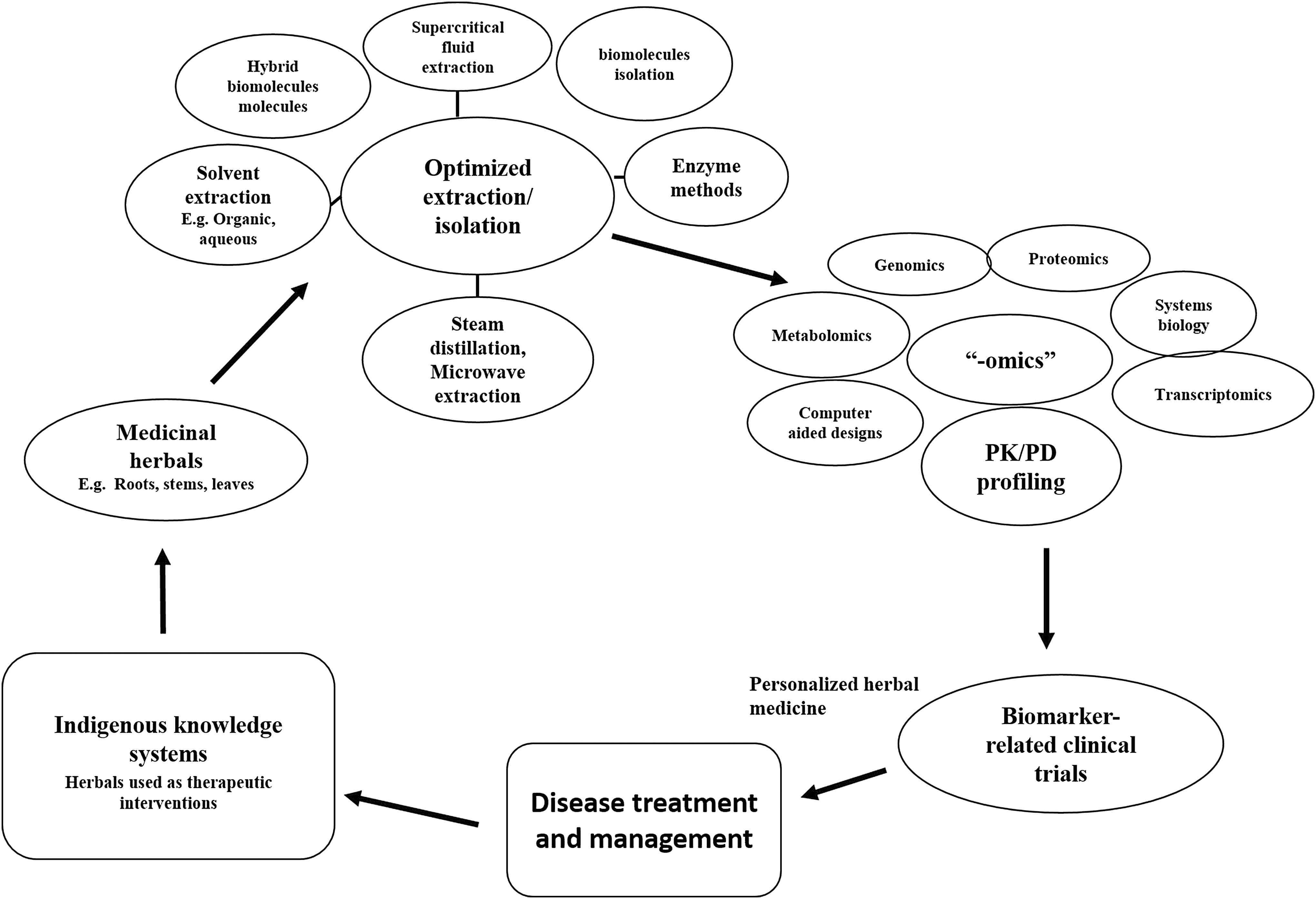
Roadmap toward achieving “personalized herbal medicine” from indigenous knowledge.
The IKS background of herbal usage allows for the therapeutic efficacy of herbals to be obtained from practicing indigenes, and with the application of the current technological revolution, these herbals can be further studied, leading to possible incorporation into medical treatment regimens. The backbone of precision medicine initiative is increasing knowledge accumulated through research, technological advancement in methodologies to evaluate parameters, incorporation of patient characteristics (clinical and demographic), and robust electronic record systems that enable the bringing together of all factors needed to make a definite diagnosis. This would include due consideration to both utility of both conventionally prescribed medications and widely acclaimed herbal medicines for particular conditions.
The pressure to bring herbal medicine out of the closet is coming from the attitudes and practices of patients themselves, who routinely use herbal remedies and supplements in a bid to increase their chances of getting cured. Thus, precision medicine initiatives should increasingly factor-in herbal remedies to achieve its goals. However, research in herbal medicine should be made attractive so that advances that have been seen in the discovery and development of conventional medicines are also made to happen in this field. There are several conditions where both conventional and herbal medicines are reportedly used (Table 1); however, more focused studies need to be carried out to evaluate the effectiveness of such concurrent use of both conventional and herbal medicine (Doos et al., 2014; Roberts et al., 2014; Wang et al., 2010).
Mainstay interventions used for treating the main disease and comorbidities.
trade names and herbal components.
CVA, cerebrovascular accident; CVD, cardiovascular disease; EFV, efavirenz.
In the treatment of comorbidities, including cancer, diabetes, hypertension, HIV/AIDS, tuberculosis, and leprosy, multiple drug therapy is the rule rather than an exception. This multidrug therapy exploits synergistic and additive properties of individual drugs, but the challenge is minimizing adverse drug effects. The WHO has played an active role in promoting multidrug therapy in HIV/AIDS, tuberculosis, and malaria by providing resources and expertise to achieve positive outcomes. Most often, due to the multidrug therapy approach being used to combat diseases, there are possible interactions that result in adverse effects (Deps et al., 2007; Mitnick et al., 2016; Törün et al., 2005). Thus, it is important to also come up with expert guidelines on the co-use of conventional drugs and herbal medicines, emphasizing on the constituent molecules that are effective in different herbal medicines.
The phytocomplex nature of herbal medicines, if harnessed, could be key to unlocking most therapeutic challenges of global health. An example can be observed in bitter melon (Momordica charantia), which contains multiple bioactive components such as polypeptide-p, cucurbitane-type triterpenoids, steroidal saponins called “charantins,” and insulin-like peptides (Cefalu et al., 2011). Applied -omics- tools and technologies on bitter melon could be key for diabetes treatment through biomarker research and developments (R&D).
Panax ginseng, Allium sativum, Ginkgo biloba, and Aloe vera, which have been used extensively for multiple indications, including diabetes, hypertension, and lipid lowering, seem to be a bed of unharnessed therapeutics. Extensive R&D for biomarkers can potentially incorporate their prescription as “personalized herbal medicines” for treating some of these complex pathophysiological conditions (Buettner et al., 2006; Koltermann et al., 2007; Yeh et al., 2003).
Clinical trials involving A. vera have shown its effectiveness against wound healing, microorganisms, reducing sugar levels, and blood lipid levels (Choi et al., 2013; Prueksrisakul et al., 2015; Sahebnasagh et al., 2017). A. vera has been developed to be used especially as an effective topical therapeutic agent, without necessarily trying to isolate one active or individual component, although the constituents profile is mostly established (Sharrif Moghaddasi and Kumar Verma, 2011). This conveys that not all herbals have to be isolated into components through a “reductionist” approach, but biomarker R&D efforts can be used to maximize extraction to get the supposed active components optimized for therapeutic interventions.
Examples and Frontiers of Personalized Herbal Medicine
Cancer therapeutics
Chemotherapy serves as the first line of treatment for most cancers, notwithstanding the successful advent of development of targeted agents for cancer over the years (Rizzo et al., 2008). Development of chemoresistance is common and almost a predictable phenomenon when monotherapy is adopted, considering the molecular complexities involved in cancer.
The complexity of genetic background and molecular pathways of oncogenesis makes it strategically impossible to shut down only one molecular target to combat cancer, hence the now preferred multidrug therapy approach that targets multi-pathways. Targeting two or more molecular mechanisms in a single pathway allows maximal inhibition of that pathway. Over the years, the effect of multitarget approach has been clinically and preclinically explored for specific agents.
For example, chemotherapy has evolved from the classical cyclophosphamide/vincristine (Oncovin)/procarbazine/prednisone (COPP) combination as initial treatment for conditions such as Hodgkin lymphoma patients to over 12 combination regimens specific for different types of cancer specific to individuals (Diehl et al., 1998; Thakar et al., 2014). The adriamycin/bleomycin/vinblastine/vacarbazine (ABVD) combination regimen is used in the Hodgkins disease, while under the leadership of Diehl, a novel dose-intensive chemotherapy program using seven drugs bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone (BEACOPP) was developed to improve treatment of Hodgkin lymphoma (Eichenauer and Engert, 2009; Sieber et al., 2003).
A Stanford group introduced the Stanford V regimen, a relatively dose-intense brief regimen made of doxorubicin, vincristine, mechlorethamine, vinblastine, bleomycin, etoposide, and prednisone in combination with radiation therapy (Canellos et al., 2014). From the above, it is observed that for cancer treatment alone, several combinations of chemotherapeutic drugs are needed to cure or manage the disease. Complex conditions like cancer exists with comorbidities that also require concomitant treatment options to give complete cure to patients.
Case reports have indicated the use of combination therapy of chemotherapeutic medications, in addition to other prescribed medications like elvitegravir, cobicistat, emtricitabine, and tenofovir disoproxil fumarate for antiretroviral therapy for HIV/AIDS co-infection (Thakar et al., 2014). In cancer co-occurring with diabetes in patients has, in addition to chemotherapy, metformin, a well-tolerated antidiabetic drug, being added to the treatment regimen for the management of the diabetes and serving as an effective chemotherapeutic adjuvant (Zhang and Guo, 2016). The combination therapy involving chemotherapeutic medications and antidiabetic medications, although may be beneficial, may also present possible interactions involving metabolism and pharmacogenetic response in individuals, which can lead to possible adverse drug reactions (ADRs) (Chen et al., 2013).
The multidrug therapy approach in combating cancer and its comorbidities, although effective, comes with possible side effects associated as a result of multiple perturbations, which result from three possible types of interaction that can be classified as synergistic, antagonistic, and/or additive (Segrè et al., 2005). What is conspicuous, in the preceding examples of combination treatment, is the absence in the consideration of inclusion of herbal medicine. Herbal remedy approaches in therapeutics are also becoming popular options in cancer therapy as herbal remedies are multi-phytoconstituted, which, based on the principle of multicomponent drugs, act in a synergistic manner to achieve maximum therapeutic effect. Herbal medicine has come through a slow evolutionary process as different populations and individuals continue to discover transforming therapeutic potential.
Given that cancer is a multifactorial disorder resulting from continuous cell division, remedial strategies target tumor cells with the aim of achieving minimal side effects on normal cells. Herbal remedies assumed to be of natural decent and hence offering minimal side effects serve as a two-pronged approach of achieving effective therapeutic efficacy with minimal or no side effects. The concept of precision medicine is ideally linked to targeting mechanisms of diseases with specific compounds.
While this approach can be effective in certain diseases, there is no single target involvement in multifactorial diseases, especially with resistant conditions. The integration or use of herbal remedies therefore will be beneficial since herbs contain multiple active components, which are likely to target multiple mechanisms (Ling et al., 2014). An average of 70% of approved anticancer medication over the past 25–30 years were either herbal medicines or developed based on experimental data generated from natural products (Du and Tang, 2014; Newman and Cragg, 2007; Rayan et al., 2017).
Some of the most commonly used anticancer herbal medicines include Rhizoma Polygoni Cuspidati, Fructus Schisandrae Chinensis, and Rhizoma Zingiberis Recens. These herbals contain many polyphenolic compounds that have varied therapeutic effects and target multiple mechanisms. Launaea taraxacifolia (African lettuce) is commonly used in the western part of Africa for the management of pathological conditions, including cancer, diabetes, hypertension, and lipid lowering. In vitro studies on the anticancer effects of the African lettuce on esophageal cancer have shown the potential of this herbal to trigger apoptosis and prevent cell division (Thomford et al., 2016b), which complements cancer therapy.
Application of metabolomics and transcriptomics will improve biomarker targets for effective utilization of African lettuce as a personalized herbal medicine for cancer. Through biomarker approaches, vincristine and vinblastine were discovered and effectively used for cancer treatment; thus, an integrated OMICs approach will improve current herbals used for cancer treatment through cancer biomarker medicine. Making the treatment or management of cancer more “precise” will require targeting specific pathways to achieve effective therapeutic outcomes with less side effects to the patient. A “personalized herbal medicine” intervention as part of precision cancer therapy may give a positive outlook in the face of multifactorial complications observed in cancer.
Diabetes
Hyperglycemia is the hallmark of diabetes; thus, glycemic control is the main goal of treatment to prevent chronic complications. Over the past few decades, stronger evidence has shown the multifactorial complications of diabetes with cardiovascular conditions like hypertension, hyperlipidemia, and nephropathy leading to guidelines and approaches that emphasize the need for concomitant treatment of diabetes with its associated complications (American Diabetes Association, 2010), to improve patients' functioning quality of life and decrease mortality risks.
According to previous studies, most adults with diabetes have at least one comorbid chronic condition (Druss et al., 2001) and as many as 35% have at least three (Lalkhen et al., 2015; Maddigan et al., 2005; van Olmen et al., 2012). Thus, guidelines became necessary, and most of these show the complexity associated with diabetes treatment or management.
Metformin, currently the first-line treatment for type 2 diabetes, improves diabetes control primarily by suppressing hepatic glucose production and improving insulin sensitivity (Foretz and Viollet, 2015). Glyburide, a sulfonylurea, has also been one of the drugs used for treating diabetes with an additional property of inhibiting NLRP3 inflammasome and subsequent IL-1b activation in macrophages (Lamkanfi et al., 2009). Similarly, gliclazide has been reported to decrease the expression of inflammatory markers and endothelial dysfunction in patients with type 2 diabetes, in addition to significantly decreasing glycemic levels (Drouin et al., 2004).
It is common for diabetic patients to have comorbid complications requiring multidrug therapy approaches. As such, a look at the current milieu of medications used in treating diabetes and its complications shows the use of statins (Gross et al., 2005), Vitamin D (Lim, 2014), angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers, beta-blockers, and calcium channel blockers (CCBs) (Arauz-Pacheco et al., 2003; Ganesh and Viswanathan, 2011). The multifactorial pharmacological treatment used in diabetes and its comorbidities elevates the risk of patients experiencing ADRs or drug interactions (May and Schindler, 2016). These and other complications have resulted in patients resorting to complimenting their treatment regimen with herbal medicines.
Herbal medicine usage in diabetes management is a common occurrence in populations in health transition and even in advanced economies. Randomized controlled trials using Silymarin (milk thistle, silybum) (Fallahzadeh et al., 2012; Rafieian-Kopaie and Nasri, 2012) and curcumin (turmeric) (Khajehdehi et al., 2011) show significant reduction in levels of critical parameters such as albuminuria, urine TNF-α, urine, serum malondialdehyde (oxidative stress marker), TGF-β, and IL-18 compared to baseline. These biomarkers can serve as basis for a “personalized herbal medicine” diabetes therapy. If these herbals can significantly reduce sugar levels and positively modulate cardiovascular biomarkers, a concrete R&D intervention will position some of these herbal medicines in precision diabetes medicine.
The use of herbal medicines for diabetes management remains largely unregulated as patients with diabetic complications and comorbidities seek to compliment prescribed medication with these herbal medicines without informing their physicians. The role of these herbal medicines in precision medicine remains largely uncharacterized. The few randomized controlled trials available have shown the potential role of herbals in managing diabetes and its comorbidities.
Hypertension
Hypertension is a global epidemic; in many countries, 50% of the population >60 years of age has hypertension (Lim et al., 2012). The prevalence of hypertension is steadily increasing, even with the expanded use of antihypertensive medications. It is widely recognized that hypertension is associated with increased cardiovascular and all-cause mortality, independent of other risk factors (Chobanian et al., 2003).
Hypertension remains a major risk factor for cardiovascular morbidity and mortality globally (Lim et al., 2012), for which the proposed management is normally based on two principal complimentary approaches, lifestyle modification and lifelong adherence to antihypertensive medication. Comorbidities of hypertension to which multidrug therapy is required include chronic kidney disease (CKD), diabetes, obesity, hyperlipidemia, and metabolic syndrome (Bozkurt et al., 2016; Kennard and O'Shaughnessy, 2016).
There exists an independent continuous relationship between hypertension and the incidence of several cardiovascular events, including stroke, myocardial infarction, heart failure, and peripheral arterial disease, as well as end-stage renal disease (Britton et al., 2009; Kalaitzidis and Bakris, 2010; Lewington et al., 2002), irrespective of age or ethnic groups (Brown et al., 2007; Lawes et al., 2003). Understanding the influence of comorbidities in patients with cardiovascular disease (CVD) remains of great interest as they impact healthcare outcomes such as mortality (Fortin et al., 2007; Valderas et al., 2009), health-related quality of life, quality of healthcare, and a more complex medical management of patients (Ritchie, 2007; Wolff et al., 2002).
A study conducted in the United States revealed that out of 90% patients taking medication for hypertension, only ∼60% were involved in some form of lifestyle change to control their blood pressure (BP) (Moser and Franklin, 2007). This therefore implies that a significant majority of hypertensive patients rely on medication for the control of their BP. The comorbidities that are associated with hypertension, which often occur within the same period, require the use of multidrug therapy. The National Institute for Health and Care Excellence has proposed several guidelines to rationalize treatment for patients with hypertension and comorbidities such as CKD, chronic heart failure, diabetes, and atrial fibrillation (Kennard and O'Shaughnessy, 2016; McCormack et al., 2012). Beta-blockers and diuretics have been used for the treatment of hypertension for more than three decades.
Although their effectiveness over the decades remains undisputed, studies have shown increased risk of beta-blocker usage for stroke, cardiovascular events, and mortality, with only two comparison studies showing evidence of significant cardiovascular benefit (DiNicolantonio et al., 2015; Larochelle and Lacourcière, 2014; Warmack et al., 2009). The multidrug therapy approach to hypertension control includes fixed combination doses or drugs added sequentially one after the other.
Different classes of drugs are used in combination for the treatment of hypertension, taking advantage of their complimentary action. The commonly used classes of antihypertensive agents include alpha and beta blockers, ACEIs, angiotensin receptor blockers (ARBs), calcium antagonists (CCBs), and thiazide diuretics. Several studies have demonstrated the antihypertensive effectiveness of combinations of ARBs and diuretics in low doses, showing substantially greater reductions in BP and higher response rates than either of the treatments alone (Chen et al., 2009; Heran et al., 2008; Mimran and Weir, 2005; Musini et al., 2014). The use of ARB and CCB combinations, apart from BP lowering, is an independent benefit on morbidity and mortality in patients with hypertension and comorbid conditions.
A combination of telmisartan and amlodipine at the appropriate dosages decreased BP, resulting in a decreased urinary albumin rate and other parameters of kidney function (Fogari et al., 2007). Clinical studies have emphasized the significant demonstration of improvement involving combination therapy of properly dosed ACEI and ARB regarding target organ damage, specifically heart failure and proteinuria. Combination treatment involving candesartan and lisinopril was significantly effective than monotherapy in reducing BP, and resulted in a greater decrease in albuminuria (Mogensen et al., 2000).
Although we have earlier elucidated the many different antihypertensive drugs that are available, BP levels of approximately two-thirds of patients under treatment do not reach the target level (James et al., 2014; Odusola et al., 2016), and for those who reach, there is still high cardiovascular morbidity and mortality rate (WHO, 2007). This makes achieving precision medicine with respect to hypertension treatment challenging.
Some patients using conventionally prescribed medication without the expected results choose to add “nonconventional” therapy to prevent and manage resistant hypertension (Brook et al., 2013), with robust evidence of BP-lowering effects reported for some herbal therapies (Xiong et al., 2013). For example, Chinese herbal medicine (CHM), an important component of traditional Chinese medicine therapies, has played a tremendous role in relieving hypertension-related signs and symptoms for centuries in East Asia (Wang and Xiong, 2012, 2013).
African traditional medicine, one of the oldest and most sort after of all therapeutic systems, also has a rich biological diversity in herbals used in the treatment of different diseases, including hypertension (Gurib-Fakim and Mahomoodally, 2013). However, there is generally very poor record keeping on the administration or general use because funding has not been made available to advance our understanding. Traditional herbal medicine is proposed to have a significant impact on hypertension treatment and control in sub-Saharan Africa, with a high use among adults where prevalence of hypertension ranges from 38.5% to 90% (Eddouks et al., 2002; Oreagba et al., 2011; Singh et al., 2004). Herbal medicine used as antihypertensives have different effects on the vasculature and biochemical process that results in a decrease in BP.
It has been reported that herbal medicines such as P. ginseng, A. sativum, G. biloba, and A. vera have potential usage for multiple indications, including hypertension and lipid control (Buettner et al., 2006; Koltermann et al., 2007). Elucidated mechanisms by which these herbal medicines elicit their effects include reducing NADPH activity, scavenging reactive oxygen species (ROS), inactivating ROS produced by β-adrenoceptor stimulation, inhibiting lipid peroxidation, inhibiting ACE, blocking Ca2+ channels, and increasing nitric oxide bioavailability (Al Disi et al., 2015; Anwar et al., 2016; Xiong et al., 2013).
These are biomarkers based on which current antihypertensives are prescribed, and based on elucidated mechanisms in relation to some of these herbal medicines, drug development strategies involving herbal medicine for hypertension management can be mapped out to achieve a personalized herbal medicine intervention. Taking the above into consideration and the different mechanisms by which herbals and prescribed antihypertensive drugs work, precision medicine involving herbals should be worked out to combat the epidemic of hypertension.
HIV/AIDS
Multidrug therapy in the form of antiretroviral therapy (ART) has significantly improved clinical outcomes of HIV-infected individuals by suppressing viral replication and slowing immune deterioration. The results of ART, which involve “drug cocktail” combinations, have improved quality of life and longevity. Comorbidities associated with HIV include hepatitis, mental health disorders, CVD, diabetes, hyperlipidemia, hypertension, and liver disease (Lorenc et al., 2014; Nlooto, 2017).
The immunodeficiency that is caused by chronic HIV infection results in increased risks of coinfections with pathogens that are controlled by innate and adaptive cellular immune responses, and some that are controlled by phagocytic antibody responses such as tuberculosis, bacterial infections, herpes simplex, oral thrush, or candidiasis (Chang et al., 2013; Nlooto, 2017). The challenge is that the administration of combination ART or ART in HIV coinfections does not always restore the pathogen-specific immune response to normal levels.
More than 36 FDA-approved anti-HIV drugs are currently available at the market for use by persons living with HIV/AIDS. HIV treatment or management involves controlling CD+ target cells as a crucial part of the viral life cycle, which use host cells to replicate itself and thus proliferate. Reverse transcriptase inhibitors prevent viral RNA from being reverse transcribed to DNA, thus blocking integration of the viral code into target cells. Protease inhibitors (PIs), on the other hand, affect the viral assembly process in the final stage of the viral life cycle, preventing the precise cutting and structuring of the viral proteins before their release from host cell. PIs therefore effectively reduce the number of infectious virus particles released by an infected cell (Adams et al., 2004; Arts and Hazuda, 2012).
Efavirenz (EFV), a non-nucleoside reverse-transcriptase inhibitor (NNRTI) continues to be one of the most commonly prescribed antiretroviral drugs as a first line of treatment in combination with other antiretroviral drugs (Kryst et al., 2015). Several clinical trials have demonstrated the effectiveness of EFV with other categories of ARVs based on different mechanisms of action to effectively eradicate the virus (Cohen et al., 2011; Gazzard et al., 2011; Molina et al., 2011; Nelson et al., 2011a). EFV pharmacokinetics is affected by several factors, including host genetics, ethnicity, gender, body mass index, hepatic impairment, disease status, and pregnancy (Burger et al., 2006; Ngaimisi et al., 2013; Stöhr et al., 2008). Focus on host genetics has been on drug-metabolizing enzymes involved in EFV metabolism. EFV is primarily metabolized by CYP2B6 with minor contributions by CYP1A2, CYP2A6, CYP3A4, CYP3A5, and UGT2B7 (Swart et al., 2015).
The drug-metabolizing enzymes involved in the metabolism of EFV are highly polymorphic and exhibit interindividual variability in expression and function (Cusato et al., 2016; Zanger and Schwab, 2013). Pharmacogenetic based EFV dose modification involving DMEs and other factors has been suggested for different populations to bring out optimum clinical response (Mukonzo et al., 2014; Ribaudo et al., 2010; Salem et al., 2014). EFV, although widely used and serves as one of the first-line ARVs, has side effects that may occur with continuous use such as dizziness, confusion, rash, hallucinations, elevated liver enzymes, and depression (Antinori et al., 2017; Nelson et al., 2011b). ARVs are able to reduce viral load to its barest minimum, but cannot completely eradicate the virus as the virus moves into a latent stage, which evades the action of administered ARVs.
The scourge of HIV/AIDS has increased the prospects of finding an everlasting cure to this global pandemic. Aside the investments in ARVs, an overlooked potential for combating HIV/AIDS is herbal remedies. Herbal medicine usage among HIV/AIDS patients has increased due to adverse effects associated with conventional ARVs, restricted access to quality ARVs, and affordability (Awortwe et al., 2013; Endale Gurmu et al., 2017; Langlois-Klassen et al., 2007; Namuddu et al., 2011; Nyangu and Mokwena, 2015). HIV patients are also accessing herbal medicines as alternate forms of treatment as some patients believe these herbals have antiretroviral activities that help reduce viral load.
Herbal medicine use is very common among people of African and Asian descent; however, in recent studies, it has been shown that there is global use of herbal medicine, including Europe, North America, and the Caribbean (Orisatoki and Oguntibeju, 2010). Among the various herbal medicines used for HIV treatment and management among the various populations include black cumin (Nigella sativa) (Salem, 2005), garlic (A. sativum), moringa (Moringa oleifera) (Marrufo et al., 2013), Hypoxis hemerocallidea (common name: African potato), and Sutherlandia frutescens (Mills et al., 2005). The proposed mechanism of action of these herbal medicines involves immunomodulatory activities and inhibiting viral replication.
Knowing HIV/AIDS affects host immune function, immune biomarkers can be teased out from these herbal medicines to rationalize new “personalized herbal medicine” options for combating HIV/AIDS. These herbs also contain phytochemicals that also have therapeutic effects on HIV-related signs and symptoms- as well as comorbidities such as hypertension, dyslipidemia, and even certain cancers (Langlois-Klassen et al., 2007).
Reported clinical trials of herbal medicines and herbal concoctions in HIV/AIDS patients have significant increased CD4 counts (Wang et al., 2006) and decreased HIV RNA levels (Sangkitporn et al., 2005). Looking at the devastating effects of HIV/AIDS across the globe, assessing the therapeutic effects of herbal remedies on human immunodeficiency virus could help focus herbal medicine in HIV precision medicine.
Perspectives and Outlook
A network approach to personalized herbal medicine
Precision medicine is no longer an area that one specialty can claim alone; it is an ecosystem where various parts in the healthcare system must be integrated to achieve the common goal of giving patients the best possible care (Fig. 2). In practice, it involves the utilization of the unique patient characteristics, patient's disease status (including comorbidities), and environmental factors (including microbiota profiles and lifestyle), all integrated to arrive at the best possible intervention for the patient, which may include individual or combinations of drugs/herbal medicines.
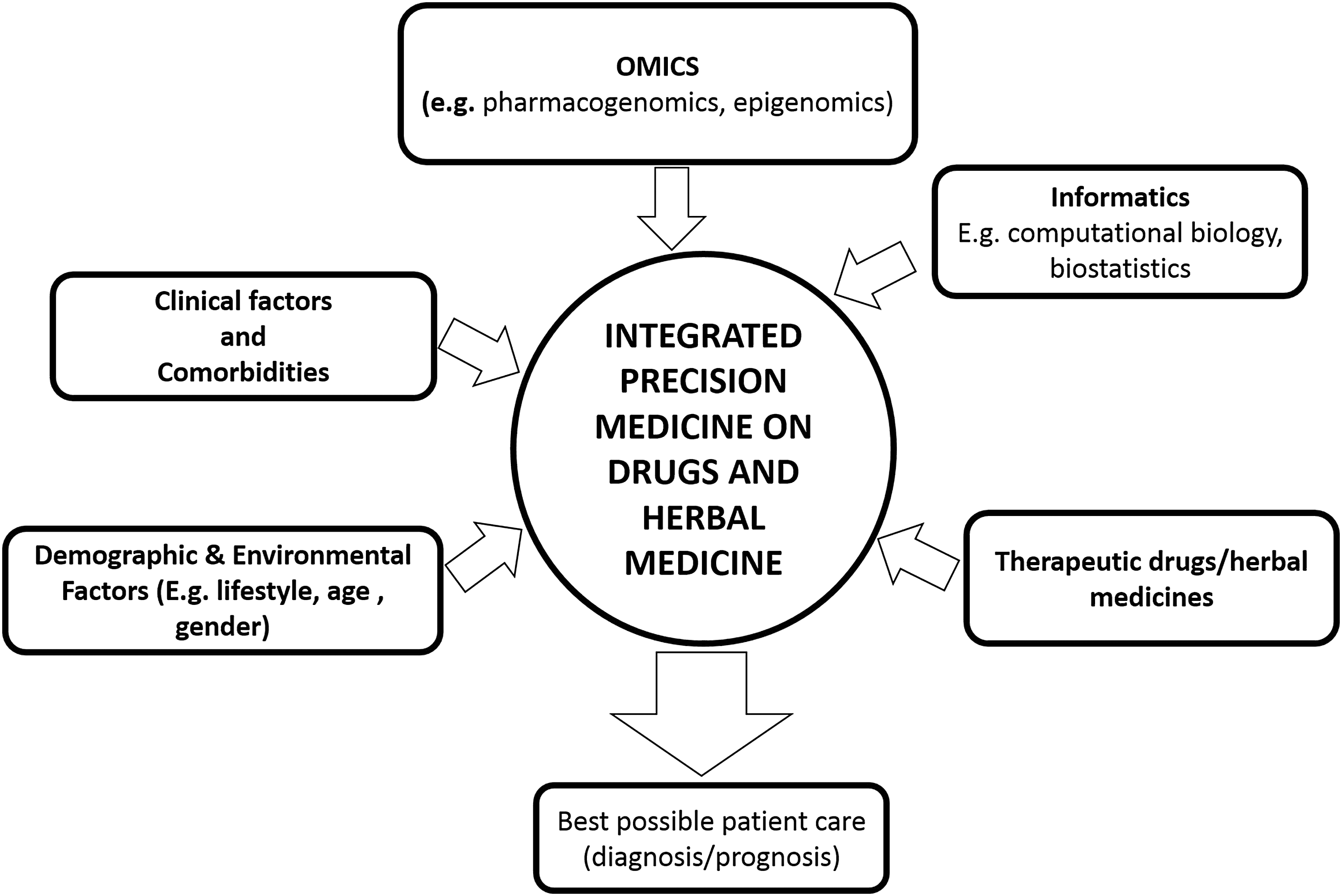
A graphical representation of integration of omics, clinical medicine, and treatment options involving conventional and herbal medicine in achieving precision medicine for diagnosis and prognosis.
We emphasize that medicinal herbal remedies should be incorporated in this precision medicine algorithm after understanding their effects alone or in combination, which achieves best responses. This calls for de-stigmatization of research in herbal medicine as well as targeted funding to raise our understanding of the contribution of this area of medicine to global health.
As illustrated in Figure 2, an effective inclusion of herbal medicine in “precision medicine” will require application of “-omics-” technologies such as genomics, transcriptomics, metabolomics, proteomics, and informatics (e.g., bioinformatics) to break the barrier where herbal medicine is often neglected. Achieving “personalized herbal medicine” leading to new intervention strategies for complex pathophysiological conditions can occur from a conscious R&D approach in application with biomarker medicine. “Personalized herbal medicine” can be strategically positioned in the precision medicine ecosystem and positively promoted, where there is enough scientific evidence elucidating its mechanisms of action, conferring on it the requisite legitimacy.
Utilizing omics-based approaches is useful in elucidating and understanding the mechanism of action of the various phytochemical components of herbal medicine and enhancing their action. Phyto-fingerprinting of these herbs using metabolomics approach such as GC-MS/LC-MS/UPLC-MS and NMR spectroscopy will advance the correct profiling of metabolites (Pelkonen et al., 2012; Thomford et al., 2016a; Wang et al., 2016). Quantifying these metabolites and chemicals in herbals will also help advice the addition of herbal ingredients in the appropriate ratios to achieve optimum therapeutic effect.
Transcriptomics can be used to elucidate target biomarkers and bioinformatics used to analyze or link biological events instigated by these herbs to predict their therapeutic potential. Pharmacogenomics and toxicogenomics involving metabolites from herbal medicines can facilitate interaction, thereby advising judicious and targeted use of the herbal medicines (Barlow et al., 2012; Bidon et al., 2009; Thomford et al., 2015) is key in “personalized herbal medicine” strategy.
The use of “-omics-” technologies can also serve in identifying potential drug candidates from herbal medicines through systems biology embedded target drug discovery (Vandamme et al., 2014), while stratifying target patients. “-omics-” technologies can help identify biomarkers of herbal medicines and disease targets, building an effective evidence-based basis for precision medicine, which will improve global health and provide new therapeutic options in combating the global epidemic of diseases like cancer, diabetes, HIV/AIDS, and hypertension. Focusing on personalized herbal medicine incorporated in precision medicine, and for an all-inclusive scholarly convergence on herbal biomarker R&D, innovative strategies that apply to conventional drug can be employed (Table 2).
PD, pharmacodynamics; PK, pharmacokinetics.
A look at the roadmap highlights the potential for herbal medicine to be developed to a level where there is standardization in all the processes leading to the final product for consumption, leading to effective treatment strategies to be at par with conventional medication. To ensure consistency, investments in medicinal herbal farms (biofarming) will ensure supply. There is an interconnection between conventional medication and herbal medicines for biomarker innovation. In addressing the global public health needs, there is the need to identify biomarker innovations through R&D. Multiomics platforms have presented prospects for herbal medicines.
It is becoming clear that herbal medicines cannot be continuously kept on the sidelines, but should be integrated into medical practice and training. We are calling for curricula review so that herbal medicine is given even recognition and time. If this is taken, we anticipate to produce a new type of a physician, who has an option to subspecialize in herbal medicine. Regulatory agencies should review the current models used for herbal medicine practice and utilization as therapeutic interventions.
Herbal medicines that exhibit effective therapeutic potential on diseases from an indigenous system should be assessed using similar or adapted platforms for conventional medications. Such herbal medicines should be developed to assess the benefit/risk balance, biomolecular extraction, and composition using multiomics platforms and appropriate clinical trials. The past few decades have observed the gradual convergence of legislations on medicines, leading to an improvement in the quality of medicines, including herbal medicines, and stringent regulatory requirements. Despite these regulatory mechanisms, specific innovative concepts for herbal medicines and conventional medications as part of the medical ecosystem should be applied for therapeutic interventions.
In the face of global health challenges, the convergence of herbal medicines with currently prescribed medications using multiplexed platforms will deliver effective therapeutic innovations. Conceivably, the positives of CHM practice pave way for biomarker innovations in herbal medicines as interventional strategies (Teschke et al., 2016; Wen et al., 2018; Xiao et al., 2017). Clinical trials of herbal medicines often flop statistically using the “conventional adaptive designs” because there are no binding rules to pick the most appropriate design for biomarker-related trials (Lin and He, 2015).
Biomarker-related trials on herbal medicines can help resolve such statistical issues and satisfy all regulatory requirements. The acceptance of “proposed biomarker-related trail designs” for herbal medicines and conventional medicines by regulatory agencies will motivate for biomarker innovations. The ultimate outcome of precision medicine practice is the well-being of the patient. Herbal medicine practice is becoming an everyday routine in modern medicine consciously or subconsciously. Most patients already exposed to herbal medicine seem to be deriving therapeutic benefits, which should be confirmed through clinical trials to generate unequivocal evidence.
Conclusions
It is imperative that as part of precision medicine, attention should be paid on the continuum of drug care integration (both conventional and herbal) with proper health records that capture the use of herbal medicine without prejudice or stigmatization for evaluation of benefits or risks, with respect to co-use of different therapeutic drugs. As part of revolutionizing precision medicine and incorporating “personalized herbal medicine” into medical practice, medical curricula should be open and have a place for interrogating herbal medicine to identify combinations or formulations that may assist in treating the 20% to 70% of patients on a spectrum of current conventional drugs, who are not effectively treated. Personalized herbal medicine is an unexploited ground which requires a systematic R&D approach to bring validation to the therapeutic efficacy of herbal medicine.
Scientific legitimacy utilizing the current technological revolution, using biomarker research for personalized herbal medicine, would be appropriate and critical for the scholarly convergence, achieving the precision medicine goal for most diseases in a holistic approach to benefit patients. This will also demand that issues related to the production and supply of herbal medicines are addressed for reasons to do with sustainability. In addition, the study of the conventional medicine/drug and herbal medicine research and clinical practice ecosystems under the newer and conceptually robust models of social analyses, such as “responsible innovation” frameworks, would lend itself to further effective guidance of these two bodies of highly intertwined and relevant knowledge (Fisher et al., 2015; Fisher, 2018; Guston, 2015; Sarewitz, 2015).
At this critical juncture when precision medicine initiatives are being rolled out worldwide, precision/personalized herbal medicine is both timely and essential for modern therapeutics, not to mention biomarker innovations that stand the test of real-life practices and implementation in the clinic and society.
Footnotes
Acknowledgment
This study was supported by the South African National Research Foundation (NRF) through the Indigenous Knowledge System (IKS) program. NET is also supported by the Faculty of Health Sciences, University of Cape Town, South Africa.
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.