
Abstract
Pharmacogenomics (PGx) education is crucial to support the effective delivery of PGx services in any health care system. We mapped the current educational environment of genomics and PGx in the United Arab Emirates (UAE) and assessed the readiness of the accredited higher education system to move forward with the implementation of PGx in the country. We employed a mixed-methods triangulated approach to map the PGx educational environment in UAE. We used two qualitative methods and one quantitative method. University curricula inspection, interviews, and questionnaires were the main resources of data. PGx was taught in 6 out of 21 accredited universities, but only for pharmacy majors. Only three out of six PGx courses were stand-alone. Majority of academia exhibited positive attitudes toward the availability and accessibility of genetic testing, with 89% agreeing that the government should invest more money into its development. Interviews with academics and, importantly, the commissioners who oversee the accreditation process of universities in UAE revealed recurrent themes that included recognizing the importance of genomic medicine and PGx and called for translational and implementational research, including recruitment of experts in the field. We recommend, as supported by our findings in this study, the creation of standardized curriculum of genomics and PGx for each health science field, using the blended teaching approach, and benchmarking internationally accredited universities to foster international collaboration and improve the education and practice of genomics in the clinic and public health systems. An 11-item genomics and PGx strategy is presented herein. Finally, the mixed-methods study design employed in this research may also serve as a model conceptual frame for other science education mapping efforts at country or multi-institutional scales in the future.
Introduction
Following the completion of The Human Genome Project in 2003, advances in genomics have propelled personalized medicine forward (Karas-Kuželički et al., 2019). Pharmacogenomics (PGx) combines the study of genomics and pharmacology in investigating the impact of acquired and inherited genetic variation on drug response (T P et al., 2009). It aims to minimize drug toxicity and improve drug efficacy and hence improve outcomes (Gurwitz et al., 2003; Gurwitz, 2010; Pisanu et al., 2014).
The slow clinical application of PGx is mainly attributed to lack of genomic knowledge among health care professionals (Pisanu et al., 2014). Therefore, PGx education is essential, especially for pharmacists, to support the delivery of PGx services (Talwar et al., 2019). Several studies demonstrate that, despite their belief in the importance of PGx in pharmacy, pharmacists and health care providers perceive themselves to have low confidence in their knowledge and application of PGx testing, indicating the need for extensive PGx education to optimally guide patients (Formea et al., 2013; Mccullough et al., 2011; Pisanu et al., 2014). In 2005,
The International Society of Pharmacogenomics (ISP) published recommendations directed to Deans of Education at medical, pharmaceutical, and health schools worldwide. It included a recommendation with an urgency to implement PGx in core pharmacology curricula (Gurwitz et al., 2005). Therefore, many studies conducted evaluations and assessments of PGx education using the ISP's recommendations as the reference point (Green et al., 2010; Higgs et al., 2008; Karas-Kuželički et al., 2019).
A survey used to assess pharmacist's educational exposure to PGx showed that 67.1% reported that PGx should be a focal point in school education, yet 80.1% reported that it was not an integral part of their education (Mccullough et al., 2011). A 2019 study among pharmacy students in Jordan and West Bank of Palestine indicated that 60.3% stated their PGx education was insufficient (Jarrar et al., 2019). Moreover, a study reported that among 206 pharmacists in Saudi Arabia, only 30% received formal training on PGx (Algahtani, 2020).
A survey completed in 2010 displayed that 74.4% of respondents in the U.S. and Canadian medical schools have incorporated PGx into the degree's curriculums, but still less than the 89.3% of U.S. pharmacy schools and the 84% of British medical schools (Green et al., 2010). Haga and Moaddeb (2019) reported that, while PGx was included in the pharmacy curricula of U.S. schools, less than 50% had a stand-alone course. Similarly, Basyouni and Shatnawi (2020) displayed that 85.7% of U.S. medical schools included PGx in their curricula but not as a stand-alone course.
A 2014 study concluded that PGx educational programs were not uniformly provided in Europe. It showed that Northern European countries such as the United Kingdom, Germany, and Netherlands's PGx education is more uniform when compared to South Eastern countries undergraduate and/or postgraduate studies where PGx is not at all included (Bosnia and Herzegovina, Cyprus, and Malta), included in some (Bulgaria, Albania, Croatia, Serbia, and Turkey), or extensively taught (Greece and Italy) (Pisanu et al., 2014).
We recognized the necessity to map the educational environment of genomics and PGx in the United Arab Emirates (UAE) in reaction to our assessment of the knowledge of both health care providers and health sciences students; both cohorts exhibited poor to fair knowledge of genomics and PGx (Rahma et al., 2020b, 2020c). Furthermore, we aim to assess the readiness and wiliness of the higher education system to move forward with the implementation of genomic medicine and PGx in UAE.
Materials and Methods
This study was approved by the Social Science Research Ethics Committee of United Arab Emirates University ERS_2017_5671. All participants read the information sheet of the study and signed the consent form before participating in the study.
We employed a mixed method triangulated approach to map the PGx educational environment in UAE. We used two qualitative methods and one quantitative method. The two qualitative approaches were interviews and content analysis of the educational curricula of different UAE universities. We interviewed and distributed a questionnaire among the university faculty members in accredited universities to get an in-depth understanding of their needs and vision of the future of genomics and PGx. Furthermore, we conducted interviews with higher education experts from the commission for academic accreditation (CAA) at the Ministry of Educations in UAE to close the loop and draw their attention to the current status of genomics teaching in UAE. In addition, we surveyed the academia teaching in medical and health sciences degrees in the accredited universities in UAE to assess their attitudes and to complement our curriculum mapping.
Qualitative 1
Mapping the genomics and PGx curricula in medical and health sciences degrees in the accredited universities in UAE
A qualitative approach was adopted to map the genomics and PGx curricula in medical and health sciences degrees at the accredited UAE universities. All universities were identified, private and public, through the UAE Ministry of Education. Universities that do not offer health sciences, medical or dental programs, were excluded. The university's latest syllabus and webpage were used as the main source of data collection. The keywords used were genetics, genomics, molecular genetics, pharmacogenetics, PGx, public health genomics, medical genomics, and molecular diagnostics.
Data were entered and coded in an excel sheet based on the name of the university, location, public or private status, degrees offered, name of the course, credit hours, and whether the course was stand-alone or integrated within another course. Course modules were grouped into 11 course categories: genetics, genomics, pharmacogenetics, PGx, molecular diagnostics, molecular biology, molecular biology techniques, genetic engineering, gene therapy, clinical genetics, and biotechnology.
Qualitative 2
Understanding of the current environment and the future directions of genomics and PGx educational environment in UAE
A total of four semistructured interviews were conducted; two with university faculties and two with commissioners in UAE. Commissioners were interviewed to close the loop because they oversee the accreditation process of universities in UAE. The interview guide was constructed and then reviewed by experts in the field of genomic medicine, public health, qualitative study, and epidemiology. All interviews were audio recorded and field notes were logged during and after the interview. Each semistructured interview took 40 to 60 min and was performed at participants' workplace. The interviews were transcribed in a verbatim manner. Grounded theory guided the independent extraction of the codes and themes by the two researchers (I.E. and A.T.R.). NVivo software version 12 was used for coding and theme extractions.
Quantitative
Assessing the current status of PGx teaching in medical and health science degrees in the accredited universities in UAE and the attitude of academia toward genomics implementation
A validated and piloted questionnaire (Supplementary Data) was used, which was based on validated and published questionnaires that were used to assess PGx in the curricula of colleges and schools of pharmacy in the United States as well as other published work (Murphy et al., 2010; Pisanu et al., 2014).
We piloted the questionnaire among public health and pharmacy faculty members and amended it accordingly. The questionnaire was randomly emailed by an identified focal person (dean, secretary identified from website of the colleges) to the academia teaching in medical and health science degrees in the accredited universities in UAE. The Statistical Package for the Social Sciences (IBM SPSS) was used to perform descriptive statistics on our data such as frequencies and means.
Results
Mapping of the university curricula
Out of the universities in all seven emirates comprising UAE, two were excluded as the degrees did not match criteria. The assessment of university curricula included a total of 21 universities.
Courses included after thorough keyword searching of all universities' curricula totaled to 368 credits. Genetics resulted in a total of 140 credits out of the 368 (38%). All genetics credits belonged to stand-alone courses, with the exception being in medical and dental degrees, where only 8 out of 35 genetics credits belonged to stand-alone courses. PGx and genomics courses accounted for 15 and 9 credits out of 368, respectively. Figure 1 displays the number of total credits per course category.
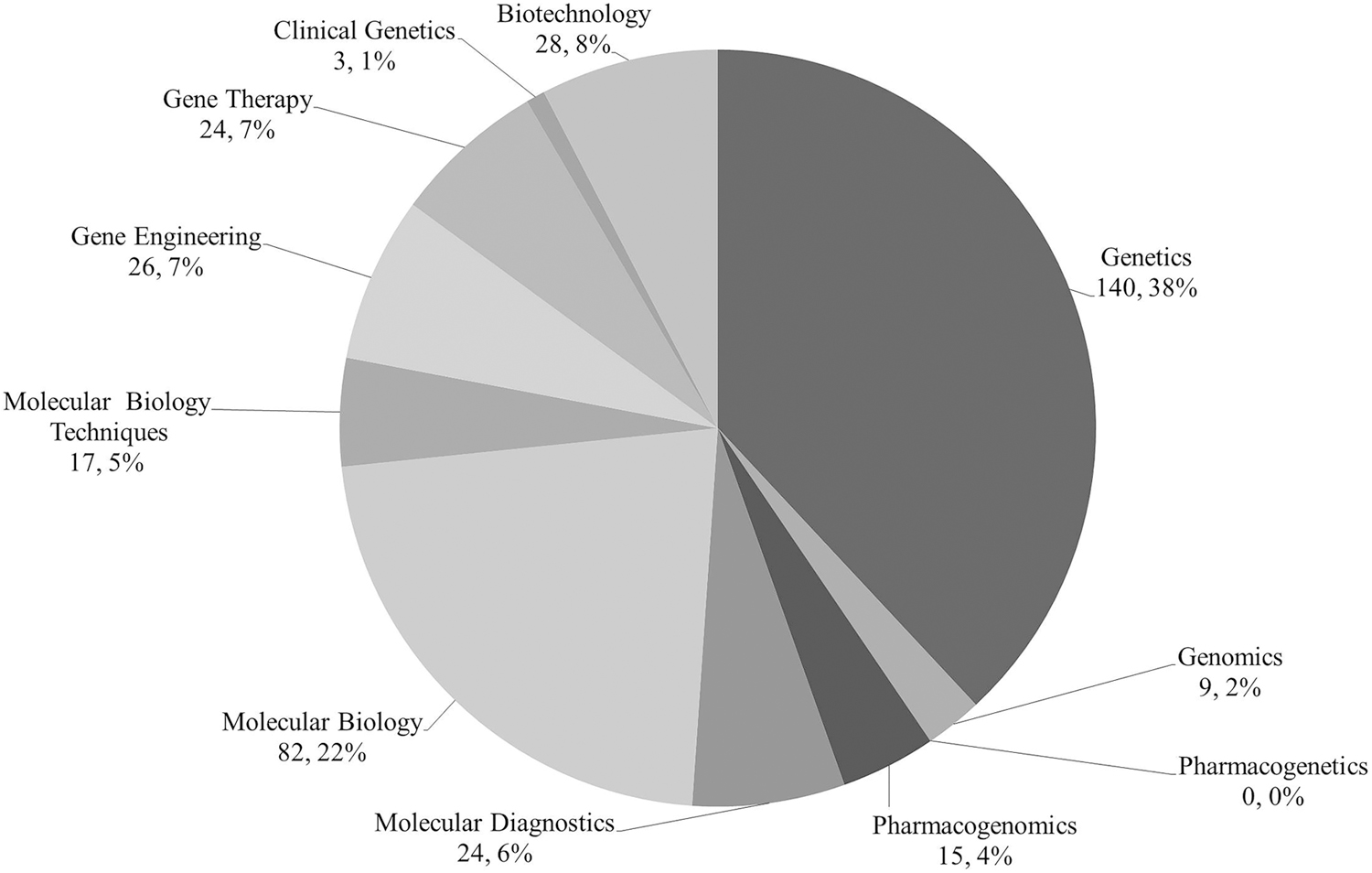
Total number of credits per course category (total credits = 368).
PGx was taught in the curriculum of six universities; however, it was only for Pharmacy majors. Only three out of the six PGx courses were stand-alone. When searching for “genomics,” five universities yielded results. None of the genomics courses was stand-alone. When the keyword “pharmacogenetics” was searched in all universities' curricula, no results were found. Figure 2 displays the results per level when “pharmacogenomics” and “genomics” were searched in the curricula.
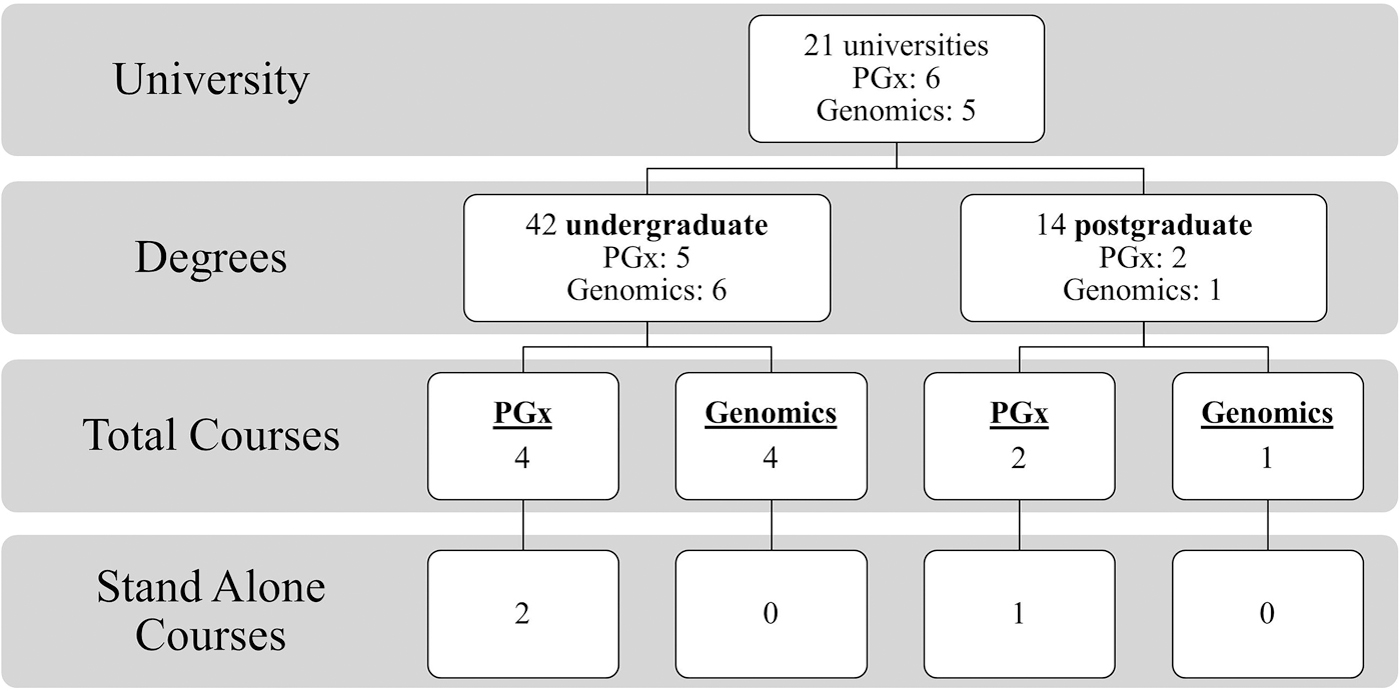
“Pharmacogenomics” and “genomics” search results by university, degree, and course level.
Findings of the semistructured interviews
The identified main themes coded inductively from the iterative analysis of the semistructured interviews with the teaching faculties in UAE, and the commissioners and higher education experts from the CAA are presented in Table 1. Below are the most relevant themes.
Identified Themes of Semistructured Interviews with the Teaching Faculties and the Commissioners and Higher Education Experts in the United Arab Emirates
UAE, United Arab Emirates.
(1) Recognizing the importance of genomic medicine and PGx to prepare the future healthcare providers for the personalized medicine era.
Interviewee 2: “I graduated from the xxx medical school, so all what we had then was basic molecular biology, so I went abroad to study, but when I came back to teach here, I found there are courses about genomic medicine and probably there is a lecture or two about pharmacogenomics.”
Interviewee 3: “I've visited college of pharmacy just last week and they have a new curriculum and in the curriculum there was a pharmacogenetics course and they told us that they added this based on international reviews, I think the international norms that there should be a pharmacogenetics course in pharmacy curriculum.”
Interviewee 4: “My personal experience of accreditation of medicine and pharmacy programs is that if pharmacogenomics is insufficient in these programs, external review teams normally do require that curricular content is added. This can be either as separate courses but often better integrated into other courses.”
(2) Calling for translational and implementational research along with recruiting experts in the field.
Interviewee 1: “I think the main barriers is ignorance, I would say ignorance on many levels, you know from healthcare workers who don't know much about genomic medicine, misconception in the community sometimes. Obviously, the decision makers again they don't have the full picture also studies or solid studies to implement genomic medicine into healthcare systems more effectively.”
Interviewee 4: “I agree that many pharmacy colleges in UAE do not have faculty with much expertise in pharmacogenomics. This can be addressed through faculty development and through use of visiting lecturers who do have the relevant expertise.”
Academia survey assessment
Respondents affiliated with the colleges of medicine constituted 70% of the sample, and 13.8% from pharmacy or pharmacology. Respondents were 51.2% male with all ages ranging between 28 and 70, with a mean age of 44.
When asked on the current state of PGx teaching in most universities and schools in UAE, 36.2% of the sample considered it to be poor and 39.1% indicated that they do not know. According to the survey, only 34.3% of participants indicated that PGx coursework was being taught within their curriculum. Respondents pointed out that 39.1% PGx coursework was taught at a master's level in their institution. Only 26.1% stated it was a stand-alone required didactic course. Majority of respondents (81%) estimated 1–2 credit hours are dedicated to PGx in their curriculum (Table 2). The top 3 topic areas currently covered in respondents' PGx education are shown in Table 3.
Pharmacogenomics/Pharmacogenetics Coursework Information in Respondents' Universities
PGx, pharmacogenomics.
Topics Covered in Respondents' PGx/Pharmacogenetics Curricula (n = 23)
Majority of respondents exhibited positive attitudes toward the availability and accessibility of genetic testing, with 89% agreeing that the government should invest more money into its development. However, 74% agreed that the availability of genetic tests could be problematic for insurance companies and future employers. Figure 3 displays the results of the questions on genetic testing.
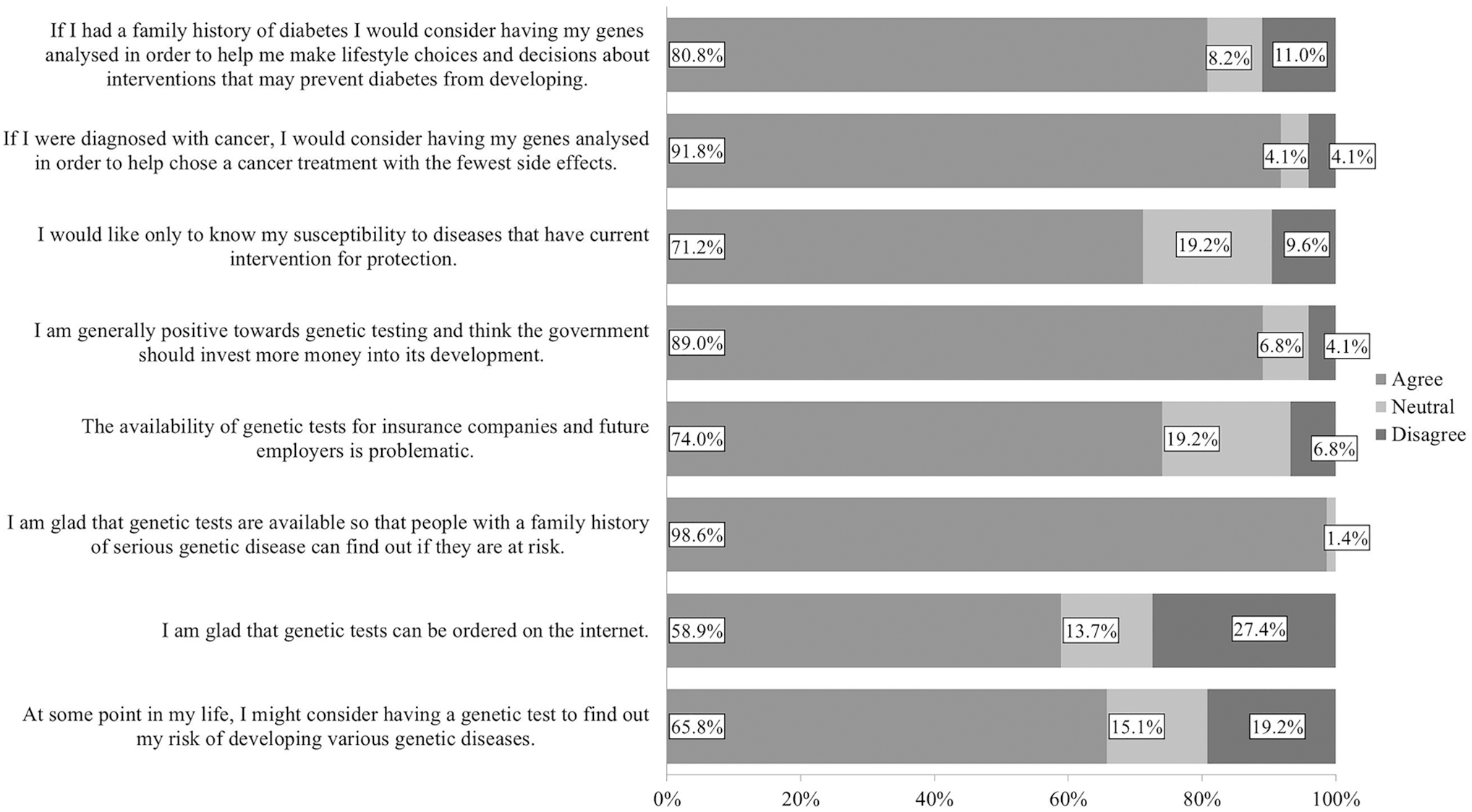
Views on genetic testing (n = 73).
Respondents had a positive outlook on the future of personalized medicine and PGx (91.8%), with 82.2% agreeing that more course study time should be devoted to the teaching of PGx. However, 69.9% believed insurance companies and employers could exploit PGx. Confidentiality did not seem to be a top concern with only 35.6% unwilling to get their genome analyzed due to confidentiality issues. When asked if they would prefer a physician or pharmacist to explain their genome report, 83.6% preferred a physician. Respondents' views on the concerns and outlook on the future are shown in Figure 4.
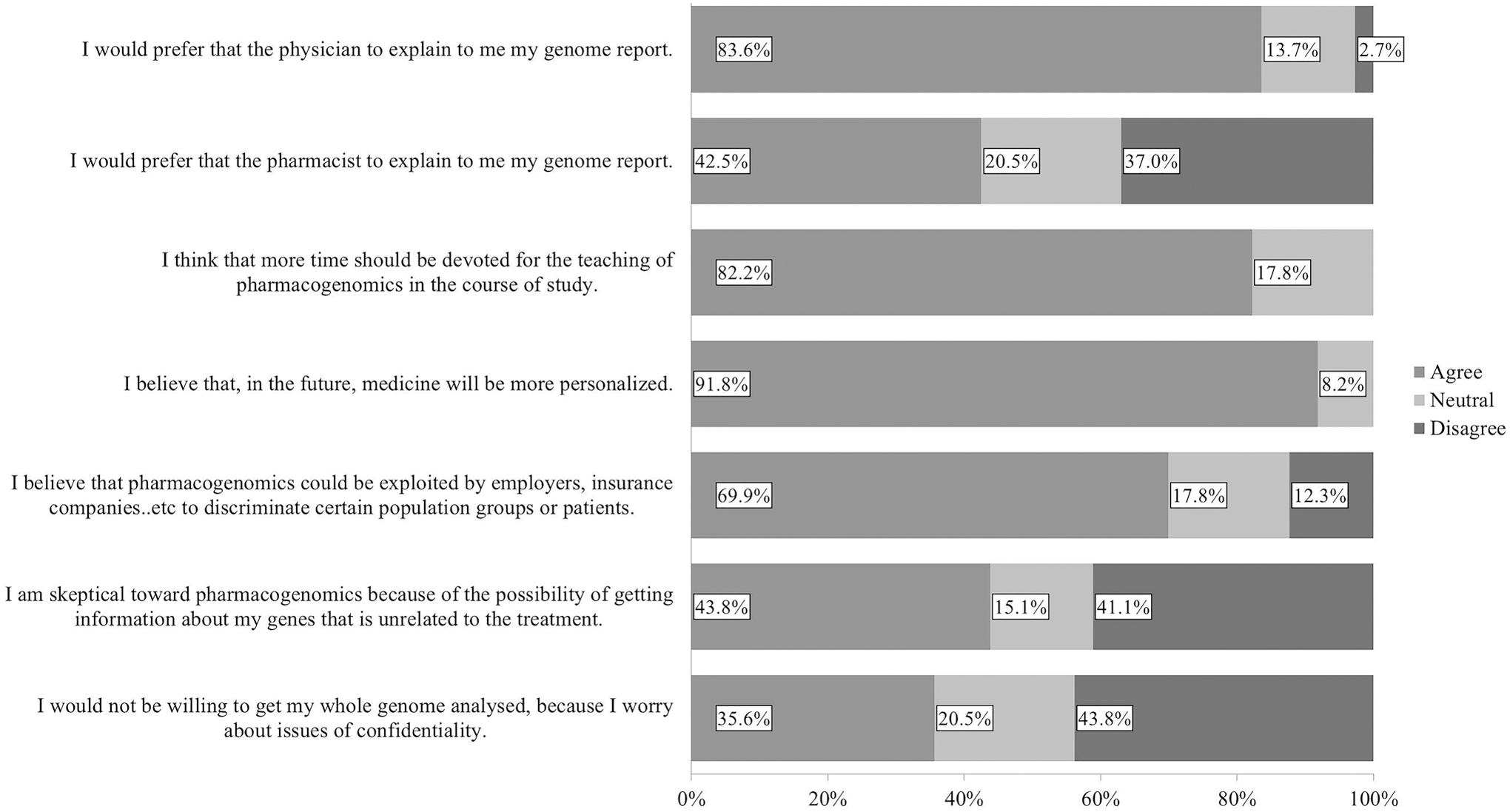
Concerns and outlook on the future of PGx (n = 73). PGx, pharmacogenomics.
Respondents exhibited positive attitudes when questioned on their desire to participate in genetic research, with 76.7% agreeing to participate and 74% interested in attending a PGx course and/or educational seminar. When asked on their preferred method to learning PGx, 56.3% chose workshops or seminars. Moreover, 63% agreed to donate genetic materials to a bio bank.
Respondents identified the top 3 barriers for PGx implementation to be lack of training or education (67.6%), lack of clinical guidelines on PGx/pharmacogenetics practice (64.8%), and lack of testing services and shortage of personnel (52.1% each).
Discussion
In this study, we present a large-scale and multi-institutional map of the current state of genomics and PGx education in UAE, and using a state of the mixed-methods study design. We did not limit ourselves to specific field of genomics to allow broader mapping of the current educational environment. This served as a baseline for other researchers as well as a point of comparison for the stakeholders. We employed both qualitative and quantitative methods to create comprehensive data and insights.
Breadth of studies attributed the poor knowledge of health care providers toward genomics and PGx to the dearth of official tutoring in the universities and recommended incorporating genomics and PGx in the curriculum (Chair et al., 2019; Rahma et al., 2020b, 2020c; Sharoff, 2019; Stark et al., 2019; Whitley et al., 2020). The mapping of the medical and health sciences curriculum of the accredited universities in UAE pointed out that basic genetics is included in the majority of universities' syllabi, both undergraduate and postgraduate; however, PGx and human genetics deviated from this inclusion. Even the curriculum was not standardized among universities nor covering topics in the same significance.
The survey and the interviews of the academia disclosed that regulatory aspects and clinical resources had less weight in the curriculum of PGx. A global survey conducted in 2016–2017 about PGx tutoring in medical and pharmacy colleges in Europe, Asia, Africa, North America, South America, Australia, and Oceania disclosed that 13.4% had no PGx education (Karas-Kuželički et al., 2019). On the contrary, our mapping revealed that PGx was taught in the curriculum of only six universities for Pharmacy majors. Only three out of the six PGx courses were stand-alone.
The ISP in 2005 called for integrating at least 3–4 teaching hours of PGx in the curriculum for all medical, pharmacy, and health schools; however, 81% of the academia in our cohort estimate the number of required credit hours dedicated to PGx/pharmacogenetics in the curriculum to be 1–2 hours (Gurwitz et al., 2005). This shortcoming in relation to the ISP recommendations will impact the implementation of PGx in UAE as expressed in our study about the knowledge of both health care providers and students in UAE (Rahma et al., 2020b, 2020c). In our study of assessment of the knowledge of medical and health science students in UAE toward genomic medicine and PGx, we reported that only 4.2% responded correctly to all the knowledge questions and that can be attributed to the scarce coverage of genomics in the curriculum of the accredited universities in UAE (Rahma et al., 2020c).
Academia in UAE stated that PGx/pharmacogenetics coursework is being taught mainly at master academic level (39.1%). However, this finding is not in line with what is reported globally. Study by Murphy et al. (2010) cataloged teaching PGx mostly in the undergraduate level, PharmD, or PhD level (Murphy et al., 2010). In the same track of comparing the results of the survey of the academia of the U.S. colleges by Murphy et al. (2010) and the academia in UAE in 2020 (we used the same questionnaire), we report that 92% of the surveyed colleges in the United States teach PGx vs. 34.3% in UAE. Moreover, 72.5% of the colleges in the United States included PGx as part of other required didactic course(s) versus 56.5% in UAE. Furthermore, 21.7% of colleges in the United States require specific prerequisite courses for PGx versus 33.3% in UAE (Murphy et al., 2010). Despite the 10-year gap, UAE is lagging in adopting PGx in the curriculum of its colleges.
The academia divulged that the use of information technology to obtain credible, current information about pharmacogenetics has covered only 34.8% in the curriculum. This is a red flag. It is crucial to equip the future adopters of the science of PGx and genomics with the necessary skills to acquire reliable information (Cheng, 2003; Rahma et al., 2020a).
The ethical, legal, and social topics linked to pharmacogenetics/genetics had been covered in only 52.2% of the topics in the curriculum; that gap can explain why these aspects were cited by health care providers and students in UAE as one of the main barriers for implementation of personalized medicine in UAE (Rahma et al., 2020b, 2020c).
The commissioners and higher education experts at the CAA at the Ministry of Education in UAE ascribed this gap to the shortage of the experts in the field of genomics and PGx in UAE, as well as the paucity of partnership with the specialists. A study by Shaffer et al. (2010) advocated the genomics education partnership and concluded that it was fulfilling for both students and faculty. This was also highlighted by Perkmann and Schildt (2015) in their review of the structural Genomics Consortium case study as well as in LeBlanc and Dyer (2003) in their 3-year case study.
A positive attitude was detected among academia and commissioners toward harnessing genomics and PGx to prepare the future health care providers to the personalized medicine era. The majority (82.2%) agreed that more room should be allocated in the curriculum for genomics and PGx, and 74% were interested in attending PGx courses or seminars. These results are in consonance with the international educational strategies (Adams et al., 2016; Burgess et al., 2016; Frick et al., 2018; Gálvez-Peralta et al., 2018; Guy et al., 2020; Karas-Kuželički et al., 2019; Perry et al., 2016; Weitzel et al., 2016).
Furthermore, we contextualized the personal attitude of the academia and commissioners toward conducting genetic tests and participating in genetic research and biobank, as we hypothesized that such positive attitude would influence the pace of imputing of genomics in the curriculum. This area has not been thoroughly investigated in the literature and warrants further research.
Academia and education commissioners shared an optimistic view of the future. They captured the strides that map the implementation of genomic medicine and PGx in UAE. The profound strategy is education. This finding is in line with literatures and recommendations of international societies like the ISP and The International Society of Nurses in Genetics (ISONG) (Beamer and Rosinski, 2019; Gurwitz et al., 2003, 2005; Hickey et al., 2018; Karas-Kuželički et al., 2019; Lesko and Johnson, 2012; Ziegelstein, 2015).
In the systematic review by Talwar et al. (2019), they analyzed the current genomics courses offered to health professional students and concluded that the field of genomics education incubates evolving pedagogical methods like self-genotyping, which can be adopted by the academia in UAE.
The strength of our study is the complementary mixed-methods approach that countenances a comprehensive assessment and mapping of the educational environment of genomics in UAE. In addition, the triangulation with our study about the assessment of knowledge of medical and health sciences students allows attribution and postulation. Furthermore, assessing the attitude of the academia is a novelty that fosters the implementation strategies. Including the commissioners and higher education experts at the CAA at the Ministry of Education delineated the stakeholders stand and fostered a top-up viewpoint.
The limitations of our study include the inherent bias of both quantitative and qualitative methods involving lack of generalization, selection, or information bias. To mitigate these biases, we employed random sampling and disseminated the questionnaires to all the accredited health sciences universities in UAE. The snapshot feature of our study is another limitation that can be considered a baseline that fosters further research for comparison and analysis. We did not dive deep in to the type of PGx biomarkers that are covered in the curriculum or if there is an integration of PGx with other omics fields or the educational tools utilized. Therefore, we urge future researchers to factor these limitations in their mapping.
Outlook and Conclusions
We recommend the following 11 strategies for development and implementation:
A standardized curriculum of genomics and PGx for each health science fields (medicine, pharmacy, nursing, dental, pathology etc.). A blended teaching approach to recruit experts in the field that can teach courses online as well. Benchmarking with the international universities and organizations for collaboration and accreditations. Blending the laboratory components in the curriculum as literatures prove it efficient. Including the ethical, legal, and critical governance aspects of genomics and PGx in the curriculum. Adopting “train the trainer” strategy. Embarking on the basics of genomics and PGx in elementary schools using innovative pedagogy. Fostering the collaboration between academia and health care setting to produce research and databases. Spanning the residency and fellowship opportunities to include genomics, PGx, bioinformatics, and genetic counseling. Mandating the stand-alone courses of genomics and PGx in the curriculum for both undergraduates and postgraduates. Establishing national accreditation council to train, educate, and license health care providers based on competencies.
Mapping the educational environment of genomics and PGx in UAE is in a heuristic stage, which will, however, galvanize the implementation trajectory and strategies. The positive attitude along with the interest of the stakeholders in academia will is a well-aimed target in the pursuit of implementation. Finally, the mixed-methods study design employed in this research may also serve as a model conceptual frame for other science education mapping efforts at country or multi-institutional scales in the future.
Footnotes
Authors' Contributions
F.A.M., A.T.R., I.E., L.A.A., B.R.A., and G.P.P. conceived and designed the study. A.T.R. and M.A.K. collected data. A.T.R. and M.E. analyzed the data. A.T.R. and M.E. drafted the article. F.A.M., L.A.A., B.R.A., G.P.P. and I.E. reviewed the analysis and the interpretation. All authors made a significant intellectual contribution to the article contents and have agreed to the final version of the article.
Acknowledgments
The authors would like to thank and acknowledge the academics, commissioners, and all participants who agreed to take part in this study.
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
This study is supported by a grant from Zayed Center for Health Sciences, United Arab Emirates University, Fund code 31R175. The sponsor has no roles in study execution, the preparation and analysis of data, or the article.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.