
Abstract
The coronavirus disease 2019 (COVID-19) pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus is anticipated to transition to an endemic state as vaccines are providing relief in some, but not all, countries. Drug discovery for COVID-19 can offer another tool in the fight against the pandemic. Additionally, COVID-19 impacts multiple organs that call for a systems medicine approach to planetary health and therapeutics innovation. In this context, innovation for drugs that prevent and treat COVID-19 is timely and much needed. As the virus variants emerge under different ecological conditions and contexts in the long haul, a broad array of vaccine and drug options will be necessary. This expert review article argues for a need to expand the COVID-19 interventions, including and beyond vaccines, to stimulate discovery and development of novel medicines against SARS-CoV-2 infection. The Renin–Angiotensin–Aldosterone System (RAAS) is known to play a major role in SARS-CoV-2 infection. Neprilysin (NEP) and angiotensin-converting enzyme (ACE) have emerged as the pharmaceutical targets of interest in the search for therapeutic interventions against COVID-19. While the NEP/ACE inhibitors offer promise for repurposing against COVID-19, they may display a multitude of effects in different organ systems, some beneficial, and others adverse, in modulating the inflammation responses in the course of COVID-19. This expert review offers an analysis and discussion to deepen our present understanding of the pathophysiological function of neprilysin in multiple organs, and the possible effects of NEP inhibitor-induced inflammatory responses in COVID-19-infected patients.
Introduction
While new vaccines are being made available to prevent coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus, the pandemic is far from being over. A broad armamentarium of vaccines and drugs to prevent the disease will be necessary in the long haul. The Renin–Angiotensin–Aldosterone System (RAAS) and SARS-CoV-2 axis plays a crucial role in the development of COVID-19 disease. Neprilysin (NEP) and angiotensin-converting enzyme (ACE) have emerged as targets of interest in therapeutics innovation to stem the COVID-19 pandemic and for its long-term management as the pandemic evolves to an endemic infection.
This expert review aims to deepen the present state of insights on the pathophysiological function of NEP in multiple organs. This review also strengthens our understanding of the possible effects of NEP inhibitor-induced inflammatory reactions in COVID-19-infected patients.
COVID-19 as a Multiorgan Disease to Benefit from a Systems Medicine Perspective
The World Health Organization (WHO) announced COVID-19 disease as a pandemic in March 2020. This deadly infectious disease caused by a single-stranded RNA virus known as the SARS-CoV-2 virus (Chan et al., 2020) packed into a 70–90 nm particle and encoding for 29 proteins (Khailany et al., 2020) has brought the entire world to a halt causing unbelievable mortality, morbidity, and substantial economic damage. The medical symptoms of COVID-19 infection vary remarkably from person to person and from asymptomatic form to acute bilateral pneumonia. SARS-CoV-2 infection activates hyperinflammation and multiorgan failures in humans resulting in COVID-19-associated deaths. Although several repurposed drugs may aid recovery and treatment in intensive care COVID-19 patients, the corresponding clinical trials did not indicate whether it can.
The SARS-CoV-2 infection affects several organs in humans. The primary target of the viral infection is the lungs; however, the heart, brain, intestine, liver, and kidney are also affected by this virus (Balachandar et al., 2020; Jain, 2020). Multiorgan failure is a severe life-threatening condition witnessed in COVID-19 patients. This condition is due to the hyperactivation of several proinflammatory cytokines, such as Interleukin-1β, Interleukin-6, granulocyte-macrophage colony-stimulating factor (GM-CSF), and tumor necrosis factor-alpha (TNF-α) (Arabi et al., 2021; Costela-Ruiz et al., 2020).
These inflammatory cytokines have been reported to highly express between 7 and 20 days of infection in patients suffering from COVID-19 (Guo et al., 2020; Huang et al., 2020; Mehta et al., 2020a; Shi et al., 2020; Zhou et al., 2020). Hyperexpression of inflammatory reactions was involved in causing COVID-19 pneumonia, acute respiratory distress syndrome (ARDS), and acute heart failure (Guo et al., 2020; Huang et al., 2020; Shi et al., 2020; Zhou et al., 2020). The recurrence of the cytokine storm may be a major reason for these cardiac injuries and leads to mortality in COVID-19 patients. The antiviral and supportive therapies employed may not be sufficient to treat the mentioned complications in the current situation.
The current focus is on treating cytokine storms by repurposing several FDA-approved drugs. However, in such situations where there is an activation of hyperinflammation and cytokine storm with multiorgan failure, targeting the RAAS pathway with promising anti-inflammatory targets will be therapeutically relevant in the COVID-19 era.
SARS-CoV-2-RAAS-Mediated Signaling Pathway
RAAS signaling pathway consists of enzymes, peptides, and receptors, which are important in the regulation of signal transduction pathways in disease (Gheblawi et al., 2020; Simanshu et al., 2017). It also serves as a central target and entry point for the SARS-CoV-2 virus in the host cell. RAAS plays a vital signaling component in the body fluid balancing mechanism, and when activated, it brings about vasoconstriction, high blood pressure, enhanced aldosterone levels, and cardiac tissue remodeling (Ferrao et al., 2014). In a classical RAAS pathway, reduced renal blood flow leads to increased renin expression in the kidney. This renin in the kidney cleaves the liver angiotensin (Ang) to angiotensin I (Ang I). The Ang I to angiotensin II (Ang II) conversion is taking place in the lungs with the help of ACE (Gao et al., 2005).
In general, the viral entry mechanism is receptor-mediated endocytosis (Gao et al., 2005). In COVID-19 infection, the spike (S) protein from the virus binds to the receptors present in the host's cell membrane and initiates viral replication in the cell. The S protein is made up of two functional subunit domains known as a bulb (S1) and stalk (S2). S1 binds to the ACE2 receptor during the viral infection, and S2 involves binding with the membrane process (Yang et al., 2020; Yi et al., 2020). The binding of S1 with its associated receptor leads to structural changes in S2. These conformational changes lead to the attachment of viral envelope with the cell membrane of the host cell and subsequent release of viral nucleocapsid into the host cell cytoplasm (Belouzard et al., 2012).
During this virus/host binding event, the S1 subunit of the viral spike protein fused with the host ACE2 receptor by its binding domain. Subsequently, this binding leads to an increase in Ang II production. However, it leads to downregulation of ACE2 and Ang 1–7, which functions as a vasodilator (Acanfora et al., 2020a; Shang et al., 2020) and thus contributes to the hyperinflammatory consequences of COVID-19.
In humans, host cell sensitivity is related to the amount of ACE2 receptors expressed in the host. ACE2 expression is mainly found in the heart, and vascular and renal systems (Gheblawi et al., 2020). ACE2 expressions are also reported in various organs, including the liver, eye, intestines, central nervous system (CNS), upper airway, and lung epithelial cells (Gheblawi et al., 2020). ACE2 overexpression is known to mitigate lung damage and pulmonary fibrosis by activating the ACE2/Ang-(1–7)/MAS axis, which boosts the synthesis of Ang (1–7). The Ang (1–7) neutralizes the action of the ACE/Ang II/Angiotensin II type 1 receptor (AT1R) axis in the lung (Li et al., 2016; Meng et al., 2014) (Fig. 1). In this context, the renin–angiotensin system (RAS) inhibitors, especially AT1R-neprilysin inhibitors (ARNIs) are in the spotlight as chronic therapy as angiotensin-II-receptor antagonists (sartans) may lessen lung tissue damage in COVID-19 patients.
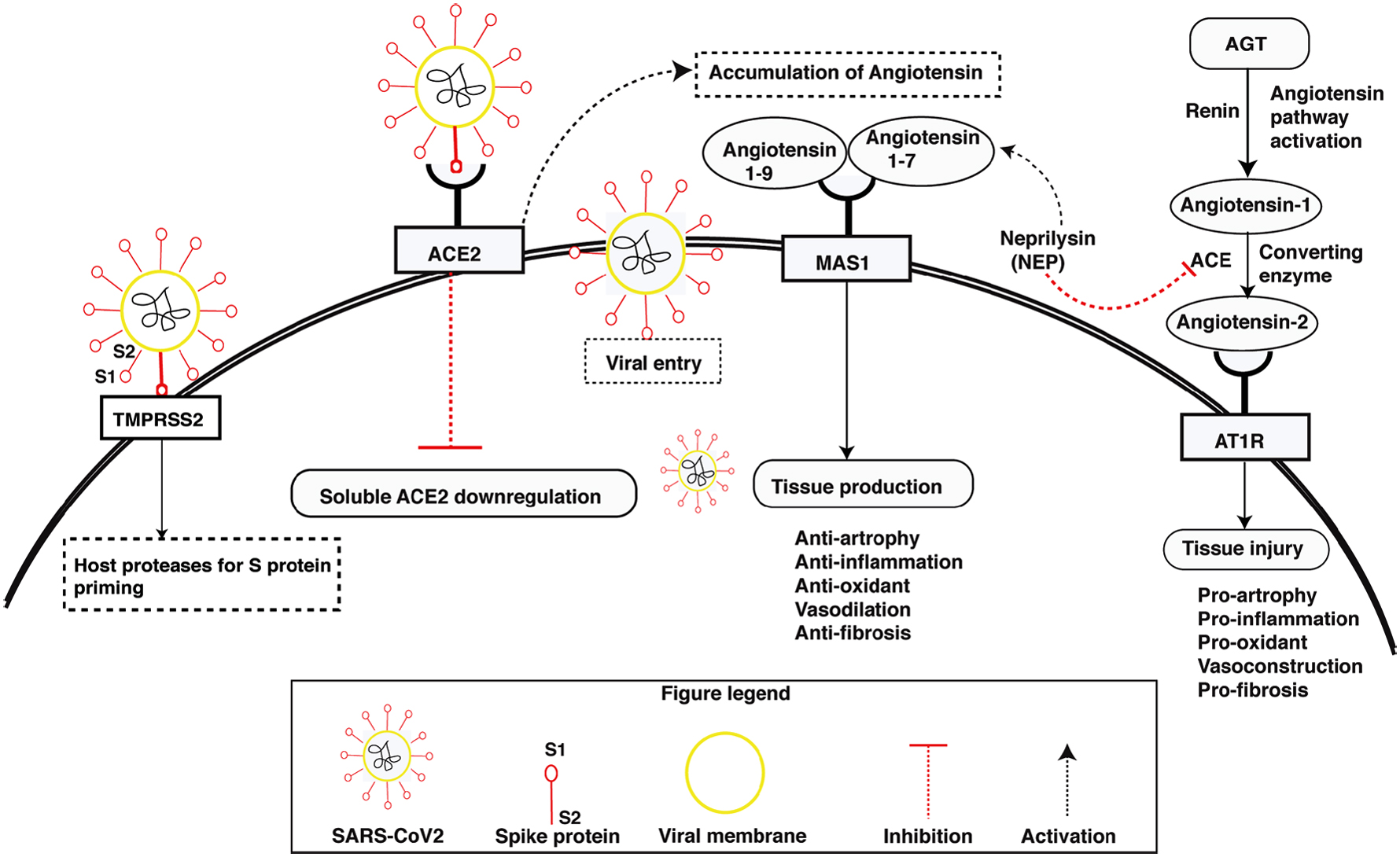
Molecular interactions between the SARS-CoV-2 viral protein and the ACE2 receptor during viral entry into host cells: The large subunit of viral S protein, primed by TMPRSS2, binds to ACE2 receptor in viral entry into host cells. ACE2 plays a critical role in preventing lung damage and attenuating pulmonary fibrosis by enhancing the ACE2/Ang (1–7)/MAS axis to increase Ang (1–7) production. ACE, angiotensin-converting enzyme; Ang, angiotensin; S protein, spike protein.
Targeting the RAAS Pathway
The scientific community worldwide is trying to decipher this pathogen's pathophysiology and the disease-related signaling networks. Recent reports have shown that the classical RAAS pathway is a key player in COVID-19 pathogenesis (Busse et al., 2020). RAAS system is involved in acute lung damage, and ACE2 is reported protective in acute lung failure (Kuba et al., 2006).
In the RAS pathway, Ang I is reduced to Ang II by ACE. This Ang II subsequently binds to the AT1R receptor. The binding of Ang II to AT1R receptors leads to increased COVID-19 disease-driven lung failure that can be mitigated by the repurposing of available inhibitors such as Ang II receptor blocker (ARB) and NEPi, commonly known as the angiotensin receptor neprilysin inhibitors (ARNIs). The ARNIs have been proposed as potential therapeutics for modulating the COVID-19 pandemic (Acanfora et al., 2020a; El Tabaa and El Tabaa, 2020; Zolfaghari Emameh et al., 2020). An FDA-approved ARNI; Entresto (Navartis), which is a combination of a NEPi (Sacubitril) and an Ang II receptor blocker (valsartan) is helpful to treat various heart problems (McMurray et al., 2014; Sauer et al., 2019). Recent reports proposed that this drug can be repurposed to treat COVID-19 (Acanfora et al., 2020a, 2020b; Gurwitz, 2020; Sankhe et al., 2021).
At the same time, other inhibitors such as ARB and ACE inhibitors are also hypothesized to be beneficial for COVID-19 patients as these inhibitors cause upregulation of ACE2 while blocking AT1R (Sun et al., 2020). NEP inhibitor therapy functions to rescue endogenous atrial natriuretic peptides (ANP), which function antagonistically to the RAAS (von Lueder et al., 2013), thereby obtaining potential therapeutic benefits by increasing natriuretic peptide (NP) levels and exert a protective effect on heart failure. Sacubitril/valsartan combination was reported to increase lymphocyte count and reduce the concentration of proinflammatory cytokines and neutrophils more than valsartan alone (Zhang et al., 2019).
Although sacubitril/valsartan has a promising role in the management of COVID-19, it is also conductive of several adverse consequences that are also present due to NEP inhibition. NEP inhibition is linked with angioedema, bronchial reactivity, and inflammation in animal models and human genetic studies (Campbell, 2017). The unwanted effects of (ARNIs) may be due to the accumulation of inflammatory peptides such as bradykinin and substance P (SP), which are canonical substrates for NEP (Campbell, 2018; Marcelino-Rodriguez et al., 2019).
The focus of the present review is to bring up the flip side of the NEP inhibitor's implications in the COVID-19 treatment regime and its possible systemic consequences, including multiple organ failures in probable high-risk group of patients.
Neprilysin and Its Physiological Role
NEP (EC 3.4.24.11) is the first reported endopeptidase in the renal tubule microvilli of rabbits in 1973 (George and Kenny, 1973; Kerr and Kenny, 1974). NEP is a 742 amino acid single-chain zinc metalloprotease, and it is a type II integral plasma membrane protein. The enzyme cleaves peptide bonds in various peptides with a preference for phenylalanine (F), leucine (L), and methionine (M) (Skidgel et al., 2004). NEP was previously known by several other names, such as common acute lymphoblastic leukemia antigen (CALLA), neutral endopeptidase, endoprotease, and neutrophil antigen cluster differentiation antigen 10 (CD10) (Bayes-Genis et al., 2015; Letarte et al., 1988; Shipp et al., 1991). NEP works on various peptide-based hormones by either cleaving them into inactive or transforming them into active agents.
Ang II, ANP, and others are NEP substrates involved in inflammation (bronchodilation) (Stephenson and Kenny, 1987). Other endogenous peptides degraded by NEP include Ang I (Erdos and Skidgel, 1990; Gafford et al., 1983), brain NP (Vogt-Schaden et al., 1989), chemotactic peptide formyl-Met-Leu-Phe (Connelly et al., 1985), α-neoendorphin, β-neoendorphin, dynorphin 1-9, gastrin, somatostatin, insulin P-chain, luteinizing hormone-releasing hormone (LH-RH), gonadotropin-releasing hormone (GHRH), oxytocin, and sarafotoxins (Koehne et al., 1998). To emphasize the significance of NEP in health and various diseases, we reviewed the myriad of physiological roles played by NEP in various major organs, including the heart, kidney, lung, and nervous system.
A subset of COVID-19 patients could experience a condition called “cytokine storm syndrome” typified by an uncontrollable, lethal hypercytokinemia together with multiorgan failure, and it seems to be a principal source of fatalities in COVID-19 (Mehta et al., 2020a; Wu and Yang, 2020). In addition to cardiovascular problems, earlier reports indicate that a COVID-19 infection may initially show neurologic symptoms before respiratory problems occur. COVID-19 may affect the entire nervous system. MRI reports show that COVID-19 patients have neurological involvement with encephalopathy symptoms, such as increased leptomeningeal spaces, bilateral frontotemporal hypoperfusion, and vascular permeabilization in the brain (Helms et al., 2020).
Nearly half of the patients hospitalized due to COVID-19 have a frequent neurological incidence of giddiness, headache, an impaired sense of taste and smell (Ahmad and Rathore, 2020). Recently, a report from China shows that nearly 4.9% of confirmed COVID-19 cases are associated with gastrointestinal symptoms (Ai et al., 2020). A recent US Inner City Hospital System reported acute kidney injury caused by direct infection with COVID-19 (Pelayo et al., 2020).
NEP and Physiological Roles in Heart
NEP is crucial in managing the cardiovascular system, as it acts on numerous vasoactive peptides, such as Ang I and II, NP, and bradykinin (Bayes-Genis et al., 2016b). NEP shows a varying degree of affinities toward its substrates (Erdos and Skidgel, 1989) and, under basal conditions, maintain a low concentration of its substrates in the extracellular milieu.
In the early 1990s, NEPI monotherapy gained popularity for its potential in heart failure treatment as it displayed promising preliminary hemodynamic parameters. However, one of the NEPIs, ecadotril, accompanied higher mortality and no clear efficacy than its placebo, which led to discontinuation of the trials on NEPIs for heart failure treatment (Bayes-Genis et al., 2016b; Cleland and Swedberg, 1998). NEPIs disappeared for about 20 years but reappeared in 2014 as a combination inhibitor along with ARBs for heart failure treatment. The NEPI and ARB inhibitors were introduced as an outcome of the PARADIGM-HF trial (Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure Trial) that exhibited the finer effect of NEPI inhibitors over enalapril in heart failure patients (Bayes-Genis et al., 2016b; McMurray et al., 2014).
Besides, NEP/ACE inhibition, neprilysin/renin inhibition systems have also been explored for the intervention of heart disease. Both the systems were reported to have shown comparable remediating effects on neurohumoral changes resulting from heart failure in rats (Ohtsuki et al., 1984). A recent report proposed that circulating soluble neprilysin (sNEP) is a presumed prognostic biomarker in chronic and acutely decompensated heart failure (Williamson and Ehrman, 1968); however, the implication of sNEP is still in its infancy, which would require further refinement.
Lung
In the lungs, NEP expresses in the undifferentiated epithelium in bronchial tissue in developing airways, airway sensory nerves, submucosal gland cells, and airway smooth muscle cells (Baraniuk et al., 1995; Sunday et al., 1992). In the lungs, NEP has a crucial function in the regulation of airway homeostasis by balancing multiple pulmonary short peptides such as SP and endothelin-1 (Erdos and Skidgel, 1987). It is reported to play different roles in lung development stages in a cell type-dependent manner (Stimler-Gerard, 1987). Respiratory irritants such as allergens, cigarette smoke, and NEP inhibitors, including phosphoramidon, have been reported to downregulate NEP levels in the lung, leading to neurogenic inflammatory manifestations, bronchial asthma, and chronic obstructive pulmonary disease (Wick et al., 2011; Wong et al., 2011).
NEP inactivates SP, which constricts the airway smooth muscles, causing excessive microvascular permeability, edema, and severe hypoxia. Inhibition of NEP activity was most likely the cause of hyperresponsiveness of the bronchial smooth muscle to SP (Sheppard et al., 1988). Another lung peptide modulated by NEP is the bombesin-like peptides (BLP), which are overexpressed in fetal lungs and likely to participate in the normal growth of the lung (Sunday et al., 1992). NEP plays a pivotal role in chronic hypoxic pulmonary hypertension by guarding the lung and preventing vascular remodeling due to hypoxia, most likely by restricting the proliferative and contractile effects of neuropeptides (Dempsey et al., 2009).
Many viruses, such as the influenza virus and Sendai viruses, are known to inhibit NEP activity and enhance neurogenic inflammatory response (Jacoby et al., 1988; Piedimonte et al., 1990). Thus, respiratory tract viral infections are an additional risk factor for asthma patients (Erdos and Skidgel, 1989). In COVID-19 patients, an estimated 40% mortality rate is due to ARDS. The pathogenesis of ARDS consists of inflammatory damages to the capillary membrane of the alveolar region (ACD), increasing pulmonary membrane permeability, and edema fluid infiltration into the surrounding airspaces. All these lead to the development of a compromised respiratory function (Bhatia et al., 2012). Thus, ARDS could be seen as a vital sign of immune system-mediated clinical consequences of COVID-19 infection (Guan et al., 2020; Xu et al., 2020).
Kidney
NEP is most abundantly expressed in the kidney and accounts for around 4% of total protein found in the membrane of the renal system (Fisk et al., 2007; Sankhe et al., 2020) and helps in maintaining kidney health in the homeostatic range. In contrast to the beneficial effect seen in the heart, NEP harms the kidney because it degrades beneficial NP such as ANP, B-type natriuretic peptide (BNP), and c-type natriuretic peptide (CNP). For example, ANP normalizes the glomerular filtration rate (GFR) and minimizes the risk of tissue damage (Lieberthal, 1991). NP enhances diuresis, vasodilation, and inhibition of the RAS (Ushijima et al., 2017). Upregulation of NPs assists in promoting urine flow, GFR, sodium excretion, and decreasing the level of previously raised serum urea and creatinine (Dizaye and Ali, 2019).
Furthermore, the valuable function of NEP appears due to its capability in the conversion of Ang I to Ang (1–7) (Campbell, 2017; Sankhe et al., 2020). Ang (1–7) activates G-protein coupled receptors known as MAS. The receptor activation leads to protection of renal injury by several mechanisms such as counter regulating Ang II and AT1R-induced inflammatory pathways, reducing reactive oxygen species, restoring nephrin protein in podocytes, and increasing diuresis natriuresis, thus mitigating renal injury (Sankhe et al., 2020). The potential of NEP inhibitors as a therapeutic target for kidney disease is still under exploration. It is still not yet established, as in the cases of Alzheimer's and cardiovascular diseases.
Nervous System
NEP inhibition might adversely impact the aging population, especially Alzheimer's disease patients, due to its role in amyloid-β peptides' metabolism (Miners et al., 2011). Several studies reported an age-associated decrease in the expression of NEP in several tissues, together with the brain (Hellstrom-Lindahl et al., 2008; Stanislavskii et al., 1978; Wang et al., 2003). NEP plays a vital role in the mammalian CNS as an enkephalin-inactivating enzyme. It is also implicated in the degradation of amyloid beta-peptide (Aβ42) in the nervous system and more potent in cleaving amyloid peptides than other enzymes (Shirotani et al., 2001).
In the brain, NEP expression has been observed in several areas, including the hippocampus, cortex, substantia nigra, striatum, caudate putamen, and globus pallidus (Back and Gorenstein, 1989; Fukami et al., 2002; Pollard et al., 1989; Vasilev et al., 2021; Waksman et al., 1986). In the neurons, NEP is synthesized in the soma and transported to the synapses through the axon. In the nervous system, NEP is comprehensively located at the presynaptic terminals in the neurons and involved in amyloid beta-peptide (Aβ42) degradation (Iwata et al., 2004).
Several studies showed enhanced NEP expression in GABAergic neurons and parvalbumin interneurons in the human brain, which is found in perisomatic synapses (Pacheco-Quinto et al., 2016). In the hippocampus and neocortex, primarily NEP is expressed in the neurons positive for GABA and metabotropic glutamate 2/3 receptor- and absent in cholinergic and catecholaminergic neuronal cells (Fukami et al., 2002), and it shows a cell type-specific expression pattern in the brain (Fukami et al., 2002; Pacheco-Quinto et al., 2016). Its functional role in the cleavage of amyloid-beta peptides has been studied extensively (Huang et al., 2006; Iwata et al., 2000; Marr et al., 2004).
Several studies reported that NEP expression and degradation of amyloid peptide has a direct correlation (Howell et al., 1995; Iwata et al., 2000; Marr et al., 2004; Yasojima et al., 2001). Its expression is also reduced in several regions of the brain that are susceptible to Alzheimer's disease, including the hippocampus, temporal and frontal cortex (Caccamo et al., 2005; Hellstrom-Lindahl et al., 2008), and mid temporal gyrus (Yasojima et al., 2001). In these studies, its expression was inversely correlated with plaque depositions. Based on these literature, it appears that NEP appears to be a bridge between brain and amyloid plaque deposits.
Apart from amyloid-beta clearance, NEP plays a significant role in the breakdown of neuropeptides, such as SP, bradykinin, enkephalins (Gregoriou et al., 2020; Malfroy et al., 1978), somatostatin, tachykinins, and neuropeptide (NPY) (Bayes-Genis et al., 2016a; Erdos and Skidgel, 1989).
Mechanism of Action of ARNIs
The current situation becomes more alarming and crucial at the current status of the COVID-19 pandemic, where hypertissue inflammation and multiple organ failure are the hallmarks of COVID-19-associated mortality (Mehta et al., 2020b). In such a setting, it becomes essential to revise the role of NEP and investigate the optimization of ANRI's administration. The combination of sacubitril/valsartan (Entresto, Novartis, Switzerland) is the first FDA-approved ARNIs for heart treatment. This inhibitor contains valsartan, a type I Ang II (AT1) receptor blocker (ARB) and sacubitril in the same molar concentration. Upon hydrolysis, this drug gives rise to NEP active inhibitor LBQ657 (Campbell, 2017). Sacubitril/valsartan is beneficial in heart diseases and COVID-19 through two complementary molecular mechanisms.
In SARS-CoV-2 infection, sartans are helpful as they inhibit the angiotensin-mediated activation of AT1R, thus upregulating ACE2 and Ang 1–7 production. Sacubitril balances unwanted degradation of NP, which are counterregulatory to RAAS, causing a decrease in systemic arterial pressure, total blood volume through natriuresis cardiac output, and diuresis (Acanfora et al., 2020c; Rubattu et al., 2020). Current studies support the advantageous effect of sacubitril/valsartan in SARS-CoV-2-infected patients at early stages as it enhances sacubitril's anti-inflammatory properties (Acanfora et al., 2020a, 2020c).
On the other hand, NEP is also responsible for the degradation and delicate balance between bronchodilator peptides like NP and inflammatory cum bronchoconstrictor peptides. It is known to regulate several vasoactive neuropeptides, including SP, bradykinin, and neurokinin A (Rubinstein et al., 1994). Bradykinin signaling complex system is activated in the lung fluid cells of those with the virus and upregulated in COVID-19 patients (Roche et al., 2020; van de Veerdonk et al., 2020).
As a result, despite its beneficial effect on heart health, long-term use of NEP inhibitors may come at the cost of some adversity. Bradykinin expression is majorly regulated by peptidase. Bradykinin, which is an endothelium-dependent vasodilator, is a substrate of NEP and ACE. ACE/NEP inhibitors are commonly used in peptidase inhibitor therapies, leading to increased bradykinin expression (Campbell, 2018). Overexpression of bradykinin may lead to activation of inflammatory cytokines (cytokine storm) in COVID-19 patients.
Several reports showed that increased levels of bradykinin activate NF-kappaB-mediated IL-6, IL-1beta, and IL-8 upregulation through MAPK-dependent pathways in human fibroblast, smooth muscle cells in the airway, synovial fibroblasts, and lung fibroblast (Hayashi et al., 2000; Huang et al., 2003; Pan et al., 1996; Schwaninger et al., 1999; Viljanto, 1991). This “bradykinin storm” may be involved and might play a significant role in the wide variety of symptoms experienced by SARS-CoV-2-infected patients, such as vomiting, diarrhea, headaches, muscle pain, fatigue, nausea, and decreased cognitive function; similar symptoms have been associated with other bradykinin-related conditions.
One of them is hereditary angioedema, a genetic condition characterized by severe swelling throughout the body (Hofman et al., 2016; Kaplan, 2011). Thus, if NEP/ACE is considered inhibitory targets, it is also important to consider bradykinin as a potential target of inhibition to control inflammation and prevent cytokine storm-mediated multiorgan failures (Fig. 2). Moreover, being a major vasodilator peptide, accumulation of bradykinin due to ACE and NEP inhibition may lead to opening up of the blood vessels, causing leakage of plasma substances carrying immune cells in lungs, which may cause or aggravate inflammation. Thus, involving RAS and bradykinin-mediated cytokine storm inhibitors in the therapeutic interventions and mechanistic model of signaling for COVID-19 is highly recommended.
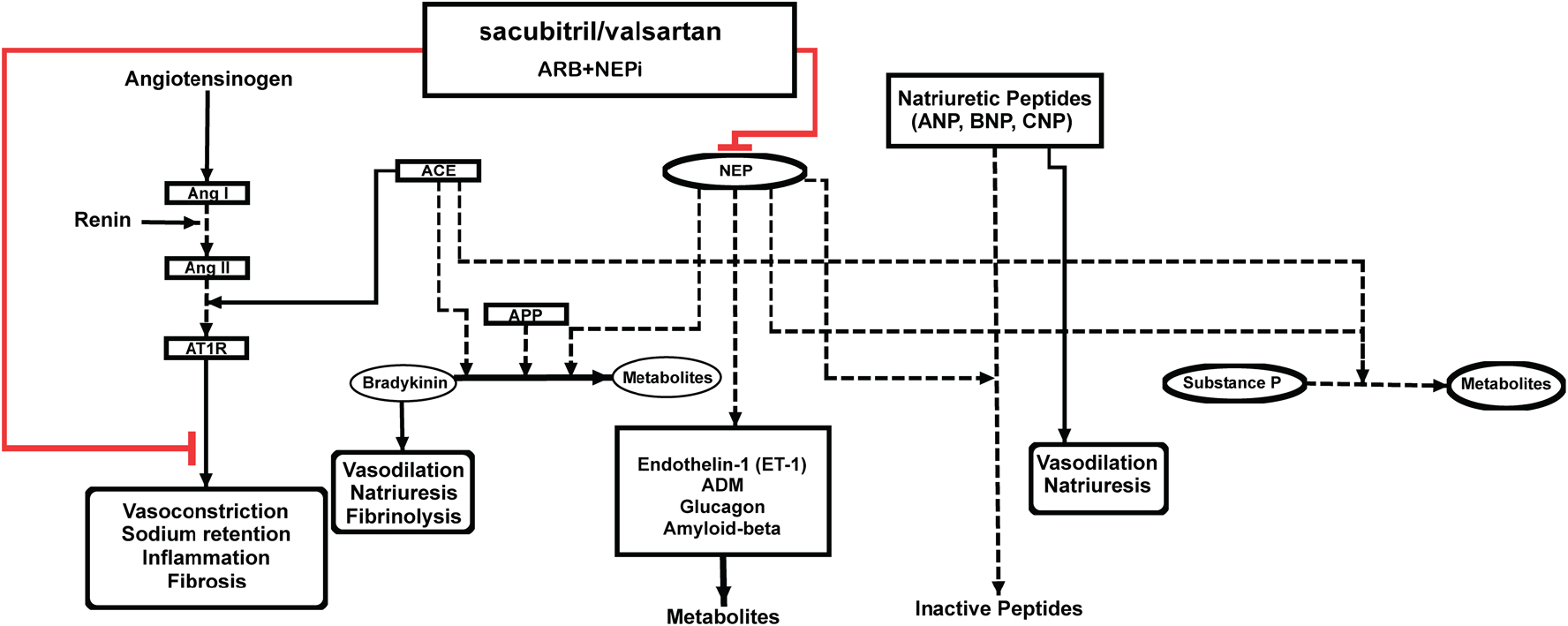
Illustration of the molecular mechanism of sacubitril/valsartan and their significance in progression of inflammatory response. Sacubitril/valsartan inhibit NEP and enhance the expression of various natriuretic peptides. This has an overall effect on Angiotensin II expression. Inhibition of NEP and ACE may lead to increased levels of inflammatory peptides such as bradykinin and substance P. NEP, neprilysin.
Knowledge Gaps, Caveats, and Prospects for Future Research
Certain groups of patients (including those with Alzheimer's disease) can be an at-risk group for receiving NEP inhibitors because decreased NEP levels have been reported in these patient groups in earlier reports (Marr and Hafez, 2014). Chronic NEP inhibition may lead to Alzheimer's disease, dementia, and a neurogenic inflammatory condition that results in inflammatory responses such as erythema, swelling, tenderness, pain, and prostate cancer. Therefore, it is reasonable to maintain a judicious usage of NEP inhibitors to avoid possible adverse effects. Since bradykinin is a significant contributor to angioedema resulting from peptidase inhibitor therapy, administration of bradykinin inhibitors may help reduce the inflammation.
Based on evidence from clinical studies, incorporation of appropriate inhibitors of inflammatory peptides into an ANRI therapeutic regime seems to be a promising remedy. Additional experiments and clinical studies on large human cohorts would help gain valuable insights into the relationships between NEP and COVID-19, facilitating further design of rational treatment strategies.
The SARS-CoV-2 infection is associated with severe inflammation, multiorgan failure, and death in some of the infected patents. Although several repurposed drugs may aid recovery and treatment in intensive care patients with COVID-19, the clinical trials did not indicate whether they really could. Targeting ACE and NEP may offer the prospect of beneficial outcomes in relation to the cardiovascular and renal function, without causing adverse effects such as inflammation and angioedema as an outcome of an increased level of bradykinin.
Footnotes
Acknowledgments
The authors thank the Karnataka Biotechnology and Information Technology Services (KBITS), Government of Karnataka, for assistance to the Center for Systems Biology and Molecular Medicine (CSBMM) at Yenepoya (Deemed to be University), Mangalore under the Biotechnology Skill Enhancement Program in Multiomics Technology (BiSEP GO ITD 02MDA2017). D.A.B.R. is a recipient of a Senior Research Fellowship (SRF) from the Indian Council of Medical Research (ICMR), Government of India. They also thank Yenepoya University for providing research fellowship to D.A.B.R. before the receipt of ICMR SRF.
Author Disclosure Statement
The authors declare they have no financial conflicts of interest.
Funding Information
This research was provided by Karnataka Biotechnology and Information Technology Services (KBITS), Government of Karnataka, under the Biotechnology Skill Enhancement Programme in MultiOmics Technology (BiSEP GO ITD 02MDA2017).