
Abstract
Trisomy 21 is a common birth defect in humans. Screening for trisomy 21 is one of the most important tasks in routine prenatal care and robust noninvasive diagnostics are needed in clinical practice. Urinary proteomics offers a new research platform for diagnostics innovation in this context. We report here new biomarker candidates using urinary proteomics profiling. Specifically, we used liquid chromatography-tandem mass spectrometry (LC-MS/MS) to analyze the proteomes of urine samples from 19 pregnant women (aged 28–44 years) carrying fetuses with trisomy 21 and 22 healthy pregnant women (aged 27–42 years) carrying fetuses with normal karyotype. We identified more than 50 differentially expressed proteins between the trisomy 21 group and healthy group, and most of these proteins were associated with the embryonic development. Importantly, tissue inhibitor of metalloproteinases 2 (TIMP2) and lysosomal-associated membrane protein 2 (LAMP2) were further selected as potential urinary protein biomarkers. We found that the combination of TIMP2 and LAMP2 could differentiate fetuses with trisomy 21 from healthy controls with a sensitivity of 74%, a specificity of 82%, and an area under the receiver operating characteristic curves (AUC) value of 0.82 (95% confidence interval, 0.69–0.95). We conclude that TIMP2 and LAMP2 offer promise as biomarker candidates and warrant further clinical research in larger study samples. These findings further our understanding of the pathological processes involved in fetal trisomy 21 and are poised to accelerate the development of new noninvasive potential biomarkers for trisomy 21 prenatal screening.
Introduction
Trisomy 21,
Trisomy 21 also leads to huge medical and social costs. Screening for trisomy 21 is one of the most important tasks in routine prenatal care (Antonarakis et al., 2020). The most common screening method involves maternal age, information from ultrasonography of nuchal translucency (NT), and multiple second trimester serum markers, such as free beta human chorionic gonadotropin (β-hCG), pregnancy-associated plasma protein-A (PAPP-A), alpha-fetoprotein (AFP), and unconjugated estriol (uE3).
It has been noted that screening by a combination of maternal age, NT, and (PAPP-A and β-hCG) or (AFP, uE3, and β-hCG) has a sensitivity of 94% with a false-positive rate of 5% (Christiansen et al., 2016; Hackshaw et al., 2001).
When these prenatal screening tests are applied to predict a high risk of fetal trisomy 21, more invasive diagnostic tests are needed for clinical diagnosis, such as amniocentesis or chorionic villus sampling (Nicolini et al., 2004). However, the potential risk of miscarriage encourages the search for safer diagnostic methods for trisomy 21.
Recent advances in genomics have led to the development of noninvasive prenatal screening (NIPS) test by sequencing the cell-free fetal DNA isolated from a maternal blood sample. There are studies reporting that the detection rate of NIPS is at least 98% and the false positive rate is 2% or lower (Chiu et al., 2011; Palomaki et al., 2011). Despite that NIPS test is gaining acceptability, however, the high cost restricts its application in all patients.
As a convenient source of clinical test sample, urine has the advantage of fast and noninvasive sampling. In healthy individuals, 70% of the urine proteins/peptides originate from the kidney and the urinary tract, and 30% of the proteins/peptides from the ultrafiltration of blood within glomerulus (Thongboonkerd and Malasit, 2005). Hence, urine may not only contain bioinformation from the urogenital system but also from other distant organs. Recently, two studies have shown that urine peptide/metabolic profiles of pregnant women with trisomy 21 fetuses are significantly different from those with chromosomally normal fetuses (Iles et al., 2015; Trivedi and Iles, 2015). However, there are still no biomarkers derived from urine samples available for prenatal screening or diagnosis of trisomy 21 in clinical setting.
Multiomics research (Kunej, 2019) and applications of proteomics toward urinary profiling offer promise for biomarker discovery and development. In a previous investigation, we examined the urine samples from pregnant women with trisomy 21 fetuses using matrix-assisted laser desorption/ionization time of flight mass spectrometry (MALDI-TOF MS) (Shan et al., 2019). However, the interpretation of peptides identified by MALDI-TOF for biomarker potential is complex and call for development work by other methodologies as well. Hence, in the present study, using liquid chromatography-tandem mass spectrometry (LC-MS/MS), we report novel observations on urinary proteomic profiles in pregnant women with trisomy 21 fetuses.
More than 50 differentially expressed proteins (DEPs) in maternal urine with trisomy 21 fetus were identified in this study, and two urine proteins were selected as lead candidate biomarkers for trisomy 21 in future clinical diagnostic development research.
Materials and Methods
Participants and urine collection
A total of 41 pregnant women who received amniocentesis prenatal diagnosis for fetal aneuploidies in the second trimester were recruited and participated in the present study conducted in Beijing Obstetrics and Gynecology Hospital in China from October 2016 to January 2018. Trisomy 21 was confirmed by karyotyping following amniocentesis (Nicolini et al., 2004). The detailed participant recruitments and the exclusion and inclusion criteria were described previously (Shan et al., 2019). Clean catch urine samples collected from each participant in the morning were put into an ice-cooled box. Subsequently, the samples were aliquoted and stored at −80°C within 3 h.
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Beijing Obstetrics and Gynecology Hospital (Approval No: IEC-B-03-V01-FJ1). Written and informed consent was obtained from all subjects in the study.
Urine sample preparation
Frozen urine samples were thawed at 37°C, and the filter-assisted sample preparation method was applied for urine sample processing. In brief, after the urine samples were centrifuged at 2000 g for 10 min to remove cell pellet, 500 μL of urine supernatant was taken and solid urea was added to adjust the final concentration to 8 M. Then the urine samples were concentrated by centrifugation at 14,000 g in ultrafiltration tubes (3 kDa, Millipore). The urine protein was reduced by 30 mM of dithiothreitol at 37°C for 1 h, followed by alkylation with 60 mM of iodoacetamide at room temperature in the dark for 30 min. Next, the urine protein was washed with urea buffer (8 M of urea in 100 mM of Tris-HCl, pH 8.2) for three times, and 50 mM of ammonium bicarbonate for three times.
The obtained urine protein was quantified with the BCA protein assay kit (CWBIO, CW0014S), and was digested by trypsin (Promega, V5111) (trypsin: protein = 1:50) in ultrafiltration tubes overnight at 37°C. After being washed with 50 mM of ammonium bicarbonate and water, the digested peptides were dried at 50°C.
LC-MS/MS analysis
The peptides were dissolved with 0.1% formic acid (FA) and analyzed by an Orbitrap Fusion Tribrid mass spectrometer (Thermo Fisher Scientific) coupled with an online nanoflow LC system (EASY-nLC 1200, Thermo Fisher Scientific). The peptides were separated by a 15 cm C18 column (150-μm-inner-diameter, 1.9 μm resin, ReproSil-Pur C18-AQ, Dr. Maisch GmbH) with 30 min nonlinear gradient from 3% to 35% buffer B (0.1% FA in acetonitrile) at a flow rate of 800 nL/min (0–5 min, 3–12% buffer B; 5–28 min,12–35% buffer B; 28–29 min, 35–95% buffer B; 29–30 min, 95% buffer B). Full MS scan (300 to 1500 m/z) were performed at a resolution of 60,000 followed by MS/MS scan with a duty cycle of 1 sec in top-speed mode.
LC-MS/MS data were processed by MaxQuant software (Version 1.5.2.8) against UniProt human database (20201015). The carbamidomethyl of Cysteine was set as the fixed modification, and the oxidation of Methionine and acetylation of protein N-terminal were variable modifications. All assigned peptides and proteins were filtered with 1% false discovery rate. Proteins with at least one unique peptide were kept for quantification. Intensity based absolute quantification (iBAQ) algorithm was used for protein quantification.
Data analysis
Proteins quantified in at least 20% samples of one group were considered for further analysis. The log2 transformed iBAQ values were normalized with quantile using R (v3.5.3) package limma. A two-tailed t-test was used to identify the DEPs between trisomy 21 and healthy samples. Proteins with p < 0.05 and fold change greater than two were selected as DEPs. Gene ontology (GO) enrichment analysis was performed with DEPs using DAVID v6.8. Principal component analysis (PCA) was performed with DEPs using the factoextra package of the R software.
Four DEPs were selected with p < 0.01 and ratio ≥4 as candidate biomarkers for trisomy 21. To improve the diagnostic effect, the receiver operating characteristic (ROC) curves for the combination of any two of the four selected proteins were created by the probabilities of binary logistic. The combination of tissue inhibitor of metalloproteinases 2 (TIMP2) and lysosomal-associated membrane protein 2 (LAMP2) got the best classification performance.
Data analysis was performed using SPSS 16.0 (IBM Corporation, New York, USA) and R version 3.4.3. All reported p-values were two tailed, and p < 0.05 was considered statistically significant.
The data in this study are provided with the article and the Supplementary Data. Raw mass spectrometry data were uploaded to iProx (https://www.iprox.cn/) (IPX0003335000).
Results
Patient characteristics
The overall workflow of this study is shown in Figure 1. A total of 41 urine samples were collected from 19 pregnant women carrying trisomy 21 fetuses (trisomy 21 group) and 22 carrying healthy fetuses (healthy control group). The clinical information of all the samples is shown in Supplementary Table S1. Because the levels of urinary protein biomarkers may be influenced by maternal age and gestational age (Wald and Watt, 1996), we analyzed the differences in maternal age and gestational age between the two group. As shown in Table 1, the maternal age and gestational age of pregnant women were not significantly different between trisomy 21 group and healthy controls in this study.

The overall workflow of urine proteomics analysis.
Clinical Information in Trisomy 21 Group and Healthy Controls
Proteome profiling of urine samples
In the 41 urine samples, we identified 1511 urinary proteins (Supplementary Table S2) and quantified 1504 proteins (Supplementary Table S3), with an average of 744 proteins quantified from each sample. Among the identified proteins, 63 urinary proteins were only identified in the trisomy 21 group, and 120 proteins were only identified in the healthy controls, while 1328 proteins were overlapped in the two groups (Fig. 2A). The distribution of protein abundance in trisomy 21 group and healthy controls showed good consistency (Fig. 2B).

Urine proteins identified in trisomy 21 group and healthy controls.
DEPs analysis
To eliminate proteins that appeared sporadically, only those proteins present in more than 20% of the urine samples in each group were further investigated. Among the 1091 proteins left, a total of 53 DEPs were identified in the trisomy 21 group compared to that in the healthy controls (Supplementary Table S4). Of them, there were 46 elevated proteins (p < 0.05, ratio >2) and 7 declined proteins (p < 0.05, ratio <0.5) in the trisomy 21 group (Fig. 3A). PCA analysis shows that the trisomy 21 group and the healthy controls have a certain trend of separation based on these 53 DEPs identified from the urine samples (Fig. 3B).
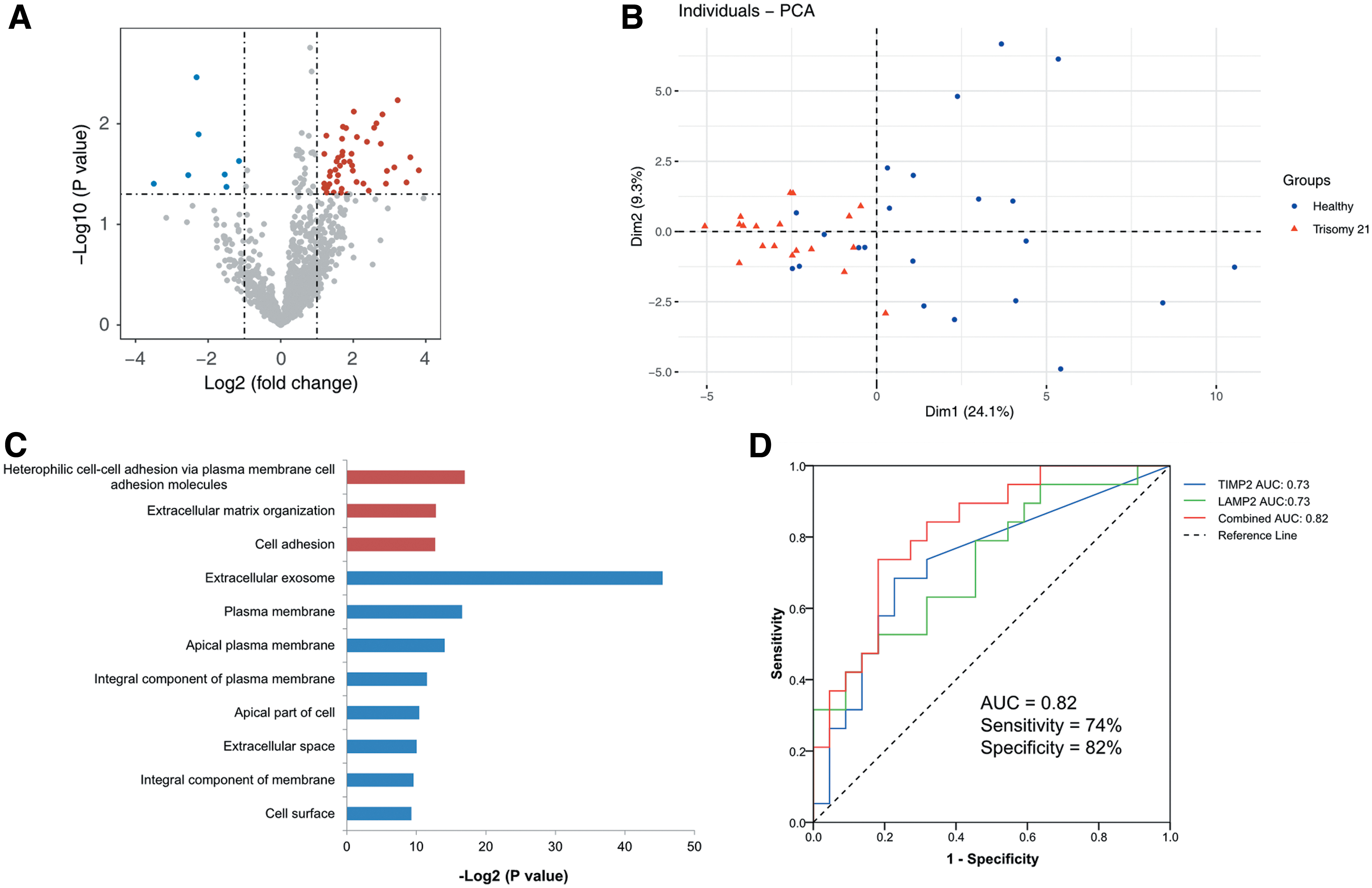
DEPs in urine and diagnostic biomarkers.
GO cellular component enrichment analysis with the elevated proteins showed that extracellular exosome was the most significantly enriched term (Fig. 3C). To identify biological function changes in the urine of trisomy 21 group, GO biological process enrichment analysis was performed with the DEPs. Biological processes related to cell adhesion and extracellular matrix organization were significantly enriched by the elevated proteins in the trisomy 21 group (Fig. 3C).
Potential urinary protein biomarkers for fetal trisomy 21
To identify potential protein biomarkers in maternal urine for fetal trisomy 21, we further screened the DEPs and selected four proteins as candidate biomarkers. Four proteins, including TIMP2, LAMP2, beta-1,4-glucuronyltransferase 1 (B4GAT1), and lysyl oxidase (LOX) were all significantly elevated in the trisomy 21 group with p < 0.01 and ratio ≥4. However, the area under curve (AUC) of the ROC curve for those four proteins were all less than 0.76.
To further improve the diagnostic effect, the combination of any two of the four selected proteins was created using the probabilities of binary logistic. The result showed that the combination of TIMP2 and LAMP2 achieved the best classification performance with a sensitivity of 74%, a specificity of 82%, and an AUC of 0.82 (95% confidence interval [CI], 0.69–0.95) (Fig. 3D). Therefore, the combination of TIMP2 and LAMP2 might serve as a panel of urinary candidate protein biomarkers for trisomy 21. This calls for further clinical diagnostic development research informed by findings from the present study.
Considering that the incidence of trisomy 21 increases with maternal age and some studies reported that plasma peptides profiling has also associated with aging (Cao et al., 2020; Lu et al., 2012), we analyzed whether protein levels of these two candidate biomarkers in urine were related to the age. The result showed that the protein levels of these two candidate biomarkers were not associated with age in neither the healthy group nor the trisomy 21 group (Supplementary Figs. S1 and S2).
Discussion
Although several screening methods have been used in clinic to detect trisomy 21, considering the inadequate diagnostic performance or high cost of these methods, more affordable and, importantly, noninvasive screening test of trisomy 21 is urgently needed. As a commonly used noninvasive sample in clinic, urine is a good source for screening of potential diseases using biomarkers. Our previous study has shown that urine peptidome could offer potential noninvasive biomarkers for screening trisomy 21 (Shan et al., 2019), notwithstanding limitations of MALDI-TOF MS. Hence, to discover identifiable noninvasive potential biomarkers for trisomy 21 prenatal screening and to understand the pathological processes involved in fetal trisomy 21, in this study, we used LC-MS/MS method to profile the global alteration of proteins in maternal urine from trisomy 21 group and control group.
Compared with the healthy group, 53 DEPs were found in the trisomy 21 group. Interestingly, the levels of most of the DEPs (86.8%) were elevated in the trisomy 21 group (Supplementary Table S4), and nearly 65% of elevated proteins were related with exosome (Supplementary Table S5). Considering that we did not specifically enrich urine exosomes in the experiment, this result indicated that exosome-related proteins in urine samples might be associated with the pathogenesis of trisomy 21. Therefore, it is recommended to focus on the exosome component of urine in the future.
Trisomy 21 is featured by dysfunction of multiple bodily systems, especially in the cardiovascular, neurological, and musculoskeletal systems (Antonarakis et al., 2020). Consistent with this, we observed the alteration of proteins associated with embryonic development in the trisomy 21 group (Supplementary Table S4). The most salient feature among these proteins is the elevation of many cell adhesion molecules, such as activated leukocyte cell adhesion molecule (ALCAM), cadherin 2 (CDH2), cell adhesion molecule 2 (CADM2), and dachsous cadherin-related 1 (DCHS1). These proteins play key role in the development of normal neurological system by affecting the neuronal migration and axon pathfinding (Accogli et al., 2019; Bye et al., 2019; O'Neill et al., 2018; Pellissier et al., 2007). In addition, DCHS1 also regulates the cell migration involved in valve formation in heart (Durst et al., 2015).
Other upregulated proteins, such as tyrosine-protein kinase platelet-derived growth factor receptor beta (PDGFRB) and the sorting receptor sortilin 1 (SORT1), are required for normal development of the cardiovascular system and mineralization of the extracellular matrix during osteogenic differentiation by scavenging extracellular lipoprotein lipase, respectively (Maeda et al., 2002; Yue et al., 2019). Among the declined proteins, the stress-responsive protein N-Myc downstream regulated 1 (NDRG1) is very important for myelin sheaths maintenance in peripheral nerves and deficiency of NDRG1 could lead to Schwann cell dysfunction (Okuda et al., 2004). The association of the protein alterations with the clinical features of trisomy 21 demonstrated that the pathological changes of fetus could be disclosed in maternal urine, which is the biological basis for infant disease biomarker discovery in this study.
Based on the altered proteins found in maternal urine, two significantly elevated proteins TIMP2 and LAMP2 had high AUC of 0.82 (95% CI, 0.69–0.95) (Fig. 3D). TIMP2 is involved in very early local maternal recognition of pregnancy by acting on matrix metallopeptidases (Ulbrich et al., 2011), while LAMP2 is required for lysosome-mediated degradative systems and lysosomal dysfunction has been found in trisomy 21 (Jiang et al., 2019). Therefore, TIMP2 and LAMP2 might be considered for future research as clinically useful potential urinary biomarkers for fetal trisomy 21. However, considering the dynamic change of fetal protein expression with gestational age, further study with a longitudinal design for precisive biomarkers within specific gestational age should be more reasonable and promising.
By contrast, β-hCG and PAPP-A, two commonly used clinical serum indicators for trisomy 21, did not perform well in the urine samples in this current study (Supplementary Fig. S3). The previous study showed that serum level of β-hCG in pregnant women with trisomy 21 fetuses is higher than those in pregnant women with healthy fetuses, whereas the serum level of PAPP-A is lower in pregnant women with healthy fetuses (Cicero et al., 2005). In our study, although both β-hCG and PAPP-A could be detected in urine with the same trend in serum, the difference of their levels between trisomy 21 group and healthy controls was not statistically significant (Supplementary Fig. S3). This result is consistent with previous studies that β-hCG and PAPP-A have no clinical screening value in maternal urine, although the concentrations of these two proteins in urine are slightly altered (Spencer et al., 1997).
Limitations
The sample sizes for cases and controls were relatively small and further validation in a larger cohort of trisomy 21 (including sufficient samples collected in different gestational ages) is warranted. The two proteins that we found as potential noninvasive screening biomarkers for fetal trisomy 21, TIMP2 and LAMP2, need to be further validated in real clinical setting. Provided that these two proteins and their diagnostic performance stand the test of further validation, other detection methods with relatively lower cost, higher convenience, and throughput, such as enzyme-linked immunosorbent assay (ELISA) or rapid test strip, could be applied for their detection with an eye to urine-based diagnostic innovation for trisomy 21 screening.
Conclusions
We conclude that TIMP2 and LAMP2 offer promise as biomarker candidates and warrant further clinical research in larger study samples. These findings will further our understanding of the pathological processes involved in fetal trisomy 21 and are poised to accelerate the development of new noninvasive potential biomarkers for trisomy 21 prenatal screening.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.