
Abstract
It is estimated that 50% of patients with coronavirus disease 2019 (COVID-19) have varying degrees of renal involvement. In this clinical biomarker development research, we examined in a retrospective study design the temporal changes in biochemical laboratory parameters in relation to the development of acute kidney injury (AKI). In a sample of 399 patients admitted from May 2020 to May 2021 to a tertiary health care intensive care unit (ICU), the incidence of AKI was 27.3%, and the median time to AKI was on 7th day of ICU admission. Most common etiology of AKI was kidney hypoperfusion. Within 72 h of developmental of low blood pressure, 63.76% developed AKI. The likelihood of AKI was higher in those with elevated serum ferritin, aspartate transaminase, and thrombocytopenia (low platelet count). A cutoff value of 750.3 ng/mL [area under the ROC curve (AUC) = 0.777] for serum ferritin, and 40.05 U/L for alanine aminotransferase (AUC = 0.677) 1 day before development of AKI displayed, respectively, a sensitivity of 76.2% and 64.3%, whereas the specificity was 69.5% and 64.1%, respectively, for these two biochemical predictors. A cutoff value of platelets (152.50 × 109/L [AUC = 0.75]) measured 4 days before development of AKI, displayed 83.3% sensitivity and 16.4% specificity. Taken together, our study thoroughly examined the temporal association of various clinical and laboratory parameters with AKI and prediction models were developed as per results of the time series data. These observations in a tertiary health care setting contribute to ongoing efforts for biomarker discovery and development using routine biochemical tests so as to forecast AKI in patients with COVID-19.
Introduction
It is estimated that 30
The reported incidence of AKI in Indian multidisciplinary ICUs with non-COVID-19 disease is 62.5% and the most common cause of AKI in this subset of critically ill patients is sepsis (Kulkarni and Bhosale, 2020). A prospective observational study from India that includes all patients admitted to a hospital with COVID-19 symptoms reported a low incidence of AKI (3.16%) but highlights, at the same time, a high mortality rate (55.85%) in this subset.
Prognosis is also guarded in survivors as progression to chronic kidney disease (CKD) rate is high (49%) in patients developing AKI after admission in the hospital (Bansode et al, 2022). The incidence of AKI and the associated death rates are expected to be higher in cohorts with more severe forms of COVID-19 disease. In a previous study from our center, in a multivariate logistic analysis, we found the mortality to be 40% in COVID-19 patients admitted to ICU (Ganesan et al, 2021). The incidence of AKI and its predictors remain to be determined comprehensively in world populations, however, so as to move toward evidence-based clinical management of COVID-19 and attendant AKI.
Moreover, reports on the incidence and predictive factors of AKI in patients with COVID-19 are limited and those that are reported are generally in high-income countries (Argenziano et al, 2020; Lendorf et al, 2020; Nowak et al, 2020). There is a lack of research on the incidence and outcomes of COVID-19-related AKI from low- and middle-income countries (LMICs). The presence of comorbid risk factors such as coronary artery disease, congestive cardiac failure, CKD, chronic liver disease, and lack of public health infrastructure could variably influence the outcome of the AKI in LMICs.
Pathophysiology of AKI associated with COVID-19 is complex; the interplay of virus-mediated injury, cytokine storm, dysregulation of complement, and microangiopathy with other known risk factors for AKI such as sepsis, abdominal compartment syndrome, low cardiac output, and persistent hypotension need to be explored. This retrospective study aimed to identify the incidence of and the predictive biochemical variables for AKI in critically ill COVID-19 patients admitted in a public sector referral hospital using longitudinal characterization of the clinical and laboratory parameters.
Materials and Methods
Study design
A retrospective cohort study of adult patients (≥18 years), diagnosed with COVID-19, as confirmed by real-time polymerase chain reaction for SARS-CoV-2 was performed in an ICU of a tertiary care hospital in the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India. Patients with moderate-to-severe COVID-19, escalated for critical care management from isolation wards of the hospital to the ICU from May 2020 to May 2021, were included. Patients with history of previous hospitalization were excluded. We also excluded patients with pre-existing kidney or urinary tract dysfunction, CKD (estimated glomerular filtration rate <60 mL/min), kidney transplant, ICU stay of <24 h, patients with immunosuppression, patients with incidentally diagnosed COVID-19 when admitted for non-COVID-19 medical, surgical, or obstetrical emergencies, and patients with abdominal distension or ascites.
The authors' Institute Ethics Committee approved the study (NK/6902/Study/618) and methodology followed was in accordance with regulations stated in the Declaration of Helsinki. The requirement for the consent was waived off by the Institute Ethics Committee as this was a retrospective study.
Data curation and patients' outcomes
The clinical outcome of interest for this study was development of AKI. The diagnosis and staging of AKI (Supplementary Table S1) were done using the Kidney Disease Improving Global Outcomes (KDIGO) criteria (Machado et al, 2014) and patients were followed for AKI from the 1st day of their ICU admission until discharge or death.
We gathered the data related to various demographic details, chronic comorbidities (hypertension, diabetes mellitus type 2, coronary artery disease, chronic obstructive pulmonary disease, asthma, tuberculosis, stroke, and hypothyroidism), clinical features on admission, serial vital signs (pulse oxygen saturation and blood pressure), serial laboratory tests (hemoglobin, neutrophil-to-lymphocyte ratio, ratio of partial pressure of oxygen to the fraction of inspired oxygen [PaO2/FiO2], serum lactate levels, total leukocyte count [TLC], platelet count, activated partial thromboplastin test [APTT], international normalized ratio [INR], D-dimer, fibrinogen, total proteins, albumin, liver function tests, namely, aspartate aminotransferase [AST], alanine aminotransaminase, lactate dehydrogenase [LDH], renal function tests in relation to serum urea and serum creatinine, serum ferritin, and procalcitonin). The data on use of invasive mechanical ventilation and vasopressor requirement in context to the onset of AKI were also obtained.
Statistical analyses
The median day of developing AKI was calculated and termed t0. We time locked the time series clinical variables to the day of AKI onset (t0). Regression analysis was done to assess the biochemical predictors of AKI onset in hospitalized COVID-19 patients. The data were presented using odds ratio (OR) and 95% confidence interval with p-value obtained using binomial regression model. Line trends of the biochemical measurements before and after t0 in AKI group and non-AKI group presenting mean and standard error of mean were made. The statistically significant predictors obtained through regression model were considered for receiver operating characteristics (ROC) curve. The ROC was plotted for 6 days before the onset of AKI.
Sociodemographic characteristics (including presence of comorbidities) and disease profile of AKI and non-AKI group were presented using frequency distribution and chi-square test of association. Normally distributed continuous measurement data are expressed as the mean ± standard deviation (SD) and non-normally distributed continuous variables are expressed as the median (25th percentile, 75th percentile [Q25, Q75]). The chi-square or Fisher's exact test was used as applicable for categorical variables and Student's t-test was used to compare continuous variables. Statistical analysis was done using the IBM® SPSS® for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA) and a two-tailed p-value of <0.05 was set as statistically significant.
Results
Out of a total of 679 patients transferred to the ICU for escalated care, 280 did not meet the inclusion criteria and only 399 patients with COVID-19 and lung involvement were enrolled in the cohort group (Fig. 1). Case files of enrolled patients were followed up until discharge or death in ICU and demographic, biochemical, and clinical data were recorded. Overall, the incidence of AKI was 27.31% (n = 109) as per KDIGO criteria, and majority of the AKI patients (61.46%; n = 67) had stage 1 disease (1.5–1.9 times increase in baseline serum creatinine levels). Median time to AKI was on 7th day of ICU admission (Supplementary Fig. S1).

Study flow diagram.
Out of 399 patients enrolled, 40 developed AKI within 24 h of ICU admission and 107 patients had ICU stay of <7 days. To enable predictive modeling for onset of AKI, longitudinal characterization of clinical and biochemical variables was thus feasible only from remaining 252 patients (147 patients had to be excluded as ICU stay was less than median time to development of AKI, which was 7 days in our cohort).
The mean age of patients developing AKI was higher than those not developing AKI. Percentage of patients with coronary artery disease and total number of comorbidities were also higher in AKI group. Clinical features at hospital admission were comparable in both the groups (Table 1). A greater proportion of patients requiring mechanical ventilation developed AKI (44.6%, 58/130) as compared with those managed using noninvasive oxygen therapy (9%, 11/122). 63.76% of patients developed AKI within 72 h of developmental of low blood pressures. Ninety-two percent of patients administered vasopressors/inotropes for prolonged period (>72 h) for maintenance of hemodynamic stability developed AKI thus highlighting hypoperfusion as an important etiological factor for development of AKI in our cohort. Administration of anesthetic drugs (sedatives/hypnotics/narcotics) to facilitate intubation in patients with COVID-19 contributed significantly to hypotension in this subset (Supplementary Fig. S2).
Sociodemographic and Clinical Profile of the Patients in Acute Kidney Injury and Nonacute Kidney Injury Groups
Chi-square test used for categorical variables. A p-value of <0.05 is significant.
Note that 147 patients were excluded from the final analysis (40 developed AKI within 24 h of ICU stay and 107 had ICU stay of <7 days [median day of developing AKI]).
Using Student's t-test. The p-values in bold are significant (<0.05).
2.9% patients had diabetic ketoacidosis in the AKI group and 1.1% in the non-AKI group (p = 0.302).
AKI, acute kidney injury; COVID-19, coronavirus disease 2019; ICU, intensive care unit; OR, odds ratio.
Biochemical predictors of hospital acquired AKI
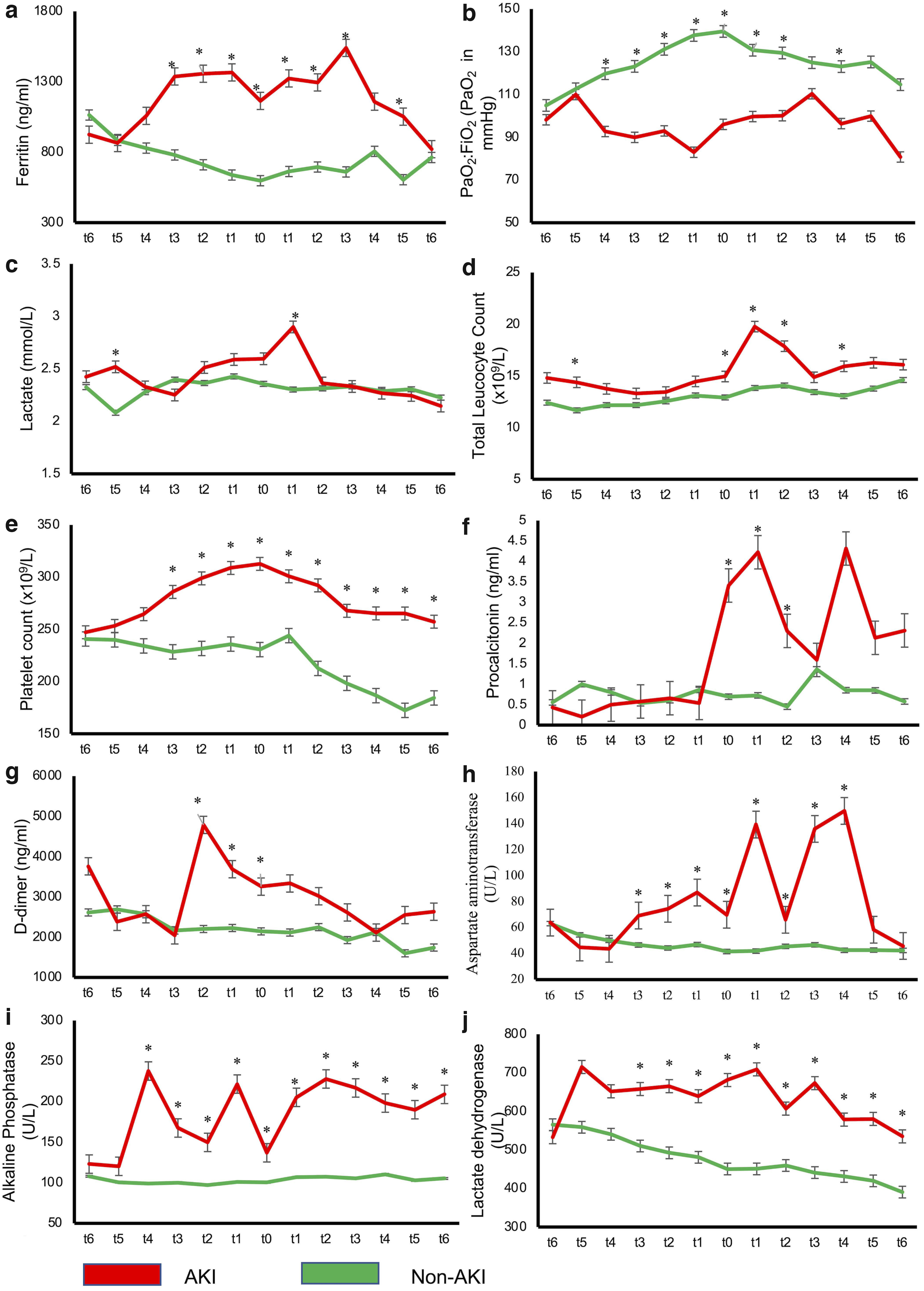
Line trends were plotted and compared for AKI and non-AKI group using mean values of 18 biochemical parameters recorded on daily basis for a period of 13 days from day of ICU admission. Day 7 of ICU stay was labeled as t0 (day of onset of AKI) and distribution of variables was depicted 6 days before and 6 days after t0 (Figs. 2 and 3). Convergence and/or divergence between two line trends (AKI and non-AKI group) for each biochemical parameter were noted and Student's t-test was used to identify any statistically significant difference at all 13 time points marked on the line graphs.
(
(
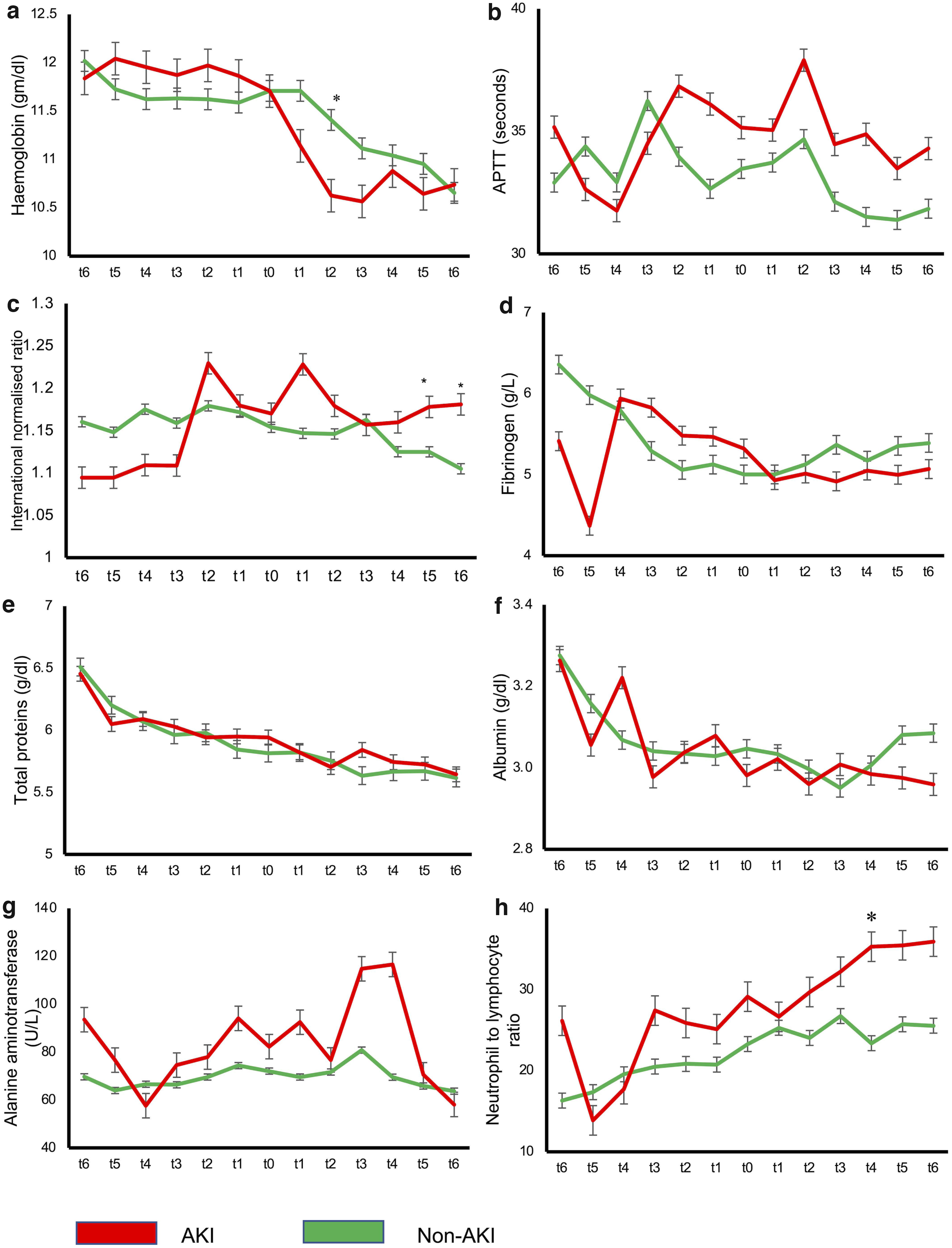
Parameters with maximum divergence at t0 and convergence at time of ICU admission were assumed to be most predictive of development of AKI and Figure 2 depicts the line trends of mean values of such parameters, namely, serum ferritin, lactate, platelet counts, D-dimer, alkaline phosphatase, PaO2/FiO2 ratio, TLC, procalcitonin, AST, LDH, and the respective p-values at different time points, which were statistically different between the two groups. Figure 3 depicts the line trends of parameters with either divergence at time of ICU admission, convergence before onset of AKI and/or multiple spikes thus suggesting no relationship and hence no predictability for development of AKI. Serial values of hemoglobin, INR, total proteins, albumin, fibrinogen, alanine aminotransferase, APTT, and neutrophil to lymphocyte ratio followed this pattern and the difference in mean values between the two groups were also not statistically significant.
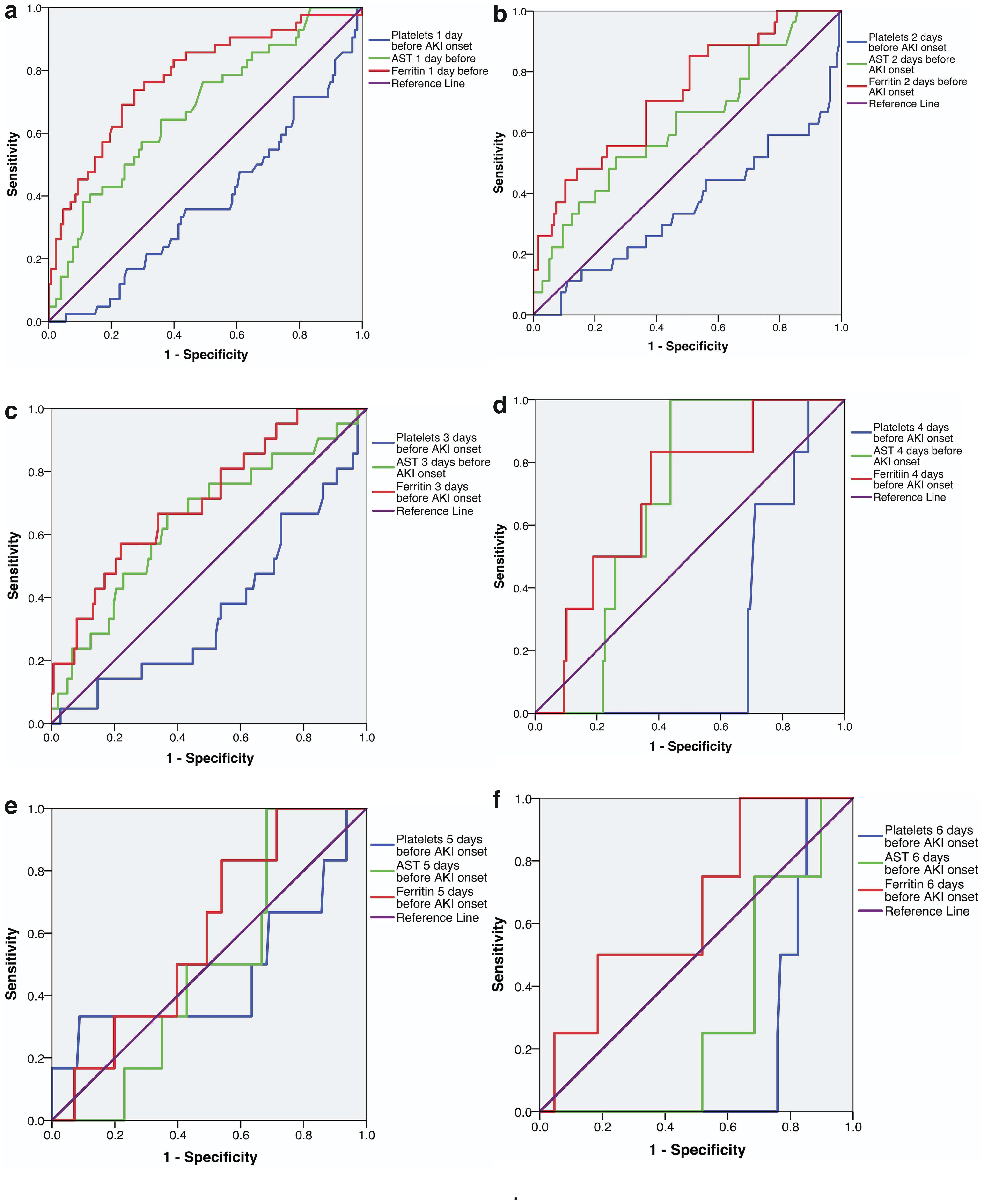
Maximum divergence was noted in the values of all 18 biochemical parameters a day before onset of AKI, and so binomial regression modeling was done on these values. Analysis revealed that likelihood of AKI development was higher with reduction in platelets count (OR = 0.989) and elevation in AST as well as ferritin levels (OR >1, [Table 2]). The mean (SD)/median (IQR) values of these three variables 1 day before the onset of AKI were also significantly different (Supplementary Table S2). Platelet counts, AST, and ferritin levels were considered for ROC curve plots (Supplementary Table S3). The ROC were plotted for 6, 5, 4, 3, 2, and 1 day before the onset of AKI (Fig. 4).
(
Binomial Regression Model to Test the Biochemical Predictors 1 Day Before Onset of Acute Kidney Injury
The p-values in bold are significant.
NLR, neutrophil to lymphocyte ratio; PaO2:FiO2, ratio of arterial partial pressure of oxygen to fraction of inspired oxygen.
A cutoff value of 750.3 ng/mL for serum ferritin measured 1 day before the AKI onset displayed a sensitivity of 76.2% and specificity of 69.5% for AKI [area under the ROC curve (AUC) = 0.777]. For AST, sensitivity and specificity for AKI detection were 64.3% and 64.1%, respectively, with a cutoff value of 40.05 U/L (AUC = 0.677). For platelet count sensitivity and specificity was 78.6% and 9.4% with a cutoff of 152.5 × 109/L and AUC of 0.621. The AUC for platelets was 0.75 and corresponding cutoff value was 152.50 × 109/L when the prediction was done using measurements 4 days before development of AKI (83.3% sensitivity and 16.4% specificity).
The ability of serum ferritin and AST in predicting AKI decreased as the time duration from the event of interest (development of AKI) increased, which is reflected in the AUC values reported on ROC analyses (0.777, 0.726, 0.709, 0.699, 0.598, and 0.653 for serum ferritin and 0.677, 0.632, 0.645, 0.677, 0.493, and 0.303 for AST 1, 2, 3, 4, 5, and 6 days before onset of AKI, respectively).
Mortality among those developing AKI was 74.31% (81/109) and those without AKI was 22.4% (65/290) and this difference in outcome was statistically significant emphasizing the need to predict and prevent the development of AKI. Ten (21.27%) patients required RRT (slow-low efficiency dialysis), but none survived. The indication for dialysis was fluid overload and hyperkalemia in 80% and 20% patients, respectively. AKI resolved in 15 (recovery rate of 37.5%) patients, but all had stage 1 severity of AKI.
Discussion
Established prediction models for onset of AKI use “on admission” clinical and biochemical characteristics and fail to consider the temporal changes in the aforementioned parameters. The accuracy of these models is thus questionable especially when used in a pandemic context as patients are admitted at different stages of disease severity. In our study, the temporal association of various clinical and laboratory parameters with AKI were thoroughly investigated and prediction models were developed as per results of the time series data.
In our cohort, the incidence of AKI was 27.31%. There is a great disparity in the incidence figures reported from across the globe; authors from New York, East Asia, and United Kingdom have reported the incidence as 37% (Hirsch et al, 2020), 25% (Chen et al, 2020), and 34.2% (Philips et al, 2021), respectively. In a systematic review and meta-analysis including more than two-third studies from China (20 out of 29 observational studies), the incidence of AKI was reported as 12% (Wenzhong and Hualan, 2020). The difference in the incidence rates of AKI in different cohorts is due to variability in COVID-19 disease severity. This is due to the emergence and circulation of numerous genetic variants of SARS-CoV-2 (López-Rodríguez et al, 2022) and the crucial role of natural killer cells in COVID-19 disease progression (Bernal et al, 2021).
We report a mortality of 74.31% in COVID-19 patients with AKI during the ICU stay, which is much higher than the reported mortality of 52% in critically ill Indian patients admitted with sepsis (bacterial/fungal) as the primary etiology (Gurjar et al, 2013). New York study reports a mortality of 33% in their cohort (Hirsch et al, 2020), which is approximately half of ours. In a systematic review and meta-analysis of 13,137 hospitalized confirmed cases of COVID-19 across 20 cohorts from Asia, Europe, and the United States, the authors report a death rate of 50% (Robbin-Juarez et al, 2020).
High mortality rates in our cohort warrant immediate attention by a team of intensivists to introspect the clinical characteristics, therapeutic interventions, and basic scientists and epidemiologist to identify the variant by genome sequencing of SARS-CoV-2. These figures also underline the challenges of managing critically ill patients in LMICs or low-income countries (LICs). Delayed presentation, limited COVID-19 specialized care at regional hospitals, diminished human resources for ample care and lack of adequate public sector hospitals to cater to the burgeoning cases are the roadblocks encountered in LMICs or LICs.
The main highlight of our study is that time series data of various clinical and laboratory parameters were collected and their association with onset of AKI and temporal progression of disease with AKI was evaluated. We were very meticulous in enrolment phase and while 109 out of 399 patients developed AKI but for longitudinal characterization we excluded 147 patients due to lack of data in view of short ICU stay. A combination of statistical tools was used for longitudinal analyses such as regression analysis, line trends, and ROC curves on the remaining 252 patients.
In our study, platelet count, AST levels, and serum ferritin levels were predictors of AKI. Serum ferritin was the most promising predictor of onset of AKI in COVID-19 cases due to two reasons; first it had the highest AUC value of 0.777 one day before onset of AKI, and AUC values reported 2, 3, 4, 5, and 6 days before onset of AKI were 0.75, 0.726, 0.709, 0.699, 0.598, and 0.653, respectively, thus enabling good prediction until 4 days before onset of AKI. Thrombocytopenia in COVID-19 is predominantly consumptive due to the development of microthrombi and mirrors the progression of COVID-19 toward unfavorable outcome (Bashash et al, 2020). Liver function abnormalities are associated with increased inflammatory markers and abnormal coagulation in COVID-19, and this explains the predictive performance of elevated AST in our cohort (Yu et al, 2021).
Previous studies have established the role of ferritin as a predictive biomarker for COVID-19 associated AKI (Lee et al, 2021; Phillips et al, 2021). However, this is the first study to provide a temporal relationship between this biomarker and the onset of AKI. In inflammatory states, secretion of ferritin from hepatocytes and macrophages (Cohen et al, 2010) leads to hyperferritinemia. This may be considered as a protective mechanism that enables the sequestration of free iron cations that are released during inflammation thus preventing the free iron to take part in the Fenton reaction, and releasing reactive oxygen species (Wenzhong and Hualan, 2020). This iron-mediated oxidative stress is known to cause kidney injury, especially at the level of the proximal convoluted tubule (Balla et al, 2019).
Another proposed mechanism for development of AKI is the formation of microthrombi in the renal tubules. Data collected in our study, however, do not support this pathogenesis as the levels of D-dimers were comparable in both the groups after onset of AKI, negating the probability of this mechanism. In the cohort of patients developing AKI (n = 109) in our study, it was noted that 63.76% developed AKI within 72 h of developmental of low blood pressure. It may, therefore, be inferred that, in a kidney under persistent oxidative stress, an additional factor such as hemodynamic compromise may cause decompensation and precipitate AKI. Hemodynamic instability and rhabdomyolysis have been reported as the leading causes of AKI in 66% and 7% of critically ill COVID-19 patients (Mohamed et al, 2020) and results of our study are also in agreement with them.
This study has some limitations. First, it is a retrospective study. Studying the risk factors for the development of AKI in this subset of patients would have been more relevant if it was a prospective study. Finally, the lack of urine analysis and kidney biopsy, and a lack of analysis factoring baseline medications, such as angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, statins, nonsteroidal anti-inflammatory drugs, and antibiotics, are other limitations.
In conclusion, 27.31% of the critically ill COVID-19 patients developed AKI in our study sample. Serum ferritin level is noteworthy as a decision tool to help forecast the development of AKI. Prevention of the renal decompensation triggered by acute hemodynamic instability and the associated vasopressor use to maintain hemodynamic stability, and identification and correction of the underlying cause (e.g., bacterial or fungal sepsis) for the same should be the goal in patients with COVID-19 ARDS requiring ICU care. These observations in a tertiary health care setting contribute to ongoing efforts for biomarker discovery and development using routine biochemical tests so as to forecast AKI in patients with COVID-19.
Footnotes
Authors' Contributions
Conception, design of the study; acquisition, analysis, and interpretation of data; and drafting and revising the article critically by T.S. Acquisition of data, and drafting and revising the article critically for important intellectual content by R.R., V.K., A.R., R.G., A.B., H.B., N.N.B., and G.D.P. Conception and design of the study; acquisition, analysis, and interpretation of data; and drafting the article by V.M. All authors approved the final version to be published and made a significant intellectual contribution.
Author Disclosure Statement
The authors declare that this research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
No funding was received for this article.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.