
Abstract
Crying is a common complaint in infants. However, crying with bloody tears or hemolacria is an unusual finding in a pediatric emergency department. There are not many conditions that can present with bloody tears. Subconjunctival hemorrhage and hematomas are known to occur with acute Epstein Barr viral infections, accidental trauma, factor deficiencies, tumors such as malignant melanoma, Rendu-Osler-Weber disease, and idiopathic thrombocytopenic purpura. There are also unknown causes. We report an infant with immune thrombocytopenic purpura presented to the pediatric emergency department with bloody tears, who responded well to intravenous gamma globulin therapy. The presence of bloody tears should be carefully investigated as it may represent significant systemic illness, especially with a strong family history of this autoimmune condition.
Case Report
In the ED, the patient was alert and comfortable. His vital signs were as follows: temperature 98.5°F, heart rate 130 beats/minute, respiratory rate 32 breaths/minute, systolic blood pressure 78 mm Hg, and pulse oximetry 100%. Physical examination showed a well-nourished male at 77th percentile for weight, 82nd percentile for length, and head circumference at 93rd percentile. Anterior fontanel was open and flat. Extraocular movements were intact. Pupils were equal and reactive to light and accommodation and red reflex was present. Bloody tears were noted in the patient's right eye, with some dried blood. Clear tears were present in the left eye. Dry blood was present in the right nostril, with bilateral clear nasal discharge. Bleeding sores were observed on the lips. The neck was supple. Heart sounds were normal. His abdomen was soft and nondistended. Multiple petechiae, ∼1 mm in width, were present bilaterally on the dorsal aspect and soles of the feet, the abdomen, legs, and arms. The patient was uncircumcised. The remainder of the physical examination was unremarkable.
Laboratory studies revealed a peripheral white blood cell count of 15,300/mm3 with 10% neutrophils, 3% bands, 70% lymphocytes, and 8% variant lymphocytes. Hemoglobin was 11.3 g/dL, with a platelet count of 12,000/mm3. Prothrombin time was 13.7 s with an international normalized ratio of 1.1 and PTT of 33.2 s. Serum electrolytes were within normal limits. Liver enzymes were elevated with alanine aminotransferase of 129 U/L and aspartate aminotransferase of 122 U/L. Urinalysis had large amounts of blood, with microscopic RBCs of 0–2/hpf. Stool was negative for occult blood. The patient was admitted to the pediatric intensive care unit with diagnosis of ITP. Intravenous immunoglobulin (IVIG) therapy was initiated after consultation with the hematology service. During his hospital course, the patient completed 5 days of IVIG therapy, and received multiple platelet transfusions. The patient recovered without any complications, and his platelet count returned to normal.
Discussion
The conjunctiva can be a site of many degenerative changes. Inflammation may occur due to exogenous infection or chemical and mechanical foreign material. 1 Infection may extend from surrounding area or be blood borne. Conjunctivitis with mucopurulent or purulent discharge is common and universal, but blood-stained tears or bloody tears is an extremely rare condition. 1
There may also be unknown causes. 2 Hereditary hemorrhagic telangiectasia or Rendu-Osler-Weber disease is a hereditary autosomic dominant disease characterized by abnormalities in 1 or 2 genes (9q33-34 and 12q13 chromosomes) involved in repairing the vascular wall. Telangiectasias are vascular dilations that spontaneously bleed from the smallest trauma. The location of the telangiectasias can guide us toward finding the underlying pathology. Thus, periungual telangiectasias are pathognomonic of systemic lupus erythematous, scleroderma, and dermatomyositis, and several of these autoimmune conditions can masquerade as other allergic conditions. 3 Telangiectasias may appear anywhere on the skin and mucous membranes and are frequently seen on the lips, tongue, face, and the palm of the hand. They first appear during childhood and grow larger during adolescence and adulthood. A suspected diagnosis can be reached by evaluating the patient's clinical situation. A full clinical work-up requires endoscopic evaluation of the digestive mucosa and the ear, nose, and throat. The existence of a spontaneous ocular hemorrhagic state in the absence of etiological factors (hemophilia, hysteria, conjunctivitis, vascular tumors, trauma, granulomas, silver nitrate treatments, and tear-duct hematic regurgitation) alerts the possible existence of vascular abnormalities and to take a precise systemic medical history in search of hemorrhagic phenomena with the same characteristics in other bodily structures. 4
The occurrence of bloody tears occurring spontaneously in a patient with epistaxis or gastric hemorrhage should lead to suspicion of hereditary hemorrhagic telangiectasia or Rendu-Osler-Weber disease. 5
Although a sanguineous discharge is a relatively frequent in conditions of acute conjunctival hyperemia and inflammation, occurrence of bleeding from conjunctiva as an isolated phenomenon is exceptionally rare as outlined in the differential diagnosis of bloody tears, severe anemia, jaundice, vascular tumors, Osler-Weber-Rendu disease, hereditary hemorrhagic telangiectasia, hemophilia, and other coagulopathies. Other causes reported are vicarious menstruation, conjunctival manipulation for follicle expression in trachoma, clinical treatment of conjunctiva with silver nitrate and epistaxis with retrograde blood stream into conjunctiva through puncta lacrimalia, and orbital varix giant papillary conjunctivitis. 4
Wiese described a case of a 56-year-old woman presented to the ED with a 2-h history of bleeding from the right nostril. She had tried to stop it by pinching her nose but had then also experienced bleeding from her right eye and ear. 6 The anatomical basis lies in the intimate connection of nose and eye via the lacrimal apparatus. An increase in pressure within the nasal cavity during epistaxis by pinching or blowing the nose can cause retrograde flow of blood through the system and thus lead to bloody tears emerging from the ipsilateral eye. 6 The patient had longstanding perforation of both tympanic membranes and the blood in her nose was also able to travel retrograde via the auditory tube and middle ear into the external auditory canal. This led to the additional bleeding from the right ear. Bleeding was readily controlled by nasal sponge tamponade and she made an uneventful recovery. 6
Baglivo stated that ocular occlusive vasculitis can be observed in inflammatory diseases, including Behçet's syndrome, sarcoidosis, systemic lupus erythematosus, infectious disorders (syphilis and acute retinal necrosis), and toxoplasmic retinochoroiditis. 7 The case reported was diagnostically challenging as the fundus appearance was not characteristic of classic toxoplasmic retinochoroiditis. Hemorrhages are more frequently found in viral infections such as cytomegalovirus retinitis explained by damage to the vascular wall passing through the retinochoroiditis without signs of a vascular obstruction. 7 This case demonstrates the importance of including toxoplasmosis in the differential diagnosis of unilateral hemorrhagic retinochoroiditis in immunocompetent patients. 7
One of us (M.F.) reported cases of Behçet's and cerebral toxoplasmosis in childhood and adult HIV infection; however, there were no bloody tears in these cases.8,9
Yazici described 3 adult patients found to have lacrimal sac pyogenic granuloma with acute dacryocystitis, lacrimal mass, and bloody tears. The nasolacrimal drainage pathway was obstructed in all cases. 10 Radiologic evaluation performed in 1 patient revealed the presence of a well-defined mass in the sac with homogenous contrast uptake. Histopathologic examination revealed capillary proliferation and inflammatory cells in a fibromyxoid stroma. Pyogenic granuloma may develop from the lacrimal sac mucosa and may cause bloody epiphora. 10
ITP is a common autoimmune disease in children, characterized by a low circulating platelet count, caused by destruction of antibody-sensitized platelets in the reticuloendothelial system. 11 T cells are also implicated in antibody production and thrombocytopenia. Antibodies are usually isotype-switched and harbor somatic mutations, consistent with a T-cell-dependent response. 12 The cytokine profile is reported to be consistent with CD4_Th0/Th1 activation, including increased prevalence of the tumor necrosis factor-α (_252) G/G phenotype.4 T-regulatory cells. 13 Decreased Fas expression on Th1 and Th2 cells, increased expression of Bcl-2 mRNA, and reduced Bax mRNA on CD4 cells may each contribute to a breakdown in T-cell tolerance.14,15 Moreover, transforming growth factor β expression (which is associated with an immunosuppressive Th3 profile) correlates with disease activity. 16
Patients with ITP are at risk for hemorrhagic manifestations. Most thrombocytopenic patients experience only minor bleeding, such as epistaxis, petechiae, and bruising. However, subconjunctival hemorrhage is an uncommon clinical presentation in patients with idiopathic thrombocytopenic purpura but has been reported, and the appearance of spontaneous subconjunctival hemorrhage in a patient should be thoroughly investigated as it can be an initial sign of a grave systemic disorder. 17
An infant with hemolacria and epistaxis is an anxiety-provoking experience for both parents and the ED staff. It is important to evaluate and examine the patient thoroughly, and explore all etiologies. As bleeding is involved, the patient should be evaluated for hemodynamic stability and the need for intervention. The 2 major etiologies to search for are trauma and systemic blood disorders, medications, and neoplasms. Thrombocytopenia for <6 months defines acute ITP; a diagnosis of exclusion and a laboratory error should be considered. A complete history, careful physical examination, and laboratory evaluation should eliminate any common causes of secondary thrombocytopenia such as drug exposure, infection, autoimmune diseases, inherited thrombocytopenia, and/or leukemia. 18 The main laboratory finding in acute ITP is isolated and is often severe thrombocytopenia. In more than half of the cases, platelet counts at presentation are <20 × 109/L. It is important to note that a preceding illness or recent immunization with live vaccine may result in thrombocytopenia.19–21
The incidence rate of ITP is thought to be between 4 and 8 cases per 100,000 children. Male and female children are affected equally. 22 However, several studies have reported predominance of boys with ITP in children under 10 years of age.23–25 ITP is commonly seen in children between 2 and 10 years of age, with the mean being 5.7 years of age. 26 The most common hemorrhagic manifestations of this disease are purpura/petechiae (83%), epistaxis (25%), and/or hematuria (4%). The severity of these manifestations is increased when the platelet count falls below 10,000/μL. The most severe hemorrhagic manifestation is intracranial hemorrhage; fortunately. this is rare with an incidence of <1%. 27
Complete recovery occurs in the majority of patients. Most spontaneous remissions occur early. The main focus of management should be on controlling hemostasis, and avoiding external factors that may be responsible. Patients should be placed on bleeding precautions and activity should be limited until the platelet count rises. Further, the avoidance of medication with anti-platelet effect is also critical.
Pharmacological interventions commonly used include regimens of corticosteroids, immunoglobulin (IVIG), and/or intravenous anti-Rho (D) immune globulin. Although such pharmacological treatments have proven to increase the rate at which platelet counts increase, there is no evidence that suggests that a decrease in the incidence is associated with treatment. 28 Reversion to a Th0/Th2 cytokine gene profile after treatment with IVIG correlates with remission in childhood ITP. 29 The mode of action of immune globulin is complex, involving modulation of the expression and function of Fc receptors; interference with the activation of complement and the cytokine network; provision of anti-idiotypic antibodies; and effect on the activation, differentiation, and effector function of T and B cells (Fig. 1). 18
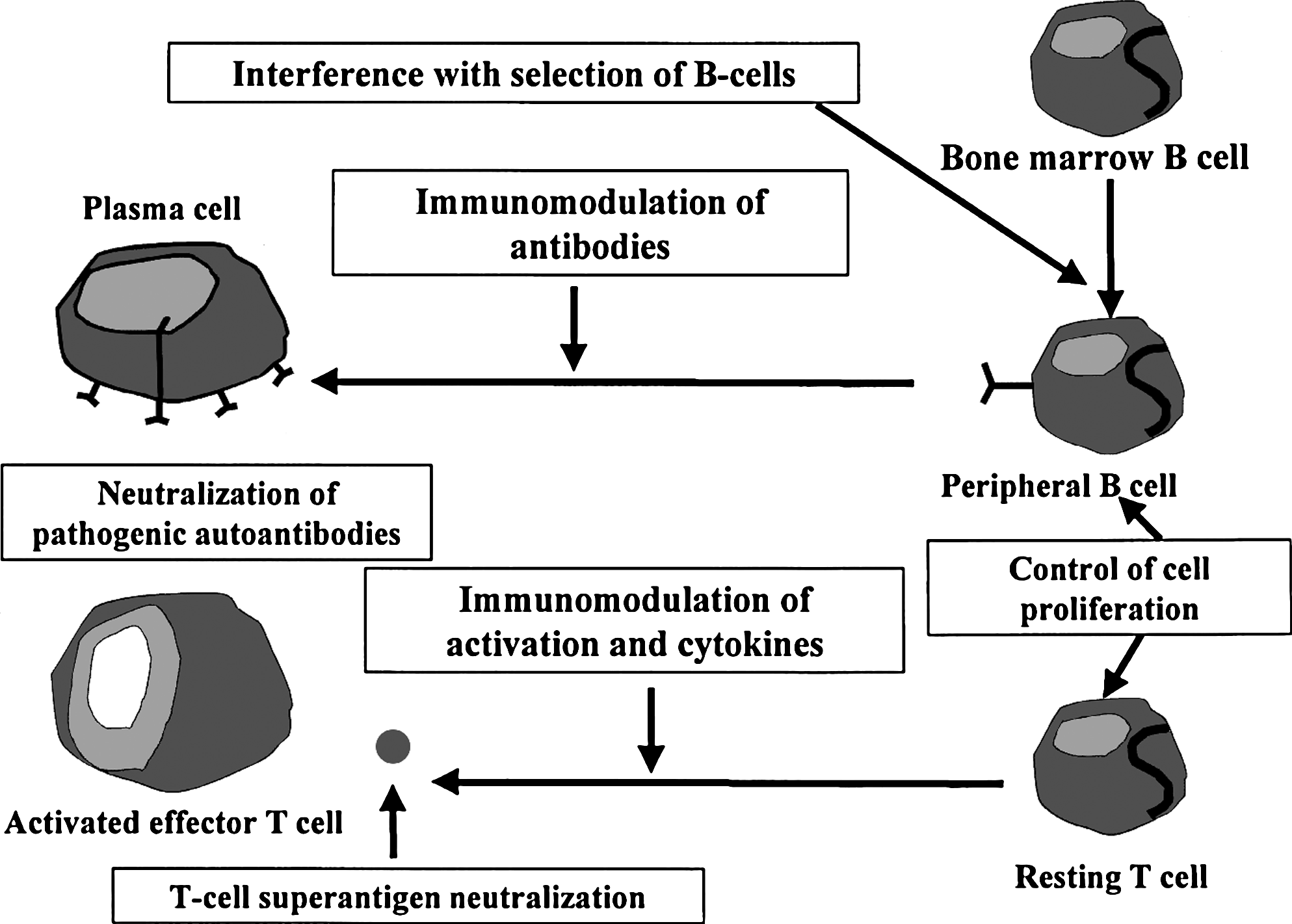
The mechanism for IVIG is shown in Fig. 1 and Table 1. 18 It is important to understand the benefits and account for the risks of each treatment before administration. The use of platelet transfusion is rare and reserved for cases where severe thrombocytopenia is responsible for life-threatening hemorrhage, such as intracranial hemorrhage. ITP is a common condition in children, but bloody tears are an uncommon presentation of ITP. We report an infant with spontaneous subconjunctival hemorrhage as the presenting clinical feature of ITP. It is important that ED physicians be aware that subconjunctival hemorrhage with bloody tears may be the initial manifestation of a systemic condition such as ITP23,24 especially in a family member with ITP. 18
Source: from Frieri. 18
Footnotes
Author Disclosure Statement
No competing financial interests exist.