
Abstract
Histopathology has been considered the gold standard for diagnosis of bronchiolitis obliterans (BO). Although chest computed tomography (CT) has gained acceptance as an alternative tool for diagnosis, no systematic studies validating the diagnostic accuracy of chest CT have been performed in children with BO unrelated to transplantation. A study was undertaken to provide estimates of the strength of association between CT findings and the presence or absence of BO, and to determine if chest CT is predictive of lung biopsy results. In a single-center, retrospective, case–control study, 120 children who had both a chest CT and lung biopsy and no history of lung, heart–lung, or bone marrow transplant were included in this study. Chest CTs were scored for the presence or absence of 24 individual CT findings by a blinded subspecialty-trained pediatric radiologist. Lung biopsies were reviewed by a pediatric lung pathologist for the presence of airway fibrosis, which was classified as mild, moderate, or severe. Ten children had moderate-to-severe BO by lung biopsy. The presence of parenchymal hypoattenuation (P = 0.003) and bronchiectasis (P = 0.001) distinguished these patients from the remaining 110 patients who formed the control group. Combinations of findings improved specificity, and the combination of parenchymal hypoattenuation and vascular attenuation was highly specific (specificity 99.1%; positive likelihood ratio 22.2 and 44.4 for moderate and severe disease, respectively). However, the sensitivity of individual and combination findings was modest. In children with moderate or severe BO, a confident diagnosis can be made with a chest CT that has characteristic radiographic findings, thus avoiding the need for open lung biopsy. However, CT is not an effective screening tool for excluding BO.
Introduction
The diagnosis of BO in children is supported by a compatible clinical history and physical examination, pulmonary function tests demonstrating fixed obstructive lung disease, characteristic features on computed tomography (CT), and lung biopsy. As in many other rare lung disorders, lung biopsy has been considered the gold standard for the diagnosis of BO. 1 However, in the modern era, CT is supplanting lung biopsy because CT is less invasive and lung biopsy does not always identify the characteristic lesions of BO due to its heterogeneous nature.8–12
In patients requiring lung transplantation, the validity of CT in diagnosing BO has been well established. CT findings associated with BO in this population include bronchial wall thickening, bronchiectasis, mosaic attenuation, and expiratory air trapping.13–19 In 2 of these studies, the identification of air trapping with or without bronchial dilatation was correlated with pathologically proven BO.18,19 However, to our knowledge, no comparable validation studies of CT for the diagnosis of BO exist in the nontransplant population. Therefore, we performed the following study to evaluate the diagnostic performance characteristics of specific CT findings in children with pathologically proven BO unrelated to transplantation.
Methods
We conducted a single-center, retrospective, case–control study comparing CT results to biopsy-proven BO. The study was approved by the Institutional Review Board of Baylor College of Medicine.
We included children who had undergone a lung biopsy or other lung resection and had an available chest CT at Texas Children's Hospital between 1991 and 2005. We excluded children with (1) a history of lung, heart, or bone marrow transplant or (2) a lung specimen inadequate for interpretation or demonstrating a tumor. Biopsies inadequate for interpretation were defined as transbronchial biopsies, endobronchial biopsies, needle biopsies, and biopsies with no terminal bronchioles for evaluation. All adequate specimens contained at least one terminal bronchiole for evaluation. CT scans available for review included those filmed and digitized for archival on a picture archiving and communication system beginning in 1993 and those digitally archived on picture archiving and communication system when the transition to a filmless radiology department began in 1997.
The CT scanning technique varied over the period of the study due to multiple CT scanner types, periodic refinement of protocols for imaging of the thorax in children and adolescents of differing ages, and varying clinical indications. The CT examinations were performed with the patient supine, with occasional prone or decubitus positioning to re-expand atelectasis or evaluate for air trapping when expiratory images were not feasible. When breath holding by the patient was feasible, scanning was performed near full inflation for inspiratory images and near end-expiration for expiratory images. Sedated patients were scanned during quiet respiration or during controlled ventilation. A more detailed description of specific CT techniques is available in the Supplementary Methods section (Supplementary Data are available online at www.liebertonline.com/ped).
Each CT study was reviewed by a pediatric radiologist (R.P.G.) with 7 years of postfellowship experience. The radiologist was blinded to the clinical history and pathology findings. An adaptation of the ChILD (children's interstitial lung disease) consortium diagnostic imaging working group score sheet was used to record the presence or absence of 24 individual CT findings. These included parenchymal hypoattenuation, expiratory air trapping, mosaic attenuation, ground glass attenuation, vascular attenuation, consolidation, linear interstitial opacities, reticular interstitial opacities, polygonal septal thickening, honeycombing, nodules, tree-in-bud endobronchiolar opacities, endobronchial mucus plugging, bronchial wall thickening, bronchiectasis, bronchial lumen narrowing, cysts, cardiomegaly, pulmonary artery enlargement, mediastinal or hilar lymphadenopathy, pleural fluid, pleural thickening, pneumothorax, and chest wall deformity.
Pathology specimens were reviewed by a single pediatric lung pathologist (M.K.D.) for confirmation of diagnosis. Biopsies were evaluated for degree of airway subepithelial fibrosis, as well as other superimposed pathologic changes. Airway fibrosis score was determined by the most severely affected airway, as follows: 0 (no airway fibrosis); 1 (mild fibrosis, involving less than one-third of the estimated cross-sectional airway diameter); 2 (moderate fibrosis/constrictive bronchiolitis, involving at least one-third but less than two-thirds of the diameter); and 3 (severe fibrosis/constrictive bronchiolitis, involving two-thirds or more of the airway diameter, or obliterative bronchiolitis, defined as complete obliteration of the airway lumen). The number or percentage of affected airways did not impact scoring. If more than one site was biopsied, all available slides were reviewed and grading was determined by the most severely affected airway in either biopsy. Case and control groups were defined before an independent of correlation with radiographic findings. The case group was defined as patients with moderate or severe fibrosis on biopsy (score 2 or 3), which were considered to be diagnostically significant constrictive or obliterative bronchiolitis by the pathologist reviewer. The control group was defined as patients with no airway fibrosis (score 0) or only mild airway fibrosis (score 1), which was considered to be nonspecific and nondiagnostic for BO by the pathologist reviewer. This approach to pathologic scoring most closely mirrors the diagnostic approach in clinical practice, in which the most severely affected airway supersedes all less affected airways in diagnostic significance for confirmation of suspected BO syndrome. Even one airway with moderate or severe constrictive bronchiolitis was considered confirmatory for BO, whereas multiple mildly affected airways were considered nonspecific and insufficient for diagnosis of BO.
Data were analyzed with SPSS version 13.0 (SPSS, Inc., Chicago, IL). The Chi-square test, with Fisher's exact test where appropriate, was used to evaluate the relationship between individual CT findings (as well as combinations of CT findings) and pathologic diagnosis. P values of 0.05 or less were considered to be statistically significant.
Results
Complete radiographic and pathologic data were available for 120 subjects. The study group consisted of 10 patients, identified as having moderate (n = 5) and severe (n = 5) BO by histopathology. The underlying etiology was postinfection (n = 6), Stevens-Johnson syndrome (n = 1), mixed connective tissue disease (n = 1), and unknown (n = 2). The control group consisted of 110 patients with no (n = 74) or mild (n = 36) BO by lung biopsy. The mean age was 11.1 years (range, 4–17 years) and 6.5 years (range, 2 weeks–17 years) for the study and control groups, respectively. Fifty percent of study subjects and 55% of control subjects were male. Other pathologic features in the control group included findings commonly associated with airway injury [focal periairway fibrosis (4/10), peribronchiolar metaplasia (5/10), focal foamy macrophages/endogenous lipoid pneumonia (2/10)]. Other nonspecific changes associated with prior lung injury included focal hemosiderin-laden macrophages (3/10), focal pulmonary arterial intimal proliferation (5/10), focal organizing pneumonia (2/10), and pleural adhesions (3/10). One biopsy also showed early acute diffuse alveolar damage and one biopsy contained caseating granulomatous inflammation. The patient with Stevens-Johnson syndrome had predominantly large airway fibrosis, as well as bronchiolar squamous metaplasia and mucosal calcification. One patient had BO in the setting of other typical findings of cystic fibrosis. The patient with mixed connective tissue disease had features of chronic interstitial lung disease (lobular remodeling, patchy interstitial fibrosis) and pulmonary arteriopathy, associated with obliterative bronchiolitis.
All of the CT studies included inspiratory images. Additionally, 4 of the 10 (40%) study subjects and 12 of 110 (10.9%) control subjects had expiratory images. Axial noncontiguous high resolution computed tomography (HRCT) images were available for 8 of 10 (80%) study subjects and 42 of 110 (38.0%) control subjects. Both helical CT and axial HRCT images were available for 6 of 10 (60%) of the study subjects and 36 of 110 (32.7%) of the control subjects. Of all cases, 50 had an axial HRCT, 42 had both an axial HRCT and a helical CT, 8 had an axial HRCT only, and 16 had expiratory images (14 obtained by conventional expiratory axial HRCT, 1 obtained by axial HRCT with supine/prone positioning, and 1 obtained by helical CT with supine/prone positioning).
Representative examples of corresponding imaging and pathologic features for moderate and severe BO are shown in Figs. 1–3.
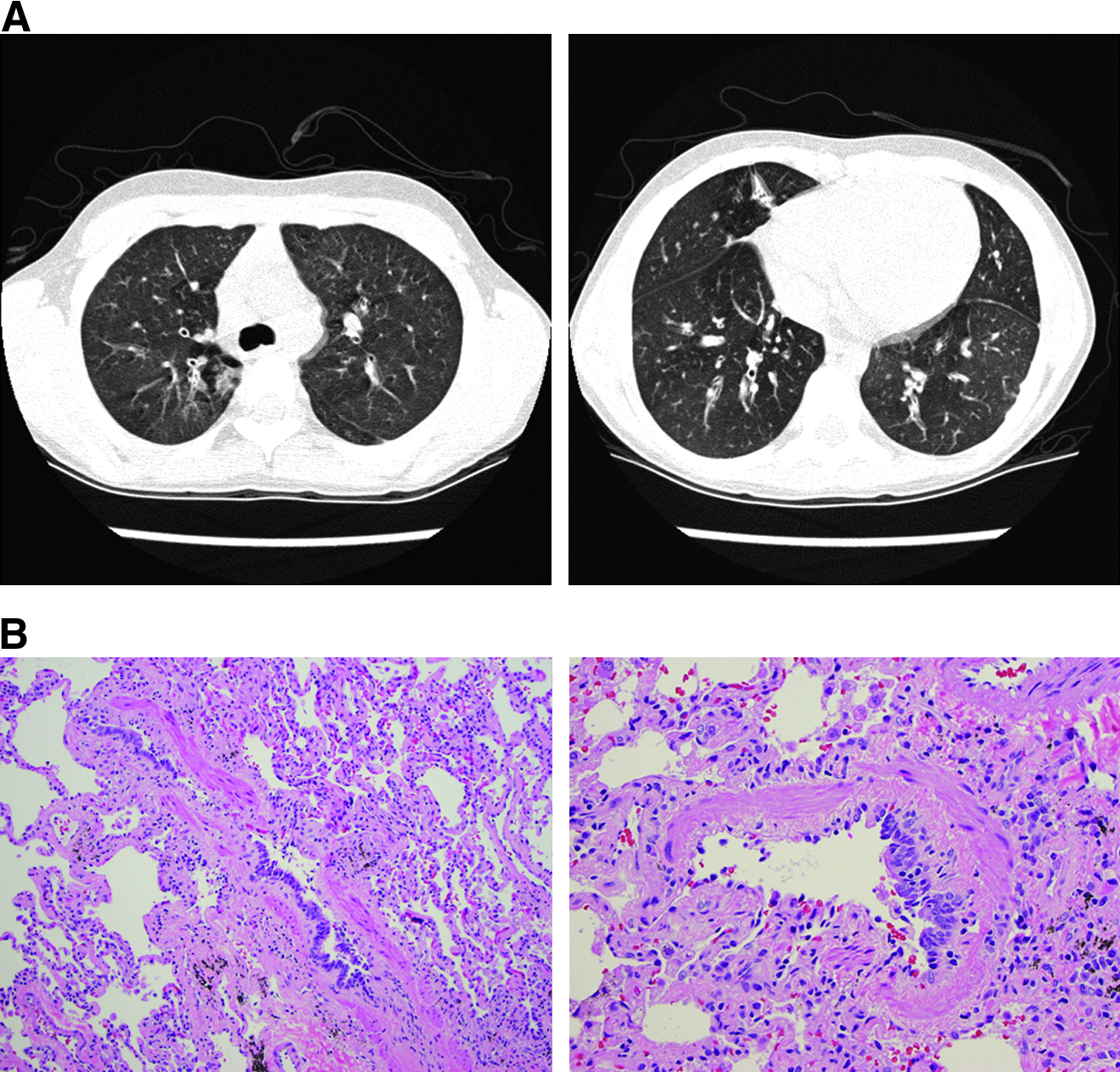
BO, moderate. An 8-year-old boy with moderate postinfectious BO.

BO, severe. A 7-year-old boy with severe BO after recovery from Stevens-Johnson syndrome.
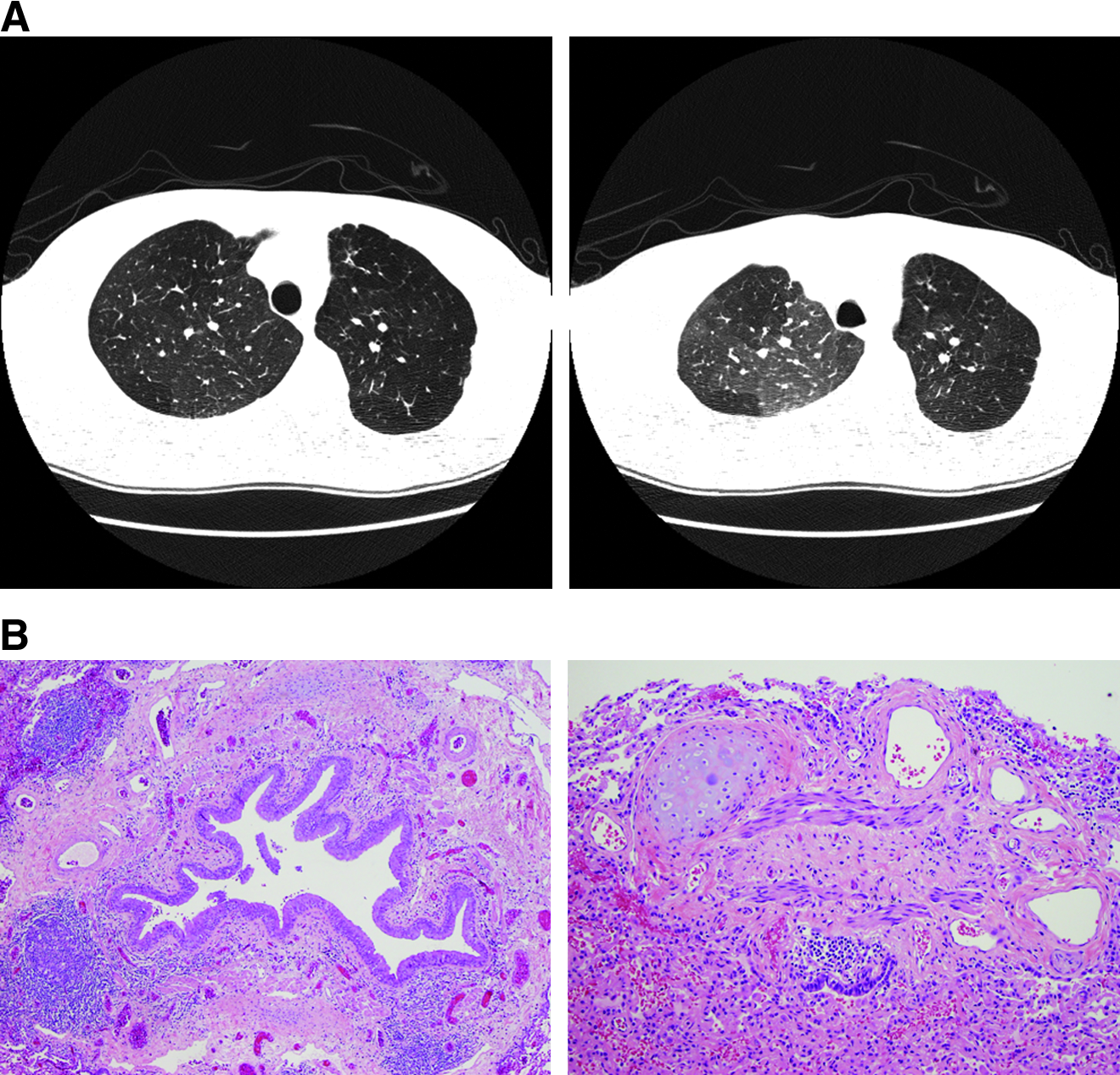
BO, severe. A 10-year-old boy with history of mild prematurity (34 weeks' gestation), a prior episode of bronchitis, and severe postinfectious BO.
Moderate or severe BO
Of the 24 individual CT variables evaluated, the presence of parenchymal hypoattenuation (P = 0.003) and bronchiectasis (P = 0.001) in patients with moderate to severe BO was significantly different from the control group (Table 1). Five additional features (mosaic attenuation, vascular attenuation, tree-in-bud opacities, bronchial wall thickening, and bronchial lumen narrowing) showed a trend toward a statistically significant difference between the study and control groups. Bronchial lumen narrowing, vascular attenuation, and parenchymal hypoattenuation had the highest specificity (≥95.5%), whereas bronchiectasis had the highest sensitivity (70%).
CI, confidence interval; LR, likelihood ratio; PPV, positive predictive value; NPV, negative predictive value.
All possible combinations of these 7 characteristics were analyzed using the Chi-square test with Fisher's exact test where appropriate to determine which combinations could best predict the presence or absence of the disease. These data can be found in Supplementary Data. As expected, combinations of CT findings showed decreased sensitivity but improved specificity for diagnosing BO compared to individual findings. Of the 127 combinations, parenchymal hypoattenuation with one or more of the findings mosaic attenuation, bronchial wall thickening, or bronchiectasis (P < 0.005), and the combination of mosaic attenuation and bronchiectasis (P = 0.002) were highly significant. The most specific combination was parenchymal hypoattenuation and vascular attenuation with a specificity of 99.1%, positive predictive value (PPV) of 66.7, odds ratio of 27.3 [95% confidence interval: 2.2–333.8], and a positive likelihood ratio (LR) of 22.2. Combinations of 3 or more CT findings generally resulted in higher specificities.
Of the 16 subjects who had an expiratory CT performed, 4 had moderate or severe BO and 12 were controls. Despite this small sample size, parenchymal hypoattenuation remained statistically significant with a sensitivity of 75%, specificity of 91.7%, positive LR of 9.0, negative LR of 0.27, and a P value of 0.027. Within this small sample of patients, expiratory air trapping showed a trend toward statistical significance (P = 0.077).
Severe BO
When the cases of severe BO alone were analyzed, parenchymal hypoattenuation (P = 0.003), bronchiectasis (P = 0.007), vascular attenuation (P = 0.013), and honeycombing (P = 0.04) distinguished severe BO from the control group. Honeycombing and bronchial wall thickening had the highest specificity (≥99%), whereas bronchiectasis and consolidation had the highest sensitivity (80%). Honeycombing may be a spurious association, since the single case with honeycombing had concomitant interstitial lung disease. As in the analysis of moderate and severe BO, multiple combinations generally had higher specificities, but lower sensitivities. These data can be found in Supplementary Data Tables S1–S4 in the online version of publication.
Discussion
Previous studies have suggested that, in an appropriate clinical setting, a constellation of CT findings can be used to diagnose BO unrelated to transplantation in children and adults.9–11,20,21 One of the strengths of the study is that the diagnosis of BO was pathologically confirmed. An additional strength is that the study included all patients who underwent a CT and a lung biopsy, resulting in a relatively large number of control cases compared to prior studies. The inclusion of a broad spectrum of clinical pulmonary disorders simulates the practice setting commonly encountered by radiologists who interpret pediatric chest CT scans with limited clinical information.
Our study demonstrates that the diagnosis of moderate to severe BO can be made confidently on the basis of certain radiographic abnormalities. In this study, bronchiectasis was the most sensitive indicator of moderate or severe BO, whereas bronchial lumen narrowing, vascular attenuation, and parenchymal hypoattenuation were the most specific. Combinations of CT findings generally improved specificity but lowered sensitivity.
This study contradicts the traditional dogma that a lung biopsy is necessary to diagnose BO in the nontransplant population. If certain, highly specific radiographic findings are present on chest CT, our study suggests that the clinician can make a confident diagnosis of BO without lung biopsy. However, since the radiographic features are less sensitive, the absence of these findings may justify open lung biopsy in the appropriate clinical setting.
Despite the inclusion of mild BO in the control group potentially diluting the comparison of study and control groups, statistically significant differences in the CT findings were still found, attesting to the strength of specific CT features in detecting more clinically relevant moderate and severe BO. This strength was achieved even though the correlating clinical information was unavailable to the radiologist.
Our study has several important limitations. As in virtually all other studies of this rare condition, this study was retrospective, and the number of moderate and severe cases of BO was small. The value of clinical history and pulmonary function testing was not analyzed.22,23 The inclusion of only patients with both a chest CT and a lung biopsy may have introduced a selection bias toward more severe cases.
Over the study period, the varied CT technique was also a major limitation in interpreting the results. Axial HRCT with control of motion and lung volumes is regarded widely as the optimal method for evaluating fine lung detail for interstitial and peripheral airway disorders, yet not all of the CT examinations included HRCT images due to varying clinical indications and varying feasibility of HRCT in the cases and controls. HRCT with control of motion and lung volumes is feasible only in older patients capable of volitional breath holding or by sedating younger or uncooperative patients and using controlled-ventilation techniques. The slice thickness and interslice gap varied due to the differing CT scanners and scanning protocols in use during the time period covered by the study. Expiratory CT improves recognition of abnormalities such as air trapping compared to inspiratory-only examinations. 24 In this study, the sensitivity for mosaic attenuation and air trapping likely is underestimated substantially, since expiratory images were acquired in only a small fraction of the cases. The sensitivity for bronchiectasis also is likely to be underestimated since not all of the inspiratory images were acquired at full lung inflation. In addition, other findings may have been obscured by blurring from motion artifact in patients in whom volitional breath-holding or controlled-ventilation techniques were not feasible.
Axial noncontiguous HRCT with breath-holding or controlled ventilation technique is preferred to helical CT for surveying the lungs of children due to lower radiation dose and superior image detail, but requires meticulous attention to technique and possibly sedation that may not be available readily at adult community hospitals or outpatient settings where most pediatric imaging studies are performed. This study reflects the varied chest CT scanning techniques encountered in clinical practice and that a high degree of specificity of certain CT findings for moderate or severe BO can be achieved with routine helical chest CT. The presence of these findings on routine helical chest CT may obviate the need for an HRCT or lung biopsy. A future study evaluating the performance characteristics of HRCT with inspiratory and expiratory images compared to routine helical CT in diagnosing nontransplant-related BO would be a welcome addition to the literature.
In our clinical practice, when a diagnosis of BO is considered in the differential diagnosis we would first recommend an axial HRCT with control of motion and lung volumes, including either breath-holding or controlled ventilation technique and inspiratory/expiratory views. If the CT findings are highly specific for BO, then a lung biopsy may not be warranted. However, if the CT images are not conclusive, then we would next recommend proceeding to an open lung biopsy with multiple biopsy sites. In summary, this study indicates that moderate or severe BO in pediatric patients can be diagnosed reliably by the presence of certain characteristic findings on chest CT. Application of these findings to clinical practice could allow some children to avoid invasive lung biopsy procedures. With only modest sensitivity, CT is not an effective screening tool for excluding BO. For children without characteristic findings on chest CT, lung biopsy may still be necessary to confirm the diagnosis.
Summary of key findings
Moderate-to-severe BO in pediatric patients can be diagnosed reliably by the presence of certain characteristic findings on CT.
Individual CT findings with the best specificity for BO include parenchymal hypoattenuation, vascular attenuation, and bronchial lumen narrowing (specificity ≥95.5%). Combinations of findings improve specificity. For example, the combination of parenchymal hypoattenuation and vascular attenuation was very highly specific (specificity 99.1%).
The most sensitive CT finding for nontransplant BO in the pediatric population is bronchiectasis (sensitivity 70%).
If characteristic CT findings are not present, an open lung biopsy may still be necessary.
Footnotes
Acknowledgments
We are grateful to Joe Black for his searches of the radiology information system in the Department of Diagnostic Imaging at Texas Children's Hospital. We also thank Ralph D. Feigin, M.D., for reviewing an earlier version of this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.