
Abstract
Cysteinyl leukotrienes (LT) and airway inflammation are thought to affect exercise-induced bronchoconstriction (EIB). The aim of this study was to investigate the relations between EIB and urinary leukotriene E4 (LTE4) levels and other noninvasive measures of airways inflammation markers in a sample of children with asthma. Pre-exercise urinary LTE4, fractional concentration of exhaled nitric oxide (FeNO) and blood eosinophil count and pulmonary function were measured in 32 children with asthma (mean age±SD, 11.2±2.9 years). Change in forced expiratory volume in one second (FEV1) was determined at 5, 10, and 15 min following 6 min of exercise on a cycle ergometer. Fifteen of the 32 subjects experienced EIB (≥10% decrease in FEV1). The urinary LTE4, FeNO, and blood eosinophil count were significantly related to the maximal percentage decrease in FEV1 after exercise (r=0.44, P<0.05; r=0.36, P<0.05, and r=0.40, P<0.05, respectively). By multiple linear regression, after adjusting for age, gender, and treatment with inhaled corticosteroids, only the pre-exercise urinary LTE4 level was correlated with the maximal percentage decrease in FEV1 after exercise (β=32, P<0.05). Bronchoconstriction after exercise is related to the pre-exercise urinary LTE4 in children with asthma.
Introduction
Among these mediators, cysteinyl leukotrienes (CysLTs) are considered to be the most important bronchoconstricting agent, being a thousand-fold more potent than histamine. 3 CysLTs are produced by mast cells, eosinophils, and alveolar macrophages and increase the vascular permeability, while constricting the bronchial smooth muscles. 4 CysLTs have been elevated in urine samples collected during EIB in some studies,5,6 but not others. 7 The relation between the pre-exercise levels of urinary leukotriene E4 (LTE4) and EIB in children has not been determined.
Measuring the fractional concentration of exhaled nitric oxide (FeNO) is a noninvasive method of evaluating airway eosinophilic inflammation in patients with asthma. 8 Some studies have shown a relation between FeNO and EIB,9–11 suggesting that FeNO may play a role in the pathogenesis of EIB. However, both of the pre-exercise urinary LTE4 levels and FeNO values have not been examined as markers of EIB in children.
The main purpose of the present study was to determine whether the severity of EIB is associated with the pre-exercise urinary LTE4 level, FeNO, blood eosinophil count, or airflow limitations.
Methods
Subjects
Children from 7 to 18 years old diagnosed as having asthma and suspected to have exercise-induced bronchospasm were recruited from the outpatient clinic of the Department of Pediatrics of the Fukuoka National Hospital. Bronchial asthma was diagnosed by pediatricians as recurrent episodes of dyspnea and wheezing. 12 Suspicion of exercise-induced bronchospasm was determined by history of difficulty breathing, cough, or wheeze with exercise by their pediatrician. Children with a history of viral infections or asthma excacerbations during the month preceding the start of the trial were excluded. Parental written informed consent and child assent were obtained for each participant. Study approval was received from the Fukuoka National Hospital Ethics Board.
Study design
Inhaled corticosteroids (ICS), LT receptor antagonists, inhaled long-acting beta2-agonists, and antihistamine medications were withheld for at least 24 h before the test. Short-acting beta2 agonists were withheld for 8 h before the test. The children in the study underwent a physical examination, FeNO measurement, and urine collection; they were then asked to complete a standardized exercise test (described below).
Pulmonary function measurements
Spirometric measurements were performed using a Lilly-type pneumotach sensor in a portable spirometer (Chestgraph HI-701; Chest Ltd.) that meets American Thoracic Society standards. Forced expiratory maneuvers were repeated until 2 acceptable values of the forced expiratory volume in one second (FEV1) were obtained; the larger value was used for the analysis in accordance with American Thoracic Society guidelines. 13 We recorded the values for FEV1, forced vital capacity (FVC), peak expiratory flow, and forced expiratory flow between 25%–75% of the FVC as percentages of the predicted values for the Japanese population, as reported by Nishima. 14
Exercise challenge
Exercise was performed using a cycle ergometer (Bosch Erg 551) for 6 min. The workload was set at 2.1 W/kg. Exercise challenge was not measured if the predicted FEV1 at baseline was less than 65%. The heart rate was monitored throughout the exercise period. During the test, the speed of the cycle ergometer was increased to induce a heart rate of at least 80% of the child's maximum predicted heart rate determined as 210-age. Pulmonary function measurements were made before and at 0, 5, and 15 min after the exercise. A 10% postexercise decrease in FEV1 was considered a suitable cutoff for EIB. 15
Urinary LTE4 levels, FeNO value, and blood samples
Urine was collected in polypropylene bottles containing 4-hydroxy-TEMPO and the aliquots were stored at −35°C until analysis. LTE4 was quantified using a commercial enzyme immunoassay kit (Cayman) after purification using high-performance liquid chromatography, as reported previously. 16
FeNO was measured using a chemiluminescence analyzer (model 280, Nitric Oxide Analyzer; Sievers Instruments). All the subjects underwent on-line measurements of FeNO before the exercise challenge test; the measurements were performed according to the recommendations of the European Respiratory Society/American Thoracic Society. 17
Blood samples were obtained in the 6 months before the test, and the blood eosinophil count and serum immunoglobulin E (IgE) levels were measured; no patients were on systemic corticosteroids at the time.
Statistical analysis
The age, height, weight, baseline pulmonary function, and maximal percentage decrease in FEV1 after exercise were expressed as the mean (SD). Comparisons of differences between groups with or without EIB were made using an unpaired t-test. The urinary LTE4, FeNO, serum IgE, and blood eosinophil count were expressed as the geometric means with 95% confidence intervals. Differences between groups with or without EIB were assessed using the Mann–Whitney U test for continuous variables and the exact Fisher test for categorical ones. The urinary LTE4, FeNO, and blood eosinophil count values exhibited skewed distributions; to reduce skew, these parameters were log 10 transformed before analyses. The correlation coefficients between the variables were assessed using the Pearson's correlation analysis. Multiple linear regression was used to investigate the association of selected pulmonary function, urinary LTE4, FeNO, and blood eosinophil count as independent variables, with maximal percentage decrease in FEV1 after exercise as the dependent variable. Both crude regression coefficients, as well as those obtained after adjustment for age, gender, and treatment with ICS, are presented.
A P-value of <0.05 was considered significant. All analyses were performed with STATA version 10.1.
Results
Thirty two children with asthma were recruited and completed study assessments. (23 boys, 9 girls; mean age±SD, 11.2±2.9 years) 31 of the 32 children exhibited evidence of atopy as defined by a ≥0.7 IU/mL result on a FluorENZYMEimmunoassay (ImmunoCAP) for Dermatophagoides pteronyssinus. Fifteen of the children (47%) were receiving ICS.
The subject characteristics, pulmonary function, maximal percentage decrease in FEV1, and inflammatory markers with or without EIB are shown in Table 1. Fifteen subjects had a decrease in FEV1 of 10% or greater after the exercise challenge [EIB(+)], whereas 17 subjects had a less than 10% decrease[EIB(−)]. Only one child with EIB had the maximal fall in FEV1 at 15 min after exercise. The other 14 children with EIB had these at 5 min after exercise. The 2 groups were very similar in age, baseline pulmonary function, and proportion treated with inhaled corticosteroid or long acting β antagonist medication. The EIB+group had more subjects taking LT receptor antagonist and had greater urinary LT levels (Fig. 1A), although these differences were not statistically significant. In children with EIB, FeNO (Fig. 1B), blood eosinophil count, and serum IgE are significantly higher than in those that did not have EIB.

Differences between 2 groups treated with or without exercise-induced bronchoconstriction.
Data are presented as mean (SD). aData are presented as geometric mean (95% CI). EIB, exercise
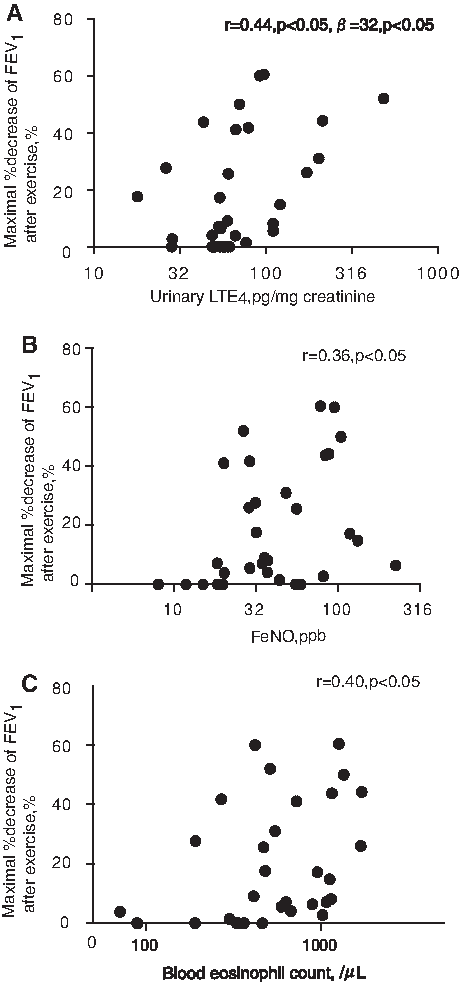
Correlations between the maximal percentage decrease in FEV1 after exercise, the pre-exercise urinary LTE4 level, the FeNO value, blood eosinophil count, and airflow limitation are shown in Table 2. In the asthmatic children, the maximal percentage decrease in the FEV1 after exercise was correlated with the urinary LTE4 level (r=0.44, P<0.05; Fig. 2A) and the FeNO value (r=0.36, P<0.05; Fig. 2B) and blood eosinophil count (r=0.40, P<0.05; Fig. 2C). In multiple linear regression analysis, including FEV1, urinary LTE4 level, FeNO, and blood eosinophil count in the model, the only pre-exercise urinary LTE4 level remained to be correlated with the maximal percentage decrease in FEV1 after exercise (β=32, P<0.05). FeNO was no longer significantly associated.
Relations between maximal percentage decrease in forced expiratory volume in one second (FEV1) after exercise and
Ajusted for age, gender, and treatment with inhaled corticosteroids.
Change of one unit in outcome per increase in maximal percentage decrease in FEV1 after exercise.
P<0.05.
CI, confidence interval.
Discussion
In the present study, we observed that in children with asthma decrease in FEV1 after exercise is related to the pre-exercise urinary LTE4 and in children with asthma in our sample.
Previous studies have reported that FeNO18,19 eosinophilic airway inflammation, 20 and serum IgE 21 play roles in EIB. The FeNO value may reflect aspects of EIB pathogenesis in asthma. Although FeNO and blood eosinophil count were correlated with EIB by univariate analysis in the present study, it was not by multivariate analysis after adjustment for age, gender, and treatment with ICS.
Pre-exercise urinary LTE4 correlated with the severity of EIB in both univariate analyses and after adjustment for age, gender, and treatment with ICS in multivariate analyses. An increase in urinary LTE4 excretion after an exercise challenge has been demonstrated in both adults 5 and children, 6 in some, but not in other reports.22,23 In contrast to our findings, Kikawa et al. 6 in a small series of 13 children with mild asthma and 10 controls did not observe a relationship between the pre-exercise urinary LTE4 level. Urinary LTE4 is now considered to be the most reliable analytical biomarker for monitoring the endogenous synthesis of CysLTs. 24 The urinary LTE4 level does not necessarily reflect the biosynthesis of CysLTs in the lower airways. 25 The CysLTs levels in exhaled breath condensate after exercise and induced sputum on the other day of exercise challenge test were increased in subjects with EIB.26,27
Although we did observe a clinically and statistically significant association between pre-exercise urinary LTE4 levels and postexercise fall in FEV1, there was much overlap in LTE4 levels between those with and without EIB (Fig. 2A).
In conclusion, this study showed that a noninvasive marker, the urinary LTE4 level was correlated with the severity of EIB, whereas other commonly used noninvasive markers of asthma control, FEV1, and FeNO were not.
Footnotes
Author Disclosure Statement
No competing financial interests exist.