
Abstract
Atopic dermatitis (AD) is commonly associated with food allergy. Oral food challenge is the gold standard in the diagnosis of food allergy, but still has some troubles. The aim of this study was to evaluate whether a single test among skin prick test (SPT), measurement of specific immunoglobulin E (IgE), and atopy patch test (APT) or a combination of them could make food challenges unnecessary in patients with AD. Twenty patients affected by AD, under 6 years of age, were evaluated. Every child was investigated for cow's milk and hen's egg allergy using SPT, measurement of serum IgE (sIgE), APT, diagnostic elimination diet for 4 weeks, and open food challenges for milk and egg. The diagnosis of food allergy was established according to the results of the food challenge. We compared the results of all the tests with those of the open food challenge and calculated for each test the following parameters: sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Eight of 40 open food challenges were assessed as positive. None of the diagnostic tools showed a sufficient accuracy to be able to replace the food challenge. However, SPT, APT, and the measurement of sIgE as single parameters showed an NPV of 90%, and the combination of SPT and APT showed an NPV of 92%. Food challenge remains the gold standard for food allergy diagnosis in young children with AD, but the combination of SPT and APT is useful when both tests are negative, because this result provides a guidance in excluding an allergy to the investigated food and could make the food challenge superfluous in this case.
Introduction
The prevalence of both AD and food allergy have increased in the last decades,2,6–8 which might explain the increased demand for a reliable evaluation of patients with suspected food-related symptoms that could have important consequences.9,10
Nowadays, the evaluation of AD and suspected food allergy is a stepwise procedure. The first step is represented by a very careful medical history, and this should suggest which food items have to be investigated. Only when possible causes for the symptoms have been identified, the available diagnostic tools for this pathology are clinical history, skin prick test (SPT), measurement of specific serum IgE (sIgE), atopy patch test (APT; even thought it is only a research tool not yet validated), and oral food challenge preceded by a diagnostic elimination diet, which is considered the gold standard for diagnosing food allergy. 11 The difficulty with oral challenge is that it is time consuming, has an inherent risk of anaphylaxis, and is more intensive in amount of time and personal required. 12 Regarding the other diagnostic tools, SPTs and the measurement of specific sIgE have been used to evaluate an IgE-mediated sensitization to allergens,13–15 but are not able to establish a clear diagnosis. APT is not yet recommended as a routine exam,16,17 but the controversy is still open, because patch testing can be used to determine delayed-type hypersensitivity.18,19
As there is a need to find a reliable evaluation of patients with AD and suspected food-related symptoms, the aims of this study were to examine the efficacy of the available diagnostic tools regarding the 2 main food items that cause food allergy in Europe (cow's milk and hen's egg) and evaluate whether a single test or a combination of them could render food challenges unnecessary, so as to minimize unnecessary investigations.
Patients and Methods
Study population
Twenty children affected by AD as defined by the United Kingdom Working Party's Diagnostic Criteria for Atopic Dermatitis 20 were included in this study. Ages ranged from 7 months to 6 years (median age: 36 months). Inclusion criteria consisted of the following data: patients of both sex, established diagnosis of AD, lack of recent allergological tests, and suspicion of food-related symptoms by parents or physicians. Children with comorbidities such as systemic diseases, immune deficiency, chronic inflammatory diseases, and celiac disease and children who were undergoing a therapeutic diet or taking systemic drugs such as steroids were not included. None of the patients was already eliminating any food. Table 1 shows the characteristics of each patient included in the study.
SCORAD, SCORing atopic dermatitis.
The clinical severity of AD was evaluated according to the SCORAD (SCORing AD) index: 7 children (35%) had mild AD, 10 (50%) had moderate AD, and 3 (15%) were affected by severe AD.
The diagnosis of food allergy was established on the base of the outcome of the food challenges.
Study design
During the first visit, we measured every child's weight and height and calculated the gravity of AD according to the SCORAD index. 21 In the same visit, SPT for casein, lactalbumin, lactoglobulin, and egg white and yolk were performed; later, blood was sampled for determining eosinophilic count and measurement of total IgE and sIgE for cow's milk and hen's egg. Then, APTs for the 2 food items were performed. For SPT, sIgE measurement, and APT, a positive test to any one of the individual components of a food was considered sufficient evidence of sensitization to that food. Finally, every child underwent an elimination diet of cow's milk and hen's egg for 4 weeks and an open oral food challenge for the 2 foodstuffs, one 7 days after the first one.
Skin prick test
We used commercial extracts (Lofarma), each with a standardized concentration (eg, lactalbumin 0.1%, lactoglobulin 0.2%, and casein 1%), and the test was performed according to the instruction of the European Academy of Allergy and Clinical Immunology (EAACI). 22 One drop of each commercial preparation was applied to the patients' forearm, and the test was performed with 1-mm single-peak lancets. Histamine dihydrochloryde was used as positive control and saline solution as negative control. Reactions were checked after 15 min, and the test was assessed as positive if the wheal was ≥3 mm, without reaction of the negative control.
Measurement of specific IgE
Blood was analyzed for concentrations of specific IgE antibody titers for cow's milk, lactalbumin, lactoglobulin, casein, egg white, and egg yolk. All the measurements were performed using FEIA with ImmunoCAP (Phadia), whose detection limit is 0.35 kU/L; the patients who had sIgE levels higher than the detection limit were considered as positive.
Atopy patch test
APT was performed on all the patients during a specific sitting, and commercial extracts of milk, casein, egg white, and egg yolk (Lofarma) were used, each with a standardized concentration (eg, milk 20% and egg 10%). One drop of each commercial extract was put on a filter paper and then applied to the uninvolved skin of the children's back with 12-mm aluminum cups on adhesive tape (Finn Chambers); glycerine was used as a negative control. The patients were dismissed and the parents were asked to not remove the tape and not wash the children's back before going back to the hospital. The test was checked after 48 h, as suggested by the EAACI/GA 2 LEN guidelines 23 : reactions were assessed as positive if erythema together with infiltration or papules was present. The APT was read according to the guidelines of the European Task Force on Atopic Dermatitis consensus of 2003, with a classification of−if no lesions occurred, + for erythema and mild infiltration, ++ for erythema and few papules, +++ for erythema and many papules from 4 to many, and ++++ for erythema, many or spreading papules, and vesicles. Irritant reactions (angry back or flare up) were not regarded as positive.
Food challenges
After an elimination diet of 4 weeks, every child underwent an open oral food challenge for cow's milk and hen's egg as well, the latter being 7 days later the former. When fasting children showed at the hospital, a venous access was obtained, emergency drugs (antihistaminic, corticosteroid, and epinephrine) were prepared, and a clinical examination with regard to the skin lesions and the respiratory and intestinal symptoms was performed before starting the test. Fresh cow's milk was given in successive doses (0.2, 0.6, 2.0, 6.0, 20.0, 60.0, 200.0 mL) that were increased every 20 min after a clinical evaluation and the control of blood pressure and heart rate. Hen's egg was given in a preparation with the following composition: 300 mL of boiled water, mixed with 60 g precooked rice cream, 30 g sugar, 1 egg, and a little saffron; successive doses (0.2, 0.6, 2.0, 6.0, 20.0, 60.0, 200.0 mL) were given every 20 min as for cow's milk.
The test was stopped if clinical symptoms occurred or if the highest dose was reached. If no clinical reactions occurred, children were dismissed after a period of 2-h observation, and parents were asked to come back to the hospital or call the physician as soon as any symptom occurred in the next 2 days, to assess late reactions. During the following week, the children performed both the fecal occult blood test (to detect a manifestation of cow's milk allergy) and a 2-weeks-later follow-up to evaluate other potential late reactions and SCORAD index. The test was assessed as positive if 1 or more of the following reactions occurred: urticaria, angioedema, wheezing, vomiting, diarrhea, shock, or exacerbation of the eczema (AD was considered to have been exacerbated if the SCORAD index increased of at least 10 points); symptoms within 2 h after administration of the last dose were considered as an early reaction, and symptoms occurring after more than 2 h were considered as a late reaction.
Statistics and predictive capacity
For the statistic analysis, we used SPSS for Windows (version 16.0). All the single tests and the combinations of them were compared to all the open oral food challenge results by making up cross tabs, and for each test we calculated the efficacy parameters: sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV).
The study was approved by the ethics committee and informed consent was obtained.
Results
The results of each allergological test for each patient are shown in Table 2.
Only the positive results for each test are shown. −indicates a negative test. When a food challenge resulted as positive, the type of reaction is indicated in brackets.
APT, atopy patch test; sIgE, serum immunoglobulin E; SPT, skin prick test.
Clinical outcomes of challenges
We analyzed a total of 40 open oral food challenges performed on 20 patients (20 for cow's milk and 20 for hen's egg): 8 results (20%) were positive and 32 (80%) were negative. Considering separately the challenges for the 2 foodstuff, only 1 test (5%) was positive for cow's milk and it was classified as an immediate reaction. Concerning hen's egg, 7 tests (35%) were assessed as positive; among them, 5 were classified as isolated immediate reactions, 1 as an isolated late reaction, and 1 as a mixed reaction. All children showed a good compliance to the oral challenges.
Outcomes of allergological tests
Among all the performed SPTs, 9 (22%) cases resulted as positive: 5 cases were positive for hen's egg, and 4 were positive for cow's milk. Concerning APTs, we recorded 21 (51.2%) positive tests: 12 were positive for hen's egg, and 9 for cow's milk. Twenty-one tests (51.2%) expressed specific IgE to the foodstuffs analyzed; of them, 12 were positive for hen's egg, and 9 were positive for cow's milk.
Concerning the single tests performances, SPTs were well tolerated by all the children. On the other hand, the measurement of sIgE was not user friendly, because it was difficult to perform when compared with other simple tests. All the APTs were easy to perform and had only the disadvantage that they had to be read after 48 h from the application of the tapes.
The performances of the allergological tests are reported in Tables 3 and 4.
PPV, positive predictive value; NPV, negative predictive value.
A, SPT+APT; B, SPT+sIgE; C, APT+sIgE.
Single test parameters
Considering the single tests, the SPT shows the highest specificity and the highest PPVs when compared with the APT and the sIgE measurement in our population. Further, it shows a very high NPV (90%). Concerning the APT and the sIgE measurement, our data show a very low PPV, the same NPV as that of the SPT, and the highest sensitivity.
Combined test parameters
Combining the APT with SPT shows an improvement in sensitivity in our population; on the other hand, specificity and PPVs remain very low. Further, APT combined with SPT shows the higher NPV (92%).
Discussion
Given the 40 open oral food challenges that we performed, 8 resulted as positive, showing a prevalence of food allergy caused by cow's milk and hen's egg in children with AD equal to 20% in the study population, which confirms previous studies. 4 As in our study we decided to test only the 2 food items that most frequently cause food allergy in Europe, we believe the prevalence could be even higher if we also considered peanuts, soy, wheat, and fish. Further, considering separately the challenges for the 2 foodstuffs, our data show that only 5% of those for cow's milk and 35% of those for hen's egg were positive, showing that food allergy to hen's egg is more common in our population.
We chose to perform an open oral food challenge instead of a double-blind one, because it is easier to perform and it can be appropriate and acceptable in young children with objective symptoms, as suggested by Bahna 24 ; further, bias due to psychological factors are minimal in the case of young children, even though they cannot be eliminated.
Concerning SPT and APT, we decided to use commercial standardized extracts instead of fresh food to avoid possible mistakes during the preparation (eg, errors in the concentration).
As the purposes of our study were to evaluate whether a test could render the oral food challenge superfluous and to minimize unnecessary investigations, we calculated sensitivity, specificity, PPV, and NPV for every option we considered (Tables 3 and 4).
Single test parameters
The better specificity and high PPV of SPT confirm previous investigations, but in our sample SPT shows a higher NPV. 25 Given a low PPV for the APT, it is possible to say that it is not useful in detecting food allergy in young children, as previously stated by Osterballe and Vanto,16,26 who both had a bigger population than ours. However, our results are partially in opposition to another study by Keskin, 27 who found a high PPV for the APT (89%), but he analyzed only cow's milk allergy. Considering the sIgE measurement, our data show the same values as for the APT, but in our experience we found that children were more compliant to APT, which, in our opinion, could be preferred.
As none of the tests has a high sensitivity or a high PPV, in our population there was no single test that could render the oral food challenge for cow's milk and hen's egg superfluous.
In our view, however, the high NPV of the 3 tests is also an important parameter, because the main aim in the diagnostic workup is to avoid unnecessary and sometimes harmful diets. Therefore, we believe that when the test results are negative, it could not be necessary to perform an oral food challenge, because the results provide a guidance in excluding the diagnosis of food allergy for the food item, especially considering also the clinical history of any single patient. However, considering that 1 patient in our sample population had a positive challenge with negative skin and blood testing (patient 8 on Table 2), up to 5% of false-negative results must be taken into account when performing and interpreting the tests.
Considering the performance values shown in Table 3 and the compliance, and knowing that SPT and sIgE measurement evaluate the same immunological mechanism, in our experience the SPT could be preferred to the sIgE measurement as an early diagnostic tool in the diagnostic workup of food allergy in young children with AD, because it showed a higher accuracy and appeared easier to perform in these patients. It is notable, however, that sometimes sIgE measurement is still needed, because it can be used to monitor a drop and it can aid in predicting a desensitization.
Combined test parameters
Our data show that none of the combinations can render oral food challenges for cow's milk and hen's egg superfluous for the diagnosis of food allergy in young children with AD, all having low PPVs.
However, the combination of the SPT with the APT improves the NPV (92%) in our population. We believe that this result can be explained, because both the IgE- and the cell-mediated immunological mechanisms at the base of the pathology could be evaluated using the combination of these 2 tests, even though there is a lack of consensus among experts about the proper performance of APT whose extract strength has been not yet validated.11,23 This result is in accordance with studies by Keskin, 27 and Isolauri, 28 who found that the combination of APT and SPT improves the predictive capacity of the single tests in patients with AD and suspected food allergy.
Even though a small number of patients were studied and open oral food challenges instead of double blind ones were performed, our data show that the combination of SPT and APT can be useful in the diagnostic workup of food allergy to cow's milk and hen's egg in young children with AD: first of all, an SPT should be performed, then an APT would be useful if the SPT resulted as negative or if the patient's clinical history suggested a cell-mediated pathogenetic mechanism; so, when both the SPT and the APT give a negative result, it could not be necessary to perform an oral food challenge, because it is highly probable that it would result as negative if it was performed (NPV: 92%). In our opinion, this is an important result, because in this kind of population it could permit to avoid unnecessary elimination diets and food challenges, lowering also the economic costs of the diagnostic process.
On the basis of our results, therefore, we propose a new working framework for the diagnostic workup of children with AD and suspected food allergy (Fig. 1).
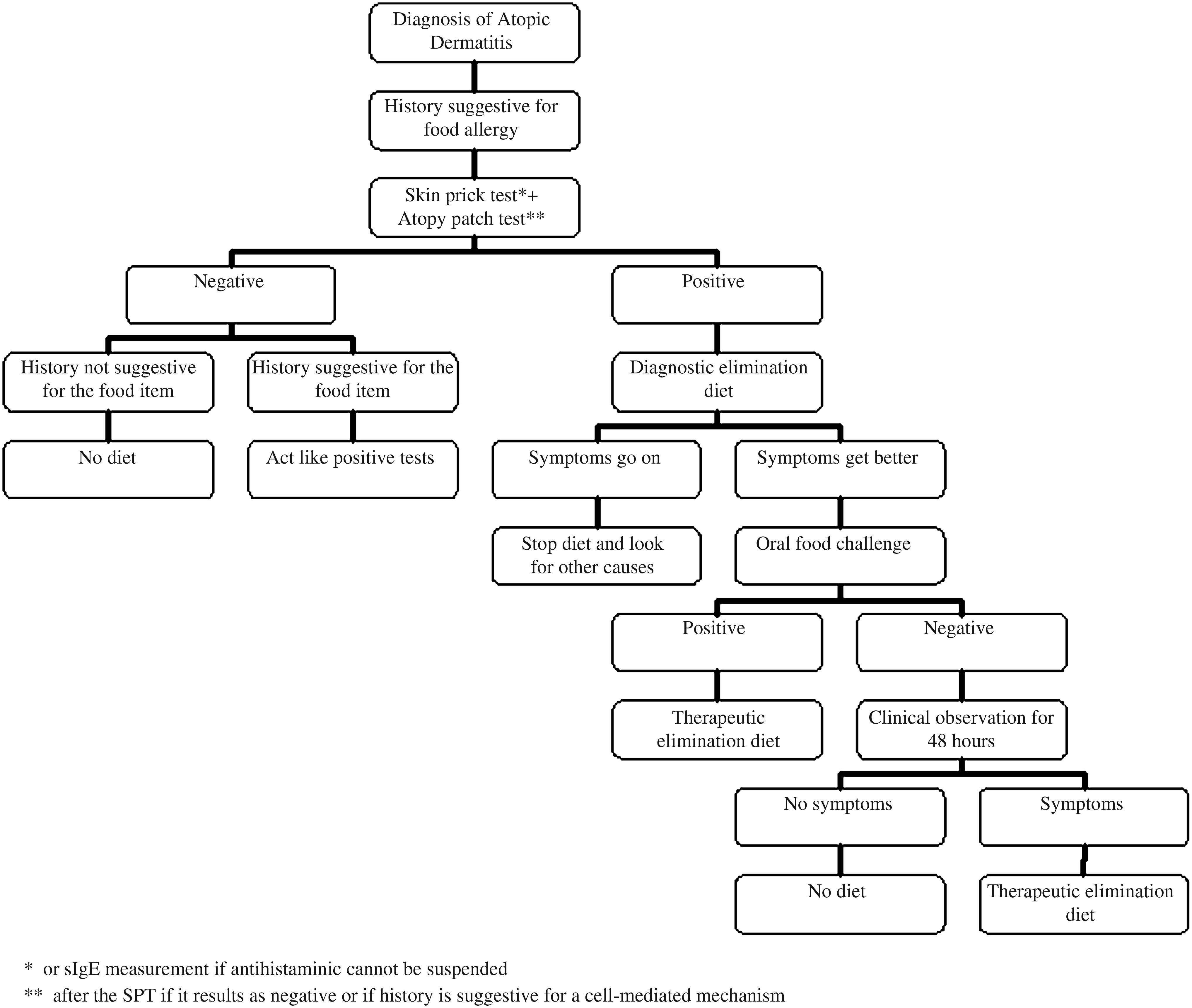
Working hypothesis for the diagnostic workup of children with atopic dermatitis and suspected food allergy.
Conclusion
Our results confirm that the food challenge is the gold standard for the diagnosis of food allergy in children with AD. However, as the combination of the APT with the SPT showed a very high NPV, we believe that this combination is useful when both tests are negative, because this result provides a guidance in excluding an allergy to the investigated food and could make the food challenge superfluous in this case, avoiding also unnecessary elimination diets. As a very small percentage of allergic patients could be missed considering only SPT and APT, however, we recommend to take the patients' clinical history into account and to go on performing the challenge when the suspicion of a food allergy remains very high although skin tests are negative.
We suggest further studies with a bigger population to better understand the usefulness of APT in the diagnostic process of AD with suspected food allergy.
Footnotes
Author Disclosure Statement
No competing financial interests exist for any of the authors.
This work was performed at the Department of Pediatrics, Legnano Hospital, Legnano, Milan, Italy.