
Abstract
Concurrent with improving survival in cystic fibrosis (CF), lung function has also steadily improved. Forced expiratory volume in one second (FEV1), the measure of airway obstruction most widely monitored in patients with CF, often does not fall below the normal range until late adolescence. Clearly, FEV1 is losing relevance for clinicians monitoring lung disease in children with CF, as it is frequently normal, declines slowly, and cannot be measured by conventional techniques in children <6 years of age. As clinicians increasingly aim to identify and treat early CF lung disease before irreversible structural airway damage occurs, there is a compelling need for better tools with which to monitor for early lung structural and physiologic abnormalities in our youngest CF patients. Three promising measures are infant and preschool lung function testing, chest computed tomography, and multiple breath washout measures of the lung clearance index. The current state of these tests as they relate to the clinical monitoring of early CF lung disease is reviewed, and improvements on the horizon that may allow them to be adopted in clinical practice explained.
Introduction
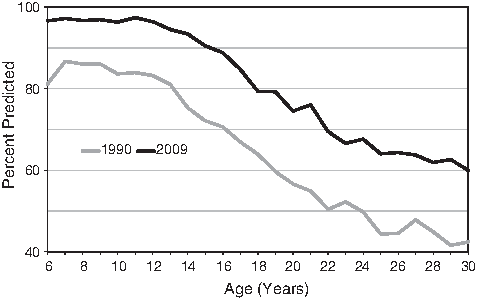
Lung function has dramatically improved over the past 2 decades (U.S. Cystic Fibrosis Foundation. 2009 Annual Report of the National Patient Registry. Bethseda, MD: 2009) There has been a greater than 10% improvement in median lung function (FEV1) in 2009 (black curve) compared with 1990 (grey curve) such that when first measured in school-aged children median FEV1 is within the normal range where it remains through the majority of childhood. FEV1, forced expiratory volume in 1 second.
Clearly, FEV1 is losing relevance for clinicians monitoring lung disease in young children with CF, as it is frequently normal, declines slowly,5,8 and cannot be measured by conventional techniques in children <6 years of age. There is a need to detect early signs of pulmonary disease, assess response to interventions and changes in clinical management, and monitor progress. The context of the early years of life is especially important as the lung is growing and developing rapidly during this period and may be particularly susceptible to insults. Pulmonary inflammation starts very early in CF4,12 and infections with common CF organisms such as Staphylococcus aureus and Pseudomonas aeruginosa usually have their onset in infancy or the first years of life. 13 As clinicians increasingly aim to identify and treat early CF lung disease before irreversible structural airway damage occurs, there is a compelling need for more sensitive tools with which to monitor for early lung structural and physiologic abnormalities in our youngest CF patients. 3 Three promising measures are infant and pre-school lung function testing, chest computed tomography (CT), and multiple breath washout (MBW) measures of the lung clearance index (LCI). Because of concerns regarding the expense, time, and intensive training required for infant lung function testing, exposure to radiation with CT scans, and the lack of validated commercially available MBW devices, these tests are currently limited largely to the research arena and not yet widely accepted for routine clinical use. However, each holds promise as a potential clinical tool in young patients with CF. The current state of these tests as they relate to the clinical monitoring of early CF lung disease is reviewed, and improvements on the horizon that may allow them to be adopted into clinical practice explained.
Infant and Preschool Lung Function
Early airway inflammation associated with infection leads to airway obstruction,14,15 ventilation inhomogeneity,16–18 air trapping, 14 and decline in lung function. 19 As evidence accumulates that lung disease begins early in CF, objective, physiologic measurements are required to diagnose and quantify early heterogeneous airway obstruction. No single lung function test exists that evaluates all physiologic components. Commercial equipment is currently available to measure forced expiratory flows, lung volumes, and ventilation inhomogeneity. Forced expiratory flows may be evaluated in sedated infants using the raised volume rapid thoracoabdominal compression technique (RVRTC). 20 Diminished values are associated with infection with P. aeruginosa, 21 S. aureus, 19 and lower airway inflammation.19,22 Although RVRTC values and lung volumes improve post-antibiotic therapy for a pulmonary exacerbation, flow limitation and air-trapping/hyperinflation have been reported to persist. 23 Many centers now use RVRTC routinely in infants with CF, where the identification of diminished lung function in minimally symptomatic infants is contributing to decisions to change clinical management. 24 The significant limitations are the requirement for sedation in infants, the expense of equipment, the technical demands of performing the tests, the time-consuming nature of the tests (2–3 h because of the need for sedation), and the increased demands for sensitivity given the generally milder lung disease present during infancy. In addition, limited reference data exist for the RVRTC, and have only been reported in 155 healthy infants. 25 Dependence on these published equations may lead to misinterpretation in both the research and clinical setting. 26 Despite these limitations, at least 100 centers perform infant pulmonary function testing worldwide, with at least two-thirds of these using the tests clinically rather than purely for research; the majority of these are performed to assess early lung disease in CF. 24 The importance of collecting suitable normative data is well recognized and groups are in the process of collecting such data from healthy infants and young children without CF.
Multiple studies have demonstrated the feasibility of performing preschool spirometry.17,27 In large observational studies, spirometric indices in preschool children differentiate the CF population from controls; however, overlap between these 2 groups is significant. Decline in lung function values has been reported during the preschool years. 28 Limitations of preschool spirometry include the need for expertise to achieve acceptable maneuvers in this age group and the inability of some children, especially 3- and 4-year-olds, to cooperate for testing. Multicenter experience suggests that if preschool spirometry is used as an endpoint in a clinical trial, a run-in period should be required to ensure acceptable individual data. 28 There are no data yet to suggest that incorporation of infant and preschool pulmonary function tests (PFTs) improves health outcomes for patients
Chest CT
In CF, chronic pulmonary inflammation and infection lead to bronchiectasis. In 90% of patients progressive structural destruction ultimately results in respiratory failure and death. Recent data highlight that bronchiectasis is already established by 8 years of age in the majority of children with CF. 11 In this prospective study in children who had been diagnosed clinically with CF, 51/60 (85%) had evidence of bronchiectasis on volumetric chest CT at a mean age of 7.8 years. Such changes can be missed by spirometry, which can remain normal even when significant and progressive bronchiectasis is present. 29 Therefore, using chest CT routinely to monitor lung disease in CF as an alternative to spirometry has been considered. 30
Recent studies have assessed the nature and onset of structural changes in infants and young children with CF. Gas-trapping, bronchial wall thickening, and even bronchiectasis are common in the first years of life. Long et al. obtained limited-slice high-resolution CT images of the chest in 34 children with CF (aged 10 weeks to 5.5 years) and 20 healthy disease controls without CF. Their study demonstrated that the airways of the CF cohort had thicker walls with more dilated lumens. Compared with airways from the healthy population, 94% of children with CF were reported to have at least 1 airway that was considered bronchiectatic. 31 Martinez et al. 32 performed limited-slice high-resolution chest CT in younger subjects with CF (8 months to 2.5 years) and found that children with CF had airways with thickened walls and narrower lumens compared with controls. It is unclear whether the observed airway wall thickening is a precursor of the findings of Long et al. in slightly older subjects, or indeed, of bronchiectasis as there are few longitudinal data. However, bronchiectasis can be identified by high-resolution chest CT even in the first few months of life 4 with 1 prospective population-based cohort study showing that the prevalence of bronchiectasis increased subsequently during the preschool years. 33 Structural changes on chest CT in young children with CF are associated with worse pulmonary inflammation and infection.4,33,34 Therefore, the potential utility of chest CT in the diagnosis and monitoring of structural changes in early CF lung disease in routine clinical practice is self-evident. However, a number of significant concerns currently limit the clinical role of chest CT in the early management of CF.
As children find it difficult to lie still and perform the necessary breathhold maneuvers required to obtain acceptable lung images, children <4 years of age undergoing chest CT usually require sedation or general anesthesia coupled with controlled ventilation strategies. This increases the risk and expense of the technique, increases the time required for the procedure (at least half a day for anesthesia and 1–2 h for sedation strategies), and decreases its acceptability to families of children with CF. Children with CF between 4 and 12 years old can, with appropriate instruction, reproducibly perform the respiratory maneuvers required to acquire high-quality chest CT images. 35 A greater limitation is the concern about the long-term risks of radiation exposure. However, some of these limitations may at least partly be mitigated by recent developments and improvements in CT technology.
New multi-detector CT scanners with dual-energy and/or dual-source capabilities were introduced in 2005 36 and are beginning to replace conventional scanners in several centers. Dual-source CT scanners are equipped with 2 X-ray tubes and corresponding detectors that are mounted onto the rotating gantry at 90° angles. Therefore, only a 90° gantry rotation is necessary to collect 180° of projection data. 37 These scanners have the potential for much faster scanning protocols requiring shorter breathhold strategies as they provide a full CT slice in only half a rotation. The latest technology already enables cardiac imaging in less than 0.3 s and is capable of scanning an infant's chest (<150 mm) in 1 sub-second rotation. In the future, such developments are likely to permit imaging in more infants and young children without the need for sedation or general anesthesia.
Children are at increased risk from unattenuated CT radiation doses as their smaller cross section is associated with a larger, actually absorbed radiation dose. Best practice when setting scanning protocols in pediatric imaging is therefore to always consider the ALARA principle (As Low As Reasonably Possible). 38 Even with existing scanners, it is feasible to perform full volumetric CT with significantly reduced radiation exposure (mean effective dose in infants of less than 1 mSV compared with a chest x-ray mean effective dose of 0.05–0.1 mSV) if scanning protocols are adapted to the anatomy of infants and young children.37,38 Decreasing the tube current (to decrease the number of X-rays produced by the anode filament of the scanner), the tube voltage (to decrease the energy of the X-rays produced by the anode filament), increasing the pitch (the speed of the table passing through the scanner's gantry), 39 using pre-patient filters to eliminate non-image forming radiation energies from the primary beam and decreasing overlap in X-ray beams that occur at the start and end of the helical acquisition (“over-beaming”) are all possible while maintaining optimized contrast in relation to noise of the images obtained. 40
The newer dual-energy source scanners permit significantly faster scanning while maintaining image quality and will enhance efforts to reduce effective radiation dose further and potentially lower than 0.5 mSV for a full volumetric inspiratory scan (approximately 50% of the radiation dose of scanners used currently in most pediatric hospitals). New scanners incorporate software that maximize contrast-to-noise ratios, which can also contribute to dose reduction. 37 Whether or not such developments result in increased clinical utility of chest CT scanning in young children with CF remains to be seen.
While chest CT remains the gold-standard radiological technique to identify bronchiectasis, and can also be used to identify gas-trapping and bronchial wall thickening (although the inter-observer repeatability in determining the latter in preschool children appears to be poor 33 ), efforts to provide surrogate markers of structural changes without the associated risks are ongoing. One proposed alternative is magnetic resonance imaging of the chest (either alone or in combination with hyperpolarized gases to provide complementary information on peripheral lung function), but there are few data in infants and young children. In terms of lung function surrogates for structural lung changes, multiple breath inert gas washout does appear to provide information that is significantly associated with lung structure (at least in school-aged children with CF) and has been proposed as a sensitive surrogate for structural lung damage.10,11,41
Multiple Breath Washout
Since emptying of gas from unobstructed lung units can compensate for diminished emptying from obstructed lung units (a concept termed kinematic interdependence of lung emptying), 42 forced expiratory flows may theoretically be insensitive to early, heterogeneous lung disease. MBW techniques measure ventilation inhomogeneity during tidal breathing and the indices that can be measured are not affected by kinematic interdependence, depending instead on regional changes. MBW measurements are therefore exciting novel tests that have the potential to detect early heterogeneous airway obstruction in CF. Commercial equipment uses either a mainstream or a side-stream ultrasonic flow meter to measure gas concentration via molar mass, usually set up to detect changes in concentration of the inert gas sulfur hexafluoride (SF6). The test involves determining the efficiency of expiring the test gas, usually SF6, from the lungs. Unlike infant and preschool spirometry, the commercially available equipment has not yet been fully validated. Another limitation is lack of standardization of this technique. Also, the technique generally requires sedation between about 2 months and 2 years of age. Performance of MBW (triplicate measurements) takes 30 to 60 min in a cooperative child, and up to 2 h in an infant requiring sedation. Measurements are feasible in children less than 2 months without sedation but take 1–2 h because of the requirement for the infant to sleep for the tests.
The most common index to assess using MBW is the LCI, a measure reflecting the number of tidal breaths, or lung volume turnover, needed to clear the inert gas from the lungs. Therefore, LCI is defined as the quotient of the total volume exhaled during the washout phase divided by the functional residual capacity (FRC). Since LCI reflects ventilation inhomogeneity, it is directly related to the severity of airflow limitation: children with more severe airflow limitation have higher LCI values. In pre-school children 17 and school-aged children, 10 LCI has proven to be more sensitive than spirometry at detecting early lung disease in CF. However, in the only published study during infancy, RVRTC and MBW detected abnormalities in different individuals and MBW was not clearly superior to RVRTC. 43
Recent studies evaluating MBW as a surrogate for structural airway damage detected by CT have been favorable.10,11 In a recent study, high resolution CT abnormalities correlated more strongly with LCI compared with spirometry in school-aged children. These same investigators reported that 84% of subjects with CF had abnormal LCI, whereas only 58% and 47% had abnormal FRC values and spirometric indices, respectively. 11 More studies are needed comparing lung structure and ventilation inhomogeneity to help validate the tool. Data are especially needed in younger subjects assessed from diagnosis to see how measurements from MBW evolve over time and how they are related to assessments of structural changes in longitudinal studies.
Finally, MBW has been used as an outcome measure in 2 trials assessing the efficacy of hypertonic saline and recombinant DNase in school-aged children with CF.44,45 These studies revealed that in children with CF receiving either hypertonic saline or DNase LCI values improved compared with the placebo group. In fact, subjects that received hypertonic saline had an improvement in LCI, but no improvement in spirometric indices, 45 suggesting that LCI had greater ability to detect change in physiologic measures. Pilot studies such as these are critical to validate the use of MBW as an outcome measure during therapeutic interventions.
Conclusions and Future Directions
As we improve our understanding of the early onset of inflammation, infection, airflow limitation, and structural airway damage in CF, we are recognizing increasingly the need for earlier interventions and new treatment paradigms in infancy and the preschool years. The quest continues for the optimal clinical tests with which to monitor both airway function and structure in infants and young children with CF. Although not currently in widespread clinical use, infant and pre-school lung function testing, chest CT, and multiple breath inert gas washout all hold promise for the early detection of abnormalities and response to treatment. Measurements of airflow obstruction and gas trapping from infant and preschool lung function testing may be more sensitive to early airway obstruction than FEV1 from conventional spirometry, but better reference equations are needed. CT is the gold standard for evaluating structural airway damage, and concerns regarding radiation exposure may be reduced in the future by low-dose protocols made possible with newer scanners. MBW measurements appear promising as potential radiation-free surrogates for the identification of structural airway damage, but standardization of techniques and commercial equipment are needed.
Areas for future research and development include the development of more robust reference equations for infant pulmonary lung functions tests, reduction in radiation exposure associated with CT scans through improved algorithms and scanners, and development of a commercial MBW device that yields measurements comparable to the gold standard and that can be used to measure lung function throughout the important early years of life. Automated CT scoring systems for clinical use would allow standardization of the assessment of bronchiectasis, airway wall thickening, and gas trapping, enabling improved diagnosis and monitoring. A better understanding of the longitudinal associations between structure, forced flows, and ventilation inhomogeneity across the ages is required. In addition, further evaluation of the response to treatment of MBW, CT scans, and infant and preschool lung function is also needed. Such advances will hopefully allow the eventual incorporation of these modalities into clinical care to improve outcomes in our youngest patients with CF.
Footnotes
Acknowledgment
We acknowledge the help of Ms. Fiona Ramanauskas in the preparation of this article.
Author Disclosure Statement
S.R. has no conflicts of interest to declare; S.D. has no conflicts of interest to declare; M.R. has no conflicts of interest to declare.