
Abstract
Disorders of the chest wall, spine, and respiratory muscles lead to lung function abnormalities consistent with restrictive lung disease. Common disorders of the thorax include diseases with respiratory muscle weakness, growth abnormalities of the thorax and spine, such as scoliosis. Spirometry alone is not sufficient to diagnose these abnormalities but may be useful to serially monitor changes over time or in response to treatments. In contrast, obesity does not produce restrictive respiratory disease in most children and produces obstructive lung disease more often. Test of respiratory muscle function, breathing during sleep, and during exercise have led to additional insights about the pathophysiology of these conditions that may provide new avenues for future therapies.
Introduction
The purpose of this article is to address the utility of pediatric lung function testing methods in diagnosing and assessing the severity of restrictive respiratory disease among patients and longitudinally in individual patients. Lung functions include those measured in the pulmonary function laboratory, the outpatient office setting, the exercise laboratory, and the sleep center. This review is limited to disorders of the chest wall, including spine deformities and disorders of the respiratory muscles, such as neuromuscular weakness. The lung function abnormalities reported in obese children as they relate to restrictive changes in mechanics are also reviewed.
This, however, is an over-simplified approach to these clinical disorders insofar as they overlap. Neuromuscular syndromes are often associated with scoliosis and also obesity. Scoliosis occurs in 95% of children with Duchenne muscular dystrophy, and 50% and almost 100% in patients with type III and type II spinal muscular atrophy respectively. 2 Children with primary chest wall disorders may be significantly underweight and malnourished, influencing both respiratory and other skeletal muscles, which, in turn, influence lung functions at rest and during exercise. 3 Obesity predisposes children to upper airway disease during sleep and asthma.4–7 The overlapping influences of these disorders on respiratory function are beyond the scope of this article. Similarly, patients with disorders of the thorax may also have co-morbid conditions, such as recurrent aspiration or atelectasis, among children with neuromuscular weakness and ineffective cough. This article assumes that the lung function abnormalities described are due to chest wall disorders alone without complicating co-morbidities.
Limitations of Spirometry
Reduced TLC is the recognized gold standard to establish restrictive respiratory disease. This is measured using either gas dilution methods or body plethysmography. However, in many clinical settings, measurement of TLC is impractical and cumbersome. Equipment to make these measurements exists in lung function laboratories often located far from outpatient care settings. Can spirometry be used alone to diagnose restrictive lung disease? Several retrospective analyses of lung functions from adults demonstrate that a normal forced vital capacity (FVC) has a high negative predictive value in ruling out restrictive lung disease.8–10 However, diminished FVC alone had a low sensitivity and specificity in predicting restrictive lung disease when compared with concurrent measurements of TLC. 8 The use of low values of FVC in association with a normal FEV1/FVC ratio improves sensitivity compared with reduced vital capacity alone, but the positive predictive value of this combination of spirometric findings only ranges from 58% to 64%.8,10 The lower the value of FVC, for example, <60% predicted in men and <50% predicted in women, the more sensitively this combination of FVC and FEV1/FVC indicates restrictive disease. 9 Therefore, spirometry is more useful in monitoring the changes in lung function over time, than as the sole means of diagnosing restrictive respiratory disease.
Lung Function Testing in Children with Neuromuscular Disease
“Neuromuscular disease” encompasses a gamut of conditions ranging from weakness to spasticity, and from selective muscle involvement, which may spare some respiratory muscles to generalized myopathies. They can be congenital or acquired and can also be persistent or progressive. This article is focused on disorders of generalized muscle weakness.
Respiratory muscle weakness reduces the inspiratory force that can be generated during inspiration and the force generated during exhalation during a vital capacity maneuver or cough. FVC is, therefore, reduced due to weakness of both inspiratory and expiratory muscles. In contrast, residual volume (RV) may be almost normal as the ability to exhale completely is reduced with expiratory muscle weakness. TLC is reduced due to the diminished FVC. However, the RV/TLC is normal or increased due to incomplete exhalation as the result of expiratory muscle weakness or a stiff chest wall rather than trapped air due to airway closure. FEV1 is reduced commensurate with the reduced FVC, and FEV1/FVC is normal. If the chest wall collapses on itself, due to thoracic muscle weakness, as illustrated in Fig. 1, then RV can decline more dramatically due to loss of intra-thoracic volume.

Chest wall shape in a child with spinal muscular atrophy with reduced lung volumes.
Direct measurement of respiratory muscle force will help clarify this spirometric pattern, given the caveat that measures of maximum inspiratory and expiratory pressures (MIP and MEP) depend on technique and effort. In addition, children with weak facial muscles may have difficulty maintaining a closed seal around the mouthpiece when attempting these maneuvers. The norms for MIP and MEP have wide ranges and are both age and gender specific.11–15 MIP values among weak children are also sensitive to position, and some authors have suggested measurements of MIP in the supine position as a more sensitive way to detect diaphragmatic weakness. An alternative measure of inspiratory muscle strength is the sniff maneuver with pressures measured from one naris during maximal sniffing, whereas the other naris is occluded. Norms for this testing procedure differ from MIP values but also exist for children. 16 Finally, MIP and MEPs have been measured by airway occlusion during crying in 100 normal infants, and this method has been used to detect infants with respiratory muscle weakness.17,18
With involvement of expiratory muscles, cough force is compromised and peak cough-generated flows are reduced. There are norms for the latter that indirectly measure expiratory muscle strength without using an occluded device and may be more tolerable for patients to perform. 19
Hypercapnea occurs initially during sleep in children with respiratory muscle weakness and may be first present in rapid eye movement sleep when intercostal and upper airway muscles lose tone. Where polysomnography (PSG) is not readily available, overnight studies of oxy-hemoglobin saturation using pulse oximetry may identify children at risk for sleep-related hypoventilation. Alternatively, measurements of SaO2 combined with transcutaneous carbon dioxide or end-tidal CO2 measurements using capnography may distinguish which patients will benefit from supplemental oxygen and which should use positive pressure ventilatory support during sleep.
Longitudinal assessment of respiratory function is part of the standard of care in children with neuromuscular diseases. Though not always based on strong data, several sensible consensus statements have been published in recent years.20–22 These are based on several reports that study different combinations of patients with different neuromuscular disorders, variable degrees of scoliosis, different proportions who were treated surgically for scoliosis, some with cardiomyopathy, and different study designs.23–28 Routine measurements of lung function during wakefulness in children with neuromuscular diseases include spirometry, MIP and MEP, peak cough flow, pulse oximetry, and end-tidal or capillary blood PCO2. PSGs should be performed when overnight SaO2 and PetCO2 values are not diagnostic in the presence of symptoms suggestive of sleep-disordered breathing. PSGs can detect episodic or persistent hypoventilation due to both respiratory muscle weakness and pharyngeal obstruction due to pharyngeal muscle weakness and/or obesity. PSGs may also detect episodes of hypoxemia independent of hypercapnia due to either a low functional residual capacity (FRC) that falls below airway closing volume or poor response to upper airway narrowing during sleep. Lastly, PSGs are useful to initiate and titrate levels of noninvasive positive pressure ventilation to assure that both sleep quality and gas exchange indices improve with treatment.
A relationship between decreased FVC and nocturnal alveolar hypoventilation has been reported for Duchenne muscular dystrophy, which is characterized by progressive respiratory muscle weakness. Although FVC between 40% and 60% of predicted norms indicates a low risk of nocturnal hypoventilation, FVC <40% predicted bears a significant risk of nocturnal hypoventilation, and FVC <20% is generally accompanied by both nocturnal and daytime hypoventilation. Peak cough flow values under 160–270 L/min in older teenagers and adults indicate ineffective cough and place patients at risk of recurrent respiratory infections and respiratory failure; corresponding values are currently unclear in children, despite publication of normal values. 19 These thresholds may not pertain to children with SMA II, who maintain functional status despite lower levels of FVC than children with muscular dystrophy. 26 In addition, these thresholds are higher than those predicting when a child with neuromuscular disease requires daytime ventilatory support as they transition from sleep-related hypercapnea to respiratory failure both day and night.23–28
Spine and Chest Wall Disorders
Diseases of the thorax involve the spine, ribs, and sternum and produce a continuum of restrictive respiratory disease. Airway obstruction can occur but is uncommon. In patients with scoliosis, rotation of the chest can produce compression of a mainstem bronchus against vertebral and mediastinal structures and reduce expiratory flows. Thoracic deformities produce several distinct phenotypes. Hypoplastic thoraces, as seen in asphyxiating thoracic dystrophy and spondylocostal dysostosis, primarily manifest as small volumes of the thorax and lungs. Chest wall compliance has not been reported in these conditions, but respiratory failure and death are common if no interventions are provided.29,30 In contrast, children with absent ribs due to congenital deformities or surgical resection of tumors have a flail chest and unstable chest wall, which is mobile but retracts into the chest with inspiratory efforts. Most common are children with early onset scoliosis with or without vertebral and rib anomalies that cause progressive spine deformity as they grow. Some authors have described all of these disorders together as Thoracic Insufficiency Syndrome. 31
Restrictive mechanical features develop principally due to decreased chest wall compliance. 32 FVC is reduced not only because of reduced intrathoracic volume but also due to decreased chest wall and diaphragmatic excursion. 33 All parts of the thorax, including the diaphragm and costo-vertebral joints, become less mobile with severe thoracic deformity. Both FRC and RV are diminished but less so that FVC as the stiff chest wall maintains a static configuration during expiration as well, preserving the RV despite forced expiratory efforts by the patient. TLC is diminished due to the larger reduction in FVC relative to RV, and RV/TLC is often elevated as a result.34–36
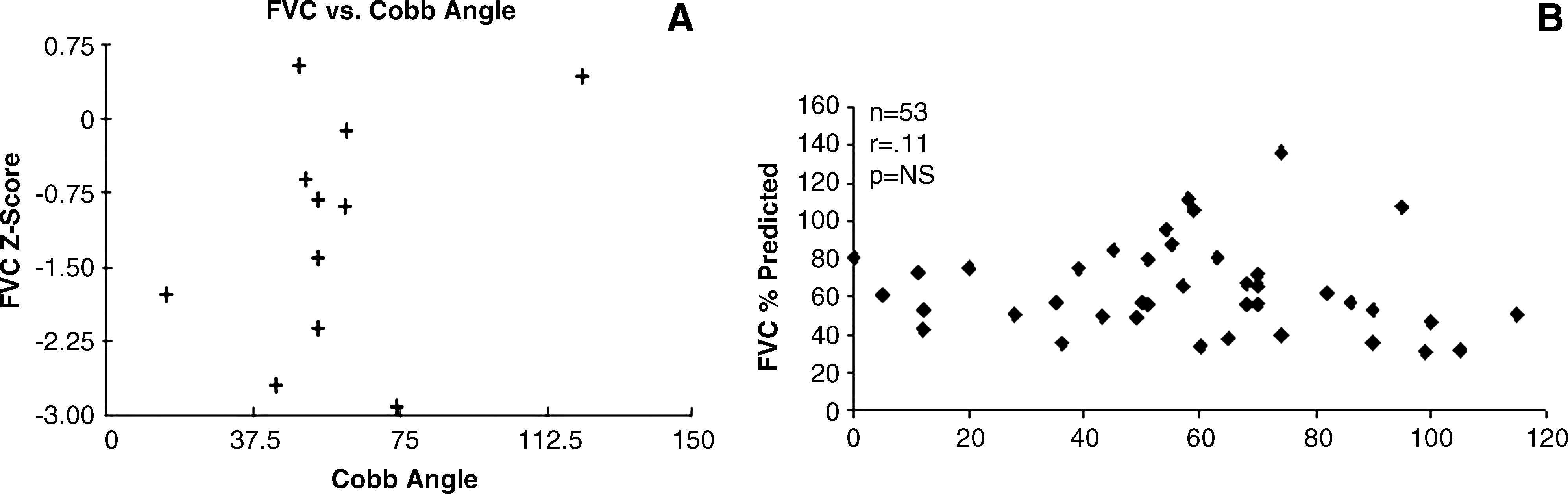
Reports of lung functions using standard spirometry and also the raised volume rapid compression method in infants describe variable degrees of restrictive findings. The functional abnormalities do not correlate with simple structural measures of scoliosis, such as the Cobb angle in either infants or older children34,37 (Fig. 2) Chest wall and spine deformities lead to scoliosis, kyphosis, lordosis, and thoracic rotation with abnormal rib angulation and motion. All of these features may occur at high or low vertebral levels and involve different numbers of vertebrae. Each 3-dimensional deformity can be reconstructed using multiplanar imaging but does not predictably reflect respiratory functional abnormalities. Consequently, measures of respiratory function cannot be surmised from structural features on imaging studies, and pulmonary function tests should be used to provide complementary information to make clinical decisions about progression and about treatment.
As the chest wall stiffens, inspiration becomes increasingly dependent on the diaphragm. In kyphoscoliosis, diaphragm excursion is diminished, and MIP may also be reduced. Respiratory muscle “weakness” occurs because of abnormal configuration of the diaphragm rather than a primary myopathy per se. There is a crude but significant correlation between MIP and FVC in adolescent idiopathic scoliosis (AIS), as illustrated in Fig. 3. 3 MEP may also be low due to the volume dependence of this measurement. MEP is low in proportion to reduction in TLC, the lung volume from which MEP is measured, rather than because of primary expiratory muscle weakness.
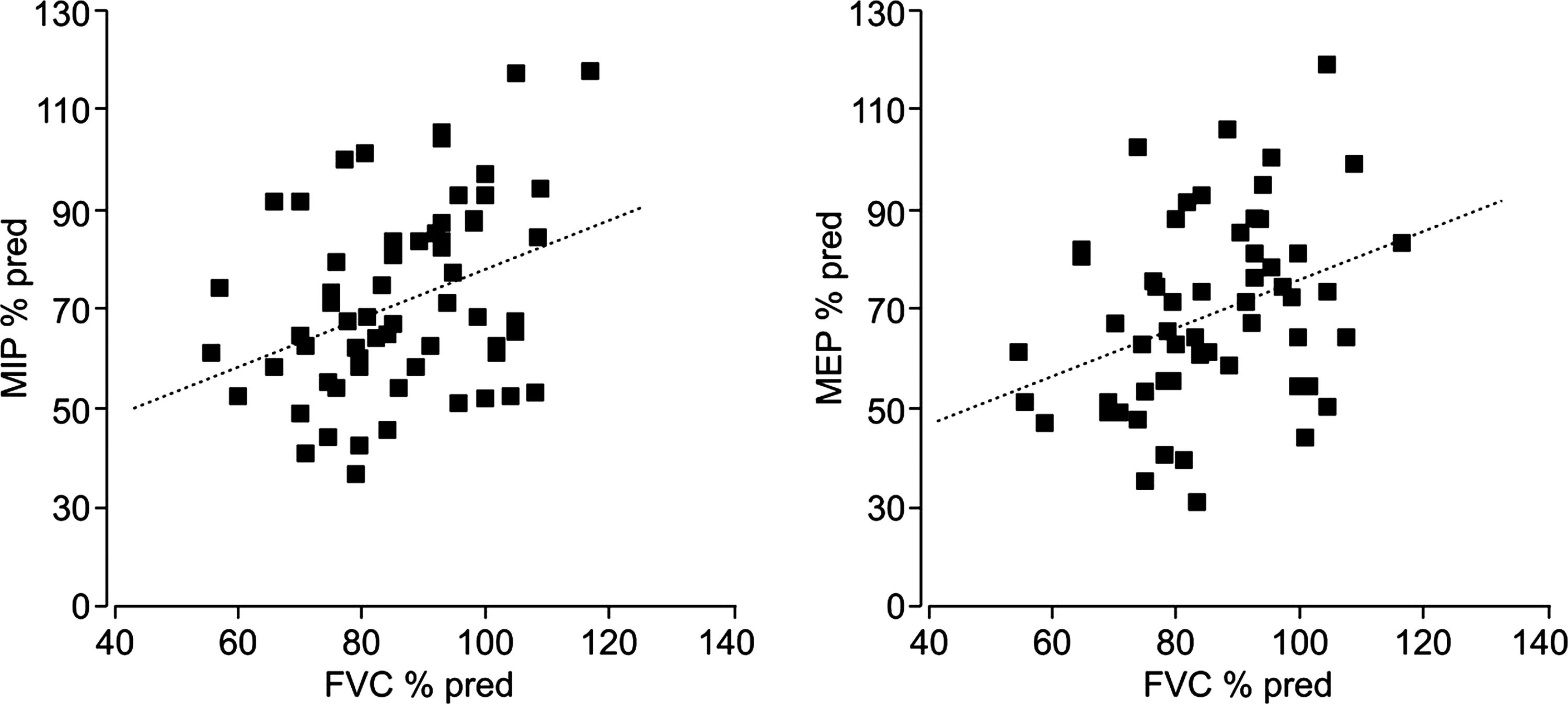
Relation of Maximum Inspiratory Pressure (MIP) to FVC in adolescents with idiopathic scoliosis. 3
Serial lung function testing has been useful to assess orthopedic surgical treatments for scoliosis. Long term follow-up of children undergoing spine fusion at an early age has demonstrated severe restrictive changes related to age of the fusion and length of spine that was fused. 13 Measurements of compliance and vital capacity over a 3 year period in 24 patients who underwent implantation and serial expansion of vertical expandible prosthetic “growing” titanium ribs demonstrated continued increase in absolute volumes of vital capacity but slightly reduced vital capacity as a percentage of predicted norms over time. Vital capacities are usually corrected for arm span to normalize for percent predicted values and to account for growth of the child. The same study demonstrated a 45% reduction in total respiratory compliance over the 3-year period, raising the question whether the titanium rib implants further stiffened the chest wall. 32 Total Respiratory Compliance measurements in this study were performed with passive inflation in the operating room under anesthesia. Compliance measures in awake children using esophageal balloons to measure pleural pressures and partition changes in lung versus chest wall compliance over time have not yet been reported.
Imaging has also been used to describe regional lung function in spine and thoracic cage disorders. A limitation of pulmonary function testing is that it is a summative measurement of the respiratory system and insensitive to changes in one hemithorax compared with the other. Uniplanar and multiplanar radiographic imaging do not provide regional volumetric information, but this can be obtained from 3-dimensional reconstructions of the lungs using computerized tomography and reconstruction software. 38 The images are usually created at FRC and not routinely at other controlled lung volumes. Extrapolations of lung volumes alone, however, do not address the regional dynamics of breathing. Instead, lung scans using radio-labeled isotopes may identify and quantify which lung contributes most to ventilation and perfusion and, therefore, guide surgical approaches. 39
More recently, gated images of diaphragm and chest wall positions with dynamic magnetic resonance imaging have been used to describe relative excursion of different components of the thorax both at tidal breathing and at TLC. One issue yet to be addressed is how change in posture alters breathing. Computed tomography, magnetic resonance imaging, and lung scan imaging are performed with the patient supine, whereas spirometry and muscle function testing in older children are performed in the upright position.
Responses to exercise have been described in older children with AIS. In general, in children with moderate degrees of spine deformity (Cobb angles >40 degrees), work capacity is mildly reduced, heart rate is higher per work load, and ventilatory reserve is reduced in some but not all patients.3,40 One study noted that reduced muscle strength, involving both the respiratory muscles and also the quadriceps muscles, correlated with reduced work capacity. Exercise was terminated due to leg discomfort rather than dyspnea. 3 The authors ascribed limitations in exercise to cardiopulmonary limitations, deconditioning, and also to muscle weakness.3,40,41 Muscle weakness in AIS has been attributed to poor nutritional status in the adolescents with moderate to severe scoliosis. Restrictive respiratory mechanics appear to contribute but not solely explain exercise limitations in these adolescents.
Disordered breathing during sleep has been described in children with early onset scoliosis in the absence of neuromuscular weakness. In one small study, the Apnea-Hypopnea Index (AHI) was abnormal in 14 of 15 patients, but the AHI was not explained by apneic events. 42 Instead, hypopneic episodes associated with oxy-hemoglobin desaturation and arousals were common and occurred more frequently in rapid eye movement sleep than in other sleep stages. The authors postulated that low lung volumes typical of thoracic cage deformities predisposed children to oxy-hemoglobin desaturation when hypopnea occurs. In another report, the serum hemoglobin level of 138 children with early onset scoliosis was >2 standard deviations above normal in 23% of those studied and improved after surgical intervention. The authors speculated that this was due to sleep-related hypoxemia that improved after surgical correction. 43 Currently, there is no consensus as to when PSGs should be ordered in this group of patients; larger case series are needed to determine the structural features and respiratory functional indices that suggest sleep-related breathing disorders are likely to exist.
Childhood Obesity
The emergence of obesity in childhood has been dramatic, and recent prevalence estimates are that 31%–42% of children in the United States are overweight or obese.44,45 Obesity predisposes children to several physiologic abnormalities, including sleep disordered breathing and a predisposition to airway hyper-reactivity and asthma.6,46,47 “Obesity” has been defined in various ways, using percent of ideal body weight, weight for height adjusted for age, or body mass index (BMI) and different thresholds to define obesity. In many cases, reports have included small numbers of children and have measured different combinations of lung function.
The types of abnormalities in lung function among obese children vary from study to study. Most importantly, lung function using spirometry and body plethysmography is normal in the majority of obese children. (373 children from 7 studies).5,6,48–53 The most common evidence of restrictive changes was a reduced FRC (<80% predicted) in 44% of 129 children.5,51,52 FVC was reduced in only 11% of 112 patients, but correlations with normal FEV1/FVC to better identify restrictive abnormalities were not reported.48,51–53 Airway obstruction is also common among obese children. Reduced expiratory flows (FEV1, FEV1/FVC, or FEF 25%–75%VC) occurred in 31% of 231 obese children.5,6,48,51–53 Increased airway resistance (>200% predicted value) using the interruptor method was described in 83% of 54 obese children. 52 Thirty-three percent of 67 obese children were also found to have a reduced lung diffusion capacity (<80% predicted after volume lung volume corrections), but these findings were not correlated with restrictive or obstructive lung function abnormalities.51,52
In multiple reports, lung function abnormalities do not correlate with quantitative estimates of obesity, for example, BMI.5,48,52 However, in one series of 300 obese children, increasing BMI was an independent predictor of reduced FVC, FEV1/FVC, and FEF 25%–75%vc, accounting for decrements of 2%, 5%, and 7%, respectively, compared with normal children. 7 This study, unlike the others, did not exclude children on enrollment with known lung disease, such as asthma. Waist to hip ratios, used to describe the distribution of adiposity, also did not correlate with pulmonary function values in 2 studies of obese but otherwise normal children. 48 The pediatric findings differ from obese adults where both BMI and waist to hip ratios correlate with reductions in lung volumes. 54 The literature currently does not include predictors as to which obese children will have restrictive respiratory disease, who will have obstructive lung disease, and who will be normal.
Footnotes
Acknowledgments
We thank Ms. Holly Kaopuiki for assistance with preparation of the manuscript and figures.
Author Disclosure Statement
The authors of this article have the following financial relationships to declare:
G.J. Redding: Speaker fees from Synthes Inc.
O.H. Mayer: No competing financial interests exist.
J.-P. Praud: No competing financial interests exist.