
Abstract
Asthma is responsible for significant healthcare costs in the United States. Although advances in pharmacology and environmental science have provided many opportunities to improve asthma control, asthma remains a major cause of missed school days, acute care visits, and hospitalizations. Patient education is a key component of asthma care. The National Asthma Educator Certification Board was established in February 2000 and charged with the mission of “promoting optimal asthma management and quality of life for individuals with asthma, their families and communities by advancing excellence in asthma education through the certified asthma educator process.” This study was performed to describe the workforce of certified asthma educators (AE-Cs®) by surveying a sample of educators who completed the recertification process. AE-Cs® who had completed the recertification process were invited to participate in an anonymous online survey. Sixty five of 135 (48%) recertificants completed the survey. The primary training of respondents was in respiratory therapy (51.6%) and nursing (42.2%). Respondents were primarily female (92.3%) and Caucasian (95.4%). The majority worked in specialty care outpatient (59.3%) or hospital inpatient (40.7%) settings. Twenty percent reported an increase in job responsibilities as a result of achieving their initial certification as an AE-C®. Most AE-Cs® have their basic training in either respiratory therapy or nursing. The workforce of AE-Cs® does not reflect the racial or ethnic percentages seen in the asthma population in the United States. More educators are needed to serve the growing numbers of individuals with asthma. Achievement of certification as an AE-C® resulted in additional job responsibilities in 20% of survey respondents.
Introduction
Effective asthma education is aimed at promoting a therapeutic partnership between patients and their providers. Coffman et al. 8 showed reductions in mean number of emergency department visits and hospitalizations following intervention in their meta-analysis of 37 pediatric asthma education programs. Karnick et al. 9 found that asthma education in inner-city children with asthma not only enhanced the health of children with asthma but also resulted in cost savings during a 1-year postintervention follow-up. Despite the success of individual projects over the short term, additional studies are warranted to evaluate key educational messages and the long-term health and cost outcomes of various educational interventions.
The National Asthma Education and Prevention Program (NAEPP) periodically reviews and updates asthma science, programming, and best practices. 10 These reports, now in their third edition, highlight the importance of education in improving awareness and promoting self-management for patients with asthma.
The creation of the National Asthma Educator Certification Board (NAECB) followed the 1999 Consensus conference of stakeholders involved in asthma education. The NAECB is an autonomous board, independent and separate from any other organization or association. Its charge was the creation of a certifying examination that would establish standards of excellence in asthma education and would integrate the knowledge and skills of a diverse provider workforce while adhering to the NAEPP Expert Panel Guidelines on the Diagnosis and Management of Asthma. This group, now beginning its 10th year, continues to grow and evolve as it invests in its mission “to promote optimal asthma management and quality of life among individuals with asthma, their families and communities through the certified asthma educator (AE-C®) process.” 11 The AE-C® credential is conferred only by the NAECB, a national, nongovernmental, not-for-profit certifying organization. Certification is valid for a period of 7 years and a voluntary registry of certificants is available online.
The NAECB was established in February 2000 and offered the first certification examination in 2002. Healthcare professionals in nursing, respiratory therapy, pharmacy, social work, and medicine were eligible to sit for the examination. Community health educators, physical and occupational therapists, social workers, and those with documentation of 1,000 hours of patient-level asthma educational experience were also invited to apply. The candidate handbook, available on the NAECB website, provides specific information for all eligible candidates who wish to prepare for the examination and includes a detailed content outline for the certification examination. 11
As of September 2010, a total of 5,041 applicants have applied and taken the examination, with a mean pass rate of 68.5% for first-time test takers and 67.8% overall for all test takers (first time, repeat, and recredential). At the present time there are 3,415 AE-Cs® in the United States. 11
As the NAECB approaches its 10-year mark, this project was undertaken to describe the workforce of AE-Cs®, to identify how and where AE-Cs® were being utilized within various healthcare systems and to identify benefits to the AE-C® credential. Because of difficulties contacting participants whose contact information had changed over the 8-year period from the initial certification, we opted to start our study with those beginning the recertification process in 2010. This survey was approved by the executive and research committees of the NAECB.
Methods
All recertificants were invited to participate in an anonymous, voluntary online survey designed to answer the following questions:
1. Which healthcare professionals seek out the AE-C® credential? 2. Do AE-Cs® tend to make this choice soon after graduation from their respective disciplines or is it chosen by those who have experience in the work place? 3. Do AE-Cs® represent the demographics of the population they serve—gender, race, urban versus suburban/rural? 4. Do AE-Cs® have direct personal or family experience with asthma? 5. What are the major job responsibilities and functions of an AE-C®? 6. Has the AE-C® credential influenced job responsibilities, salaries, and/or the ability to apply for reimbursement for asthma education services? 7. What do AE-Cs® themselves perceive as the greatest benefits from obtaining the credential?
The national database of AE-Cs® and U.S. census data 12 were utilized to calculate the ratios of AE-Cs® to asthma population by state. The 10 most and least populated states were used to make the comparison.
Results
Sixty five of 135 recertificants responded to our survey, providing a 48% response rate. The majority of AE-Cs® had their primary training in either respiratory therapy (51.6%) or nursing (42.2%). Primary training in pharmacy was reported by 1.6%, in community health by 1.6%, and in other by 3.1%. The breakdown is displayed in Fig. 1. Because of the variability that exists within the categories of both nursing and community health, we asked about the last year of school completed and found that 98.4% had completed at least 2 years of college level training. Those with a Master's level degree or higher comprised 31.4% of the group, as a whole.
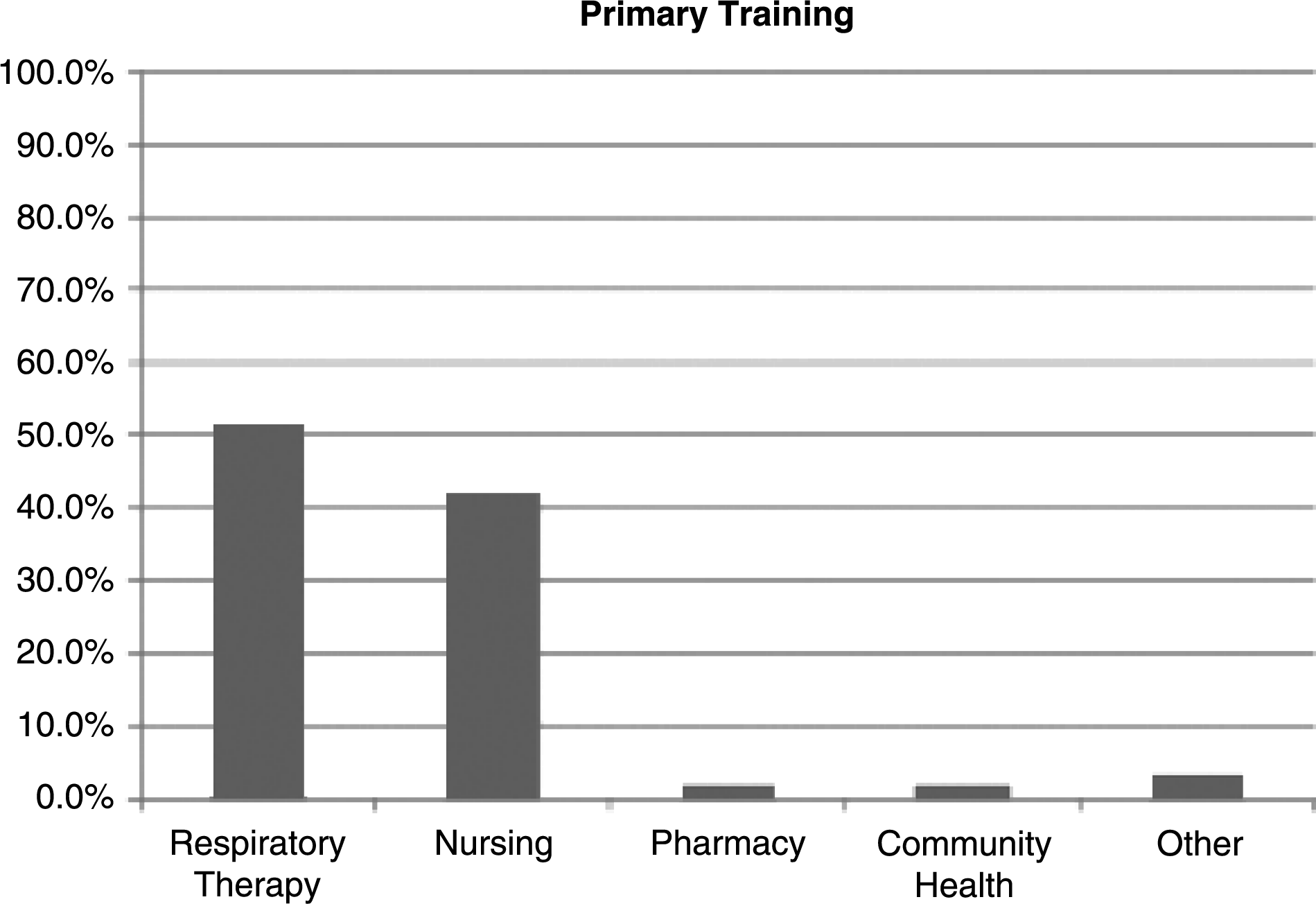
AE-Cs® primary area of training (n=65). AE-C®, certified asthma educator.
The respondents were predominantly female (92.3%). Race and ethnicity were found to be as follows: Caucasian 95.4%, Hispanic 3.1%, and African American 1.5%. There were no respondents in the Asian or other categories. See Table 1 for racial and ethnic breakdown of AE-Cs® and comparison against population of individuals with asthma in the United States. 12
AE-C®, certified asthma educator.
Over 90% of recertificants reported at least 5 years of work-related experience at the time of recertification, with the largest group (39.1%) reporting over 20 years of experience, followed by 14.1% with 15–20 years, 20.3% with 10–15 years, 17.2% with 5–10 years, and 9.4% with <5 years.
A personal diagnosis of asthma was acknowledged in 40.3% of respondents and 51.6% reported an immediate family member with asthma.
Most AE-Cs® (81.5%) live in either suburban or rural communities, whereas only 18.5% live in urban areas. Conversely, almost 60% work in urban communities in either subspecialty or hospital practices. Seventy-eight percent were employed full time. The distribution of primary work-related settings is listed in Table 2. Respondents were asked to identify their work responsibilities. These are listed in order of frequency in Table 3.
Twenty percent of the respondents stated that their job responsibilities increased as a result of achieving their original certification as an AE-C®. These added responsibilities included independent patient educational contacts and promotions to positions including coordinator of asthma education and programming, asthma program administrator, training coordinator for community health workers involved in asthma education, primary asthma educator in a children's hospital, staff educator for either or both nursing and medical staff. In addition to promotions, the responders focused on the importance of establishing credibility and demonstrating expertise in asthma education for themselves, their employers and coworkers, improved marketability, and additional managed care contracts. Only 6.3% reported an additional increase when change following recertification was addressed.
Salaries increased in 9.4% as a result of initial certification and in 1.6% as a result of recertification. However, the ability to bill for asthma education services increased from 7.8% reported after initial certification to 12.3% following the recredentialing process.
Table 4 shows the number of AE-Cs® in the 10 most and 10 least populated states. 12 Ratios have been calculated based of the number of AE-Cs® divided by the number of individuals with asthma in each state, estimated by national prevalence rate.
AE-C®/asthma population (AP) ratio was calculated by assuming a uniform asthma rate per state of 8.2%, which is the overall asthma prevalence for 2009.
Numbers in parentheses indicate state population (U.S. census 2008 12 ).
Discussion
Need, access, and availability
At this time, the AE-Cs® per asthma population ratios are poor and extremely variable, with AE-Cs® themselves reporting that the AE-C® jobs predominate in specialty and hospital-based settings.
Similar to our data, Wasilewski et al. 13 in a 2006 report of early adopters found that AE-Cs® predominated in urban settings. However, there has been a trend from inpatient hospital-based toward specialty outpatient settings as venues for educators to provide services. The supply and availability of AE-Cs® are increasing, with a current workforce exceeding 3,000 educators, certified nationally.
However, 22% of the AE-C® workforce responding to this survey was working part-time. Based on the number of individuals with asthma in the United States, there is no expectation for adequate numbers of AE-Cs® to be available in the near future to serve every patient with asthma. Initiatives to increase both numbers of AE-Cs® and access are underway to address this problem.
The AE-C® pipeline
AE-Cs® come from 2 major healthcare professions: nursing and respiratory therapy. Pharmacists, physicians, and community health workers remain poorly represented. 13 Many AE-Cs® concentrated on asthma education after years in the workforce. The AE-C® does not appear to be a primary certification. More than 30% of all AE-Cs® had a masters or higher level of education. The majority of AE-Cs® worked full time in hospital-based and subspecialty outpatient programs, which were located primarily in urban areas. Therefore, the workplace, particularly hospitals and subspecialty offices, would appear to be the most promising sites to recruit candidates for the AE-C®. The NAECB encourages young healthcare professionals interested in asthma to seek the AE-C® credential as an opportunity to improve asthma care for their patients and their communities. Significant numbers of AE-Cs® had personal links to asthma through either direct personal experiences or family involvement. This link may also provide recruitment opportunities through local asthma coalitions, school, and community program.
Workforce disparities
Asthma prevalence has been shown to be highest in the African American and certain subsets of the Hispanic-American populations in the United States. 4 It affects individuals in lower socioeconomic groups at disparately higher rates and has been found in greatest concentrations in north-eastern and mid-western regions of our country.5,6 At this time, the AE-C® workforce does not reflect the demographics of the population it serves, as 74% of those affected are Caucasian, 12% Black, 10% Hispanic, 3% Asian/Pacific Islander, and 1% American Indian or Alaskan native based on U.S. census data where adults reported if they had ever been told or currently had asthma. 1 Race and gender are not included in the examination application. The information on the workforce demographics has been generated based on survey responses. The benefits of culturally sensitive care and a diverse workforce have been extensively discussed in the healthcare literature.14–18 In addition, the AE-C® workforce is not geographically well distributed nor is it concentrated in geographic areas with the greatest asthma burden. The average number of AE-C® per state is 56, with a range between 4 and 259. There was no correlation with AE-C® numbers and prevalence of asthma either by state population or in relation to states with highest asthma prevalence.
Benefits to the AE-C® credential
The impact of the initial AE-C® certification resulted in additional job responsibilities for 20% of our respondents. These added responsibilities included independent patient educational contacts and promotions to positions including coordinator of asthma education and programming, asthma program administrator, training coordinator for community health workers involved in asthma education, primary asthma educator in a children's hospital, and staff educators for both nursing and medical staff. In addition to promotions, the responders focused on the importance of establishing credibility and demonstrating expertise in asthma education for themselves, their employers and coworkers, improved marketability, and additional managed care contracts. Many of these factors also appear in studies describing important factors determining job satisfaction and performance. Job satisfaction has been recently linked to improved performance outcomes. 19 The additional responsibilities accounted for an increase in base salary in 9.4% of those who responded to the original survey. Recertificants were also asked about the personal impact of their AE-C® certification in the 2010 study, which occurred during a time of national economic crisis. Although only 1.6% responded that they had an increase in their salary as a result of the recertification process, 12.3% of these same respondents now indicated that they were able to bill for their services when compared with 7.8% who were able to bill following initial certification.
Because there are differences in the reimbursement programs between states, among different levels of providers, and within different healthcare systems, we did not ask about level of reimbursement but only the ability to bill, which we hoped to use as a marker of acceptance and awareness of the value of educational services. The majority of survey responders did not experience a change in job responsibilities following recertification, whereas the remainder added administrative and managerial responsibilities to their existing work load.
Impact of AE-C® shortage on reimbursement
An increasing number of asthma-related organizations, including the Environmental Protection Agency 20 and regional asthma coalitions, have become staunch advocates for mandated coverage for asthma education. In fact, the Asthma Regional Council of New England has recom mended that policymakers “create a sustainable statewide reimbursement mechanism that supports best practices for asthma care, including asthma education and environmental interventions.” 21 It is our goal to engage more health plans in supporting reimbursable programs for asthma education by increasing the number, availability, and distribution of AE-Cs® to serve individuals with asthma.
Limitations of this study
Although the response rate for this study is respectable, the authors recognize the bias intrinsic to surveys and the limited number of respondents in the recertificant pool. Additionally, this is a purely descriptive study and highlights the need for outcomes-based research to confirm the cost effectiveness of AE-Cs®.
Conclusions
Most AE-Cs® have their basic training in either respiratory therapy or nursing. The workforce of AE-Cs® does not reflect the racial or ethnic percentages seen in the asthma population in the United States. More educators are needed to serve the growing numbers of individuals with asthma with the goal to improve communication and patient involvement in therapeutic partnerships with their providers.
Footnotes
Author Disclosure Statement
All authors are current or immediate past members of the Board of Directors of the NAECB.