
Abstract
We report a case of acute respiratory distress syndrome associated with eosinophilic pneumonia in an adolescent with acute Epstein-Barr viral infection.
Introduction
EBV, a member of the gamma herpesvirus family, has been associated with viral bronchiolitis and bronchitis. 2 Positive EBV serology may be present in asymptomatic carriers 3 ; however, several studies have linked EBV serology, EBV detection through immortalization assays and acute CD8+ lymphocyte predominance to an active pulmonary process in bronchoalveolar lavage (BAL) samples.4–6 EBV has also been shown to affect the lymphoid cell lines (B cells>T cells), thereby causing follicular bronchiolitis in otherwise healthy individuals as well as a lymphoproliferative disorder in the immunocompromised, post-transplant population (post-transplant lymphoproliferative disorder).7,8 Individuals with X-linked lymphoproliferative disease, a form of immunodeficiency, have mutations in their signaling lymphocytic activation molecules in both T and natural killer cells, which can result in fatal lymphoproliferation when infected with EBV. 9 Recently, EBV has been linked to fatal lymphoid proliferations in nonimmunocompromised, nontransplant children. 7
Viral infections are known to stimulate eosinophil chemoattractants that include eotaxin (CCL11) and RANTES (CCL5) as a part of the body's host defense against infection.10–12 Studies using transgenic animals have shown that the presence of eosinophils helps clear respiratory syncytial virus (RSV) infection from the lungs faster than in control animals.13,14 Recent work has also shown that Pneumovirus will replicate in eosinophils during a viral infection which increases cytokine production and likely plays an important role in viral clearance. 12
Case
A 16-year-old Caucasian woman presented to a local emergency department with a fever, cough, and sore throat. Her past medical history was unremarkable for atopic disorders, asthma, or recurrent pneumonia. Despite a normal chest radiograph, she was prescribed a 5 day course of azithromycin to treat a presumed case of community acquired pneumonia. Two weeks later, she returned to the emergency department with fever, sore throat, malaise, and mild increased work of breathing. The repeat chest radiograph showed an interstitial pneumonia, and a monospot test was positive. She was treated with albuterol and sent home with an additional course of azithromycin. Within 24 h she developed cough, progressive dyspnea, and tachypnea. She had received one dose of azithromycin. On the third return to the emergency department, she was hypoxemic with an oxygen saturation of 84% in room air. She was tachypnic with a respiratory rate of 44 breaths per minute and had moderate retractions and nasal flaring on clinical exam. The chest radiograph showed worsening interstitial pneumonia with bilateral pleural effusions and bilateral lower lobe infiltrates (Fig. 1). In the emergency department, she was given 3 albuterol treatments, dexamethasone, and placed on supplemental oxygen for subsequent transport to our pediatric intensive care unit. On arrival to the intensive care unit, her respiratory rate was 32 breaths per minute, and her oxygen saturation was 95% on 2 liters per minute of supplemental oxygen delivered by nasal cannula. Admission labs showed a white blood cell count of 5,200 cells/mcL, hemoglobin of 12.6 g/dL, hematocrit of 37.2%, and platelet count of 193,000 cells/mcL. The differential showed 77.1% neutrophils, 16.1% typical lymphocytes, 1.4% monocytes, 0.4% basophils, and 5% (<300/cu mm) eosinophils. The complete metabolic panel was unremarkable with the exception of a bicarbonate level of 19 meq/L and a total protein of 5.9 g/dL. Liver enzymes were normal. A chest computed tomography showed enlarged mediastinal and hilar lymphnodes, multifocal areas of airspace disease more consolidated in the lower lobes, patchy areas of rounded nodular airspace disease, and bilateral small pleural effusions (Fig. 1). Due to her clinical course, the infectious disease service was consulted for further evaluation of a possible atypical bacterial or fungal process in the lungs. Multiple bacterial and fungal blood and sputum cultures were sent and were ultimately negative. The EBV viral capsid antigen IgM was 3.91, and the IgG was 3.06 (both positive). The EBV nuclear antigen IgG was 0.21 (all 3 EBV assays had the same reporting range: <0.90 not detected, 0.90–1.09 equivocal, and 1.10 or greater detected). Serum titers for Mycoplasma, Histoplasma, and Bartonella were negative. HIV antibody tests were negative. Intravenous ceftriaxone, azithromycin, and amphotericin B were given after the cultures had been obtained.
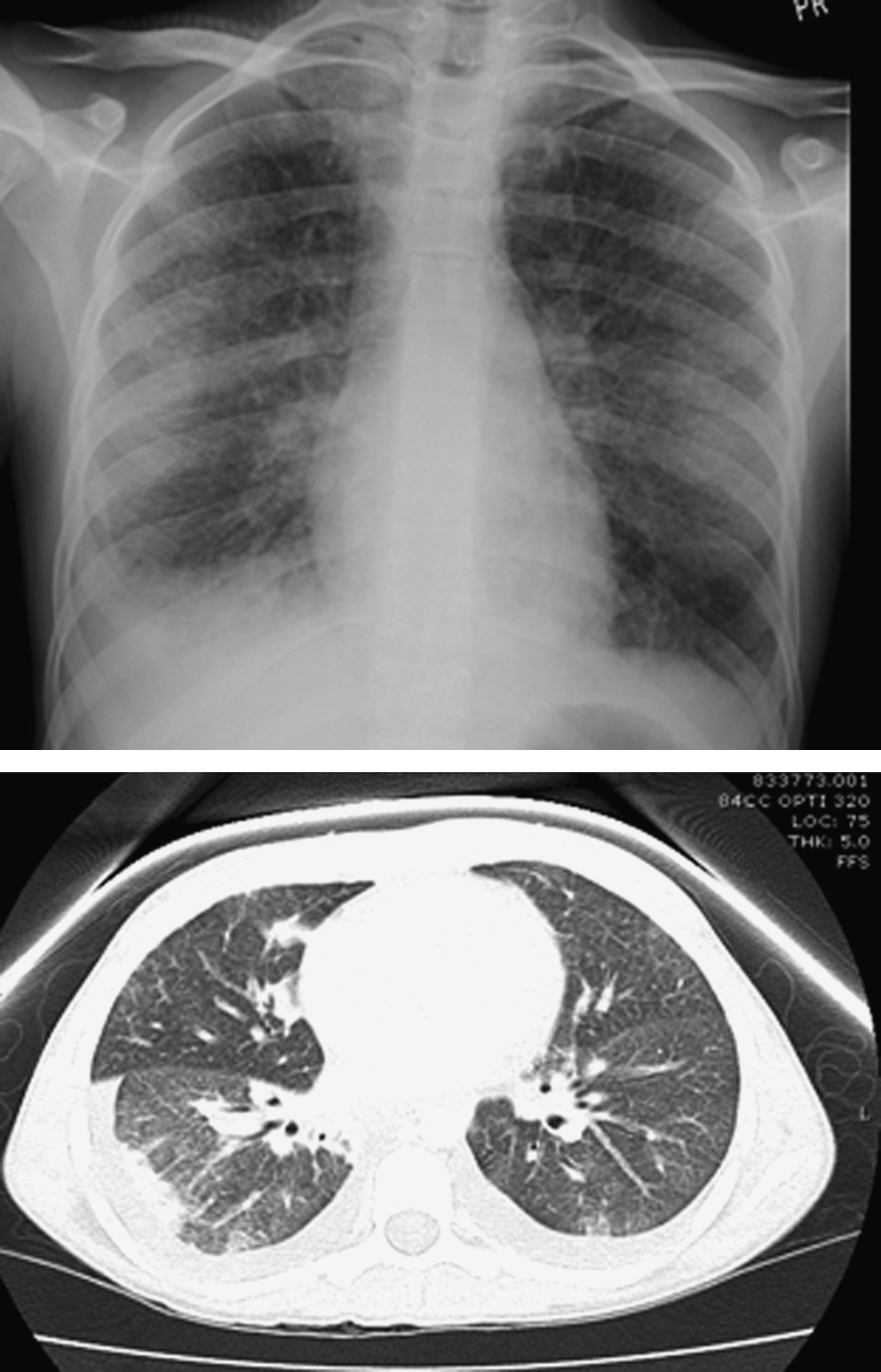
Chest radiograph showing interstitial pneumonia with bilateral pleural effusions and lower lobe infiltrates. Computed tomography scan showing multifocal areas of airspace disease with more consolidation in the lower lobes and patchy areas of rounded nodular airspace disease. Enlarged hilar/mediastinal lymphnodes are not visualized in this cut.
Within 24 h of admission, she progressed to respiratory failure and was started on bi-level positive airway pressure. Her subsequent arterial blood gas showed a pH of 7.25, paCO2 of 63 mmHg, and a paO2 of 91 mmHg. Endotracheal intubation and conventional positive pressure ventilation was initiated. Her PaO2/FiO2 gradient met criteria for ARDS (PaO2 was 114 at the time of intubation and 97 after 1 h of intubation, whereas FiO2 was 100%). A flexible fiberoptic bronchoscopy with BAL from both the right and left lungs was obtained. Her respiratory failure eventually required oscillatory support (MAP 25, Hz 5, and deltaP 75). The BAL cultures for bacteria, fungus, and mycoplasma were negative. The BAL flow cytometry showed lymphocyte predominance with a low CD4/CD8 ratio of 0.5 due to an elevated CD8 count. The cell count from the right sided BAL showed 28% eosinophils, 1% neutrophils, 33% lymphocytes, and 38% monocytes. The left-sided BAL showed 58% eosinophils, 25% monocytes, 15% lymphocytes, and 4% neutrophils (Fig. 2). Both the right and left BAL samples were EBV positive on the polymerase chain reaction (PCR) assay, but no EBV copy counts were available from the assay used. She was given intravenous pulses of high-dose methylprednisolone at a dose of 4 mg/kg/day for 5 days. She was extubated ∼24 h after initiation of methylprednisolone therapy. Two weeks later, her spirometry, lung volumes, and carbon monoxide diffusing capacity of the lung (DLCO) showed a mild restrictive defect; and her chest radiograph showed improvement in the interstitial lung disease. Five weeks after her initial respiratory failure, her chest radiograph, spirometry, lung volumes, and DLCO were normal (Fig. 2).

Table comparing pulmonary function tests that were done at 1 and 5 weeks after glucocorticosteroid therapy had been initiated. High power micrograph of the bronchoalveolar lavage fluid showing increased numbers of eosinophils.
Discussion
EBV has been implicated in multiple clinical manifestations but never in a case with EP or ARDS. In this case, we present a patient with an active EBV infection by clinical history and subsequent development of EP and ARDS. She had a positive monospot test identified 2 weeks before the onset of her respiratory symptoms and was again positive at the time of admission to the pediatric intensive care unit with a positive monospot test, EBV blood serology suggestive of an acute infection, and BAL studies indicative of an active infection (EBV PCR and elevated CD8 count).
One possible trigger for the development of EP is the azithromycin she received for presumed community acquired pneumonia. A recent review of EP reports that most patients have been treated with antibiotics for community-acquired pneumonia before a diagnosis of EP is made. 15 Clarithromycin, another macrolide, has been associated with pulmonary infiltration with eosinophilia. 16 However, the EP which developed in that patient was associated with a rash and occurred within several hours of an initial dose of clarithromycin, resolved with discontinuation of the drug, and rapidly recurred within hours of re-initiating the drug a few days later. Our patient was evaluated by the allergy/immunology department, and the possibility of a drug reaction was deemed low based on physical exam, lack of rash, and clinical history of medication dosing and timing of symptoms. Our patient had received azithromycin on 2 occasions before the development of EP and ARDS and continued to be treated with IV azithromycin in the intensive care unit past the time of the patient's clinical improvement, extubation, and improvement on chest radiograph. This clinical picture does not fit the temporal relationship of previous reported macrolide-induced drug reactions. 16
A second possible trigger for EP and ARDS is the acute EBV infection. EBV has been linked to lymphoproliferation, but not previously with EP. EBV has been linked to lymphoproliferation in both B and T cell populations (B cells>T cells),7–9 with nasal type extranodal natural-killer/T-cell lymphomas 17 and has also been linked to the pathogenesis of Hodgkin lymphoma with EBV-infected lymphocytes with EBV genes with plausible oncogenic function. 18 Also, nodular sclerosing classical Hodgkin lymphoma has increased numbers of reactive lymphocytes, eosinophils, and plasma cells on histology. Although EBV has never been clinically linked to EP, recent work has shown that dendritic cells and lymphocytes play a key role in inflammatory cell recruitment in lung inflammation, including eosinophilia. One of the chemokines in this pathway is EBV-induced lymphoid chemokine/CCL19. 6 This could be a possible link between the EBV infection and subsequent development of EP/ARDS.
A third and more intriguing possibility is the combination of a viral-drug reaction between EBV and azithromycin leading to the development of EP with ARDS. Viral-drug reactions have been identified in several different conditions including ampicillin rash during infectious mononucleosis caused by EBV. 19 Also of interest, the herpesvirus family (EBV, human herpesvirus 6, human herpesvirus 7, and cytomegalovirus) have been shown to be involved in the development of severe systemic hypersensitivity reactions [drug rash with eosinophilia and systemic symptoms/drug-induced hypersensitivity syndrome (DRESS/DIHS)] when exposed to certain classes of medications such as anti-convulsants.20,21 Our patient did not meet the strict criteria for the DIHS/DRESS syndrome, which includes a maculopapular rash, lymphadenopathy, fever over 38 degrees centigrade, leukocytosis with atypical lymphocytosis or eosinophilia, hepatitis, and HHV-6 reactivation. However, she did have fever, lymphadenopathy, leukocytosis with eosinophilia, and a low total protein count. Dramatic decreases in serum IgG, IgA, or IgM levels can be seen in these conditions. Although our patient did not have her immunoglobulin levels checked, she was noted to have a low total protein at the time of the infection. 22
Regardless of the trigger, this case is important, because it illustrates the importance of bronchoscopy and BAL for the diagnosis of EP. Our patient did not have elevated eosinophil counts in her peripheral blood, and the diagnosis of EP was made by demonstrating significant esosinophilia in the BAL specimen.
Footnotes
Author Disclosure Statement
None of the listed authors have any financial interest or involvement with organizations that are related to the subject manner in this article.