
Abstract
In this article, authors describe the work of Regional Asthma Management and Prevention (RAMP) in developing a comprehensive model for reducing the burden of asthma through the integration of clinical management and environmental protection. Over the past 15 years, RAMP grew a small legal settlement involving air pollution into a nationally recognized asthma program. RAMP collaborates, coordinates, shares resources, advocates, and promotes policy change to reduce inequities, strengthen asthma prevention efforts, and improve management for all communities. RAMP's 4 functions—provide technical assistance, serve as a clearinghouse, serve as a convener, and lead policy advocacy efforts—have provided an important structure for implementing a broad and comprehensive program aimed at reducing the burden of asthma. RAMP has demonstrated that asthma interventions must take place in numerous settings including clinical settings, homes, schools, child care, and outdoor environments and that, to reduce asthma disparities, organizations need to understand and address the environmental and social inequities that contribute to those disparities. RAMP has also seen firsthand the importance of community asthma coalitions in addressing the problem of asthma and the way that these coalitions benefit from the support of an organization like RAMP. RAMP has created a framework for reducing the burden of asthma that ties together the knowledge gained over 15 years and provides a model for other organizations.
Introduction
Theoretical Basis of RAMP
RAMP leads, promotes, and supports interventions in multiple settings—homes, schools, child care settings, clinical settings, and outdoor environments—and across multiple levels of the socioecological model (SEM). The SEM is a framework widely used in the field of public health. It conveys the importance of a comprehensive approach to prevention that encompasses multiple levels of intervention, beginning with individual level change and culminating with societal change. The SEM is used to address and recognize the multifaceted cause and effect of health disparities. RAMP has utilized this framework in guiding its work and developing an asthma-specific framework, shared later in this article.
History
In the San Francisco Bay Area in the mid 1990s, there was a growing interest in the issue of asthma among diverse constituents, ranging from public health departments to managed care organizations to community-based organizations. In 1995, asthma was estimated to affect 2.2 million Californians and it led to approximately 40,000 hospital stays. 1 PHI saw an opportunity to address this growing interest by creating a collaborative response. Using funds from a small legal settlement related to air pollution, PHI created RAMP, a project that would bring together diverse sectors—healthcare organizations, physician groups, public health departments, managed care organizations, and others—to collectively determine and guide activities to address the problem of asthma.
One problem that this new project immediately tackled was the lack of data on asthma prevalence. In response to this research gap, RAMP created and publicized a report mapping zip-code level information on asthma hospitalization rates across 4 counties in the Bay Area. Asthma prevalence is difficult to ascertain and is generally done only through self-report surveys. Therefore, data on hospitalizations or emergency department visits are often used as a proxy to understand the burden of the disease. The picture that emerged showed significant disparities in asthma hospitalizations, with low-income communities and communities of color bearing a disproportionate burden. After local health plans and local health departments were presented the data at a meeting convened by RAMP, many were compelled to start asthma programs. For example, the Contra Costa County Health Department applied for and received a 3-year grant to provide education and clinical services in the western part of the county, which has the highest rates of asthma. Additionally, in the city of Berkeley, the report prompted residents to go directly to the city council and demand to know why they had high asthma hospitalization rates; the city then allocated $50,000 for a study to try to answer that question.
RAMP also leveraged this report to gain support for its own work. The California Endowment, the largest foundation in the state, recognized the importance of a public health response to the problem of asthma and provided RAMP with a grant to stimulate activity across the region. This funding helped RAMP develop 3 of what are now considered to be its core functions: (1) providing technical assistance, (2) serving as a convener, and (3) serving as a clearinghouse. Under this grant, RAMP helped with the formation of community-based asthma coalitions in 3 communities with disproportionately high rates of asthma hospitalizations. RAMP provided technical assistance to these coalitions in the areas of coalition development, community needs assessment, program planning, advocacy, and sustainability. All of these coalitions received funds to support their coordination as well as to hire Community Health Outreach Workers (CHOWs), who conduct in-home visits with families affected by asthma. During their visits, the CHOWs work with families to support self-management of asthma and to help them identify and reduce exposure to environmental asthma triggers. This provided an opportunity for RAMP to develop its second function—serving as a convener. RAMP began hosting meetings for the CHOWs across the region to provide education, capacity building, and networking opportunities—these meetings continue to this day, demonstrating the significant demand for them. The third function that emerged was for RAMP to serve as a clearinghouse of asthma information. This was done through gathering and sharing tools, articles, and resources on RAMP's website, as well as through creating tools to support asthma programs. For example, RAMP created wall charts to assist physicians in following the asthma guidelines created by the National Heart Lung and Blood Institute. RAMP also convened a regional group to create Asthma Action Plans, which have since been updated, translated into 4 languages, and broadly disseminated across the nation.
Evolution
RAMP continues the 3 aforementioned functions today, but has also expanded its work into new areas. In terms of its original functions, RAMP still provides technical assistance to asthma coalitions across California and has compiled a set of resources in the areas that technical assistance is most often requested, now available on the Web site. RAMP also continues to serve as a convener. RAMP hosts an annual round table dialog among school nurses to discuss strategies for addressing asthma in schools. RAMP has also brought people together for discussions on topics such as land use policies, transit-oriented development, and culturally competent communication between providers and patients, to name a few. RAMP also continues its role as a clearinghouse. RAMP recently developed a section of the clearinghouse focused on inequities and shares an array of asthma updates with over 800 recipients through an electronic newsletter.
A significant expansion occurred in 2005 when RAMP assumed responsibility for the coordination of Community Action to Fight Asthma (CAFA), a statewide network of community asthma coalitions who collectively aim to reduce environmental triggers of asthma through policy change. This encouraged RAMP to solidify its fourth major function—leading advocacy efforts. RAMP and the local asthma coalitions it supports have since engaged in numerous policy efforts at the local, regional, and state levels. Asthma coalitions have successfully advocated for numerous local policy changes including the following:
• Creating and enforcing policies to prevent and address indoor air quality problems in schools; • Establishing protocols for reducing the presence of environmental triggers in schools by restricting the use of unhealthy cleaning supplies; • Promoting the use of integrated pest management to reduce children's exposure to potentially harmful pesticides in schools; • Improving housing inspection and remediation practices to reduce exposure to environmental triggers in rental housing; • Rerouting truck routes away from residential areas to protect communities from harmful diesel particulate matter.
RAMP, in coordinating the network of asthma coalitions, has helped to shape state-level policies, including the following:
• RAMP worked with a broad array of partners to advocate for 2 diesel regulations at the California Air Resources Board that addressed diesel pollution emitted by vehicles such as big rigs and construction equipment. It is estimated that these regulations will reduce diesel particulate matter by 43% by 2020. • RAMP and the CAFA Network successfully advocated to ensure that funds set aside for emergency school repairs could include repairs aimed at improving indoor air quality, thus not only highlighting the importance of the issue but also mobilizing resources. • RAMP and partners worked on the successful defeat of a California proposition that would have essentially overturned California's landmark greenhouse gas legislation.
Coalitions can serve as powerful advocates for policy change. They are able to mobilize large numbers of constituents to engage in advocacy efforts. Additionally, they bring together diverse organizations and perspectives that are able to reach and influence a broad array of decision-makers—more so than any one organization could likely do on its own. Along these lines, clinical champions play a unique role as coalition members in influencing decision-makers.
From the early stages of CAFA Network development, medical providers have played a key role as clinical champions. When conducting interventions in clinical settings, the role of clinical leadership is a key to success. However, clinician champions can have influence outside of the clinical setting as well. One coalition described a clinical champion as someone who believes in the importance of collaboration with the community and connecting with community organizations. Champions can be a conduit for communication with other physicians regarding community and social issues and can also be expert witnesses and advocate for policy change. Policy makers and the media are often interested in the testimony of medical authorities, and clinical champions can play a key role in getting the message of an asthma coalition heard. They carry a certain authority related to health and wellbeing that is hard to match.
Many clinicians became involved in coalitions during the last decade because of high levels of frustration at the inability to control for social and environmental factors when treating their patients. Clinicians would prescribe appropriate medications and educate their patients about self-management, but then send those patients back to environments where they continuously faced asthma triggers. To work with a dedicated coalition to support community and patient education as well as push policy makers to address asthma disparities and the root inequities that create them was an opportunity to address the issue more comprehensively. Examples of activities conducted by clinical champions within the California asthma coalitions include:
• Advocating for smoke-free policies at city council meetings; • Testifying at a hearing at the State Capitol about the risks of schools being built near freeways; • Testifying at the EPA about air pollution and asthma; and • Responding to media inquiries in relation to proposed bills.
Coalition members have described an important balance that includes mobilizing clinical champions to be engaged advocates while also mobilizing and elevating the voices of diverse members. These collective voices are what make coalitions so successful.
Current Programs
Throughout RAMP's existence, there has always been an awareness of and focus on asthma disparities. In recent years, RAMP has strengthened its focus on the social and environmental inequities that contribute to those disparities. In 2007, RAMP was awarded a grant from the U.S. Centers for Disease Control and Prevention to serve as a Center of Excellence in the Elimination of Disparities as part of its Racial and Ethnic Approaches to Community Health Across the U.S. Program. As a Center of Excellence, RAMP has been working to reduce asthma disparities through improving clinical management, improving management and reducing asthma triggers in schools and child care settings, and reducing asthma triggers in the environment.
In sum, RAMP has maintained many of its original activities and its core functions, but has also evolved and grown over time to create a stronger and more comprehensive model of asthma management and prevention. RAMP utilized its 15 years of experience and evolution to create a framework for reducing the burden of asthma—one that could be adapted and adopted by other asthma programs. Frameworks are important tools for both guiding the work of an organization and articulating the importance of that work. RAMP's Framework for Reducing the Burden of Asthma (Fig. 1) was adapted from the Bay Area Regional Health Inequities Initiative's Public Health Framework for Reducing Health Inequities. In this framework, RAMP demonstrates the relationships among the array of factors impacting asthma outcomes and the need for interventions at multiple target points.
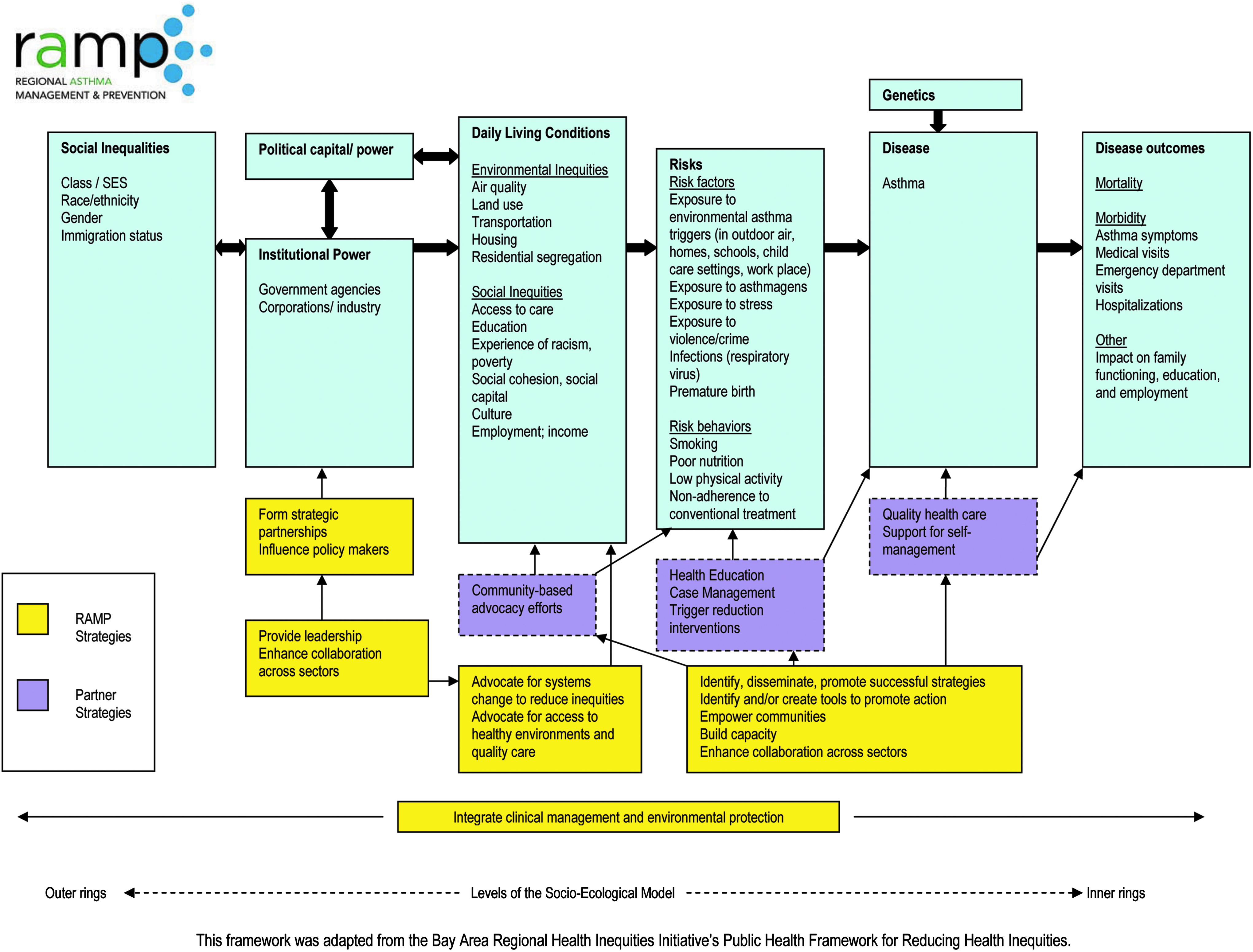
Regional Asthma Management and Prevention's Framework for Reducing the Burden of Asthma, demonstrating the causal pathway of multiple factors impacting asthma disparities and the strategies employed to mitigate those factors.
To illustrate how the framework may be used, one could look at the example of housing (Fig. 1). The far-right box of the framework has asthma outcomes, which include disparities based on race, ethnicity, and income level. To address the disease (the next box to the left), there is a need for access to quality healthcare and support for self-management. Moving further to the left, an effective asthma program also needs to address the risk factors, which include exposure to environmental asthma triggers—in the home, in this example. Health education and case management can help families reduce the triggers that are within their control, such as animal dander and environmental tobacco smoke. However, there are triggers inside housing that are beyond the control of tenants. So moving one box to the left is where there are environmental inequities—where low-income communities and communities of color are disproportionately exposed to substandard housing where landlords fail to remove mold, repair leaks, or address structural problems. It is also known that, for these same communities, housing is more likely to be near freeways, ports, or other polluting sources. So, the intervention targets become policies around housing codes and code enforcement, affordable housing, residential segregation, and land use. One could go even further to the left and focus on racism, lack of political power, and the other root causes of the inequities that lead to disparities in health.
This is just one example to illustrate how the thinking of an asthma program may evolve to span across multiple intervention points and to include a focus on inequities. A comprehensive approach to asthma includes not just addressing housing but also clinical management, schools and child care environments, outdoor air quality, transportation, and land use. The RAMP framework conveys the importance of leading or supporting interventions at multiple points across the framework's pathway and in multiple settings.
Lessons Learned
Over the past 15 years, RAMP has learned a great deal about creating a public health approach to asthma. Some of the important lessons include the following:
• An effective approach to asthma must be comprehensive, addressing both clinical management and environmental protection. • Asthma interventions must address asthma and environmental asthma triggers in numerous settings including clinical settings, homes, schools, child care, and outdoor environments. • To reduce asthma disparities, organizations need to understand and address the environmental and social inequities that contribute to those disparities. • An effective approach to asthma requires a broad array of diverse strategies including quality healthcare, health education, case management, trigger reduction interventions, community-based advocacy efforts, formation of strategic partnerships, and advocacy for systems change. • Community asthma coalitions can play a key role in addressing the problem of asthma and clinical champions can play an important role in those coalitions. • Community asthma coalitions benefit from the support of an organization like RAMP, which can provide them with technical assistance, serve as a clearinghouse, convene stakeholders, and lead collective policy action.
Footnotes
Acknowledgments
This work was performed at PHI. The source of financial support was The California Endowment.
Author Disclosure Statement
No competing financial interests exist.