
Abstract
Data on respiratory symptoms after smoking cessation are available for mature adults, but for young adults these data are limited to observational studies. This retrospective analysis of smoking cessation trials addresses the gap. A cohort of 18- to 24-year-olds without chronic respiratory illness was developed from 2 randomized trials of behavioral interventions versus standard care to promote smoking cessation. This secondary analysis was performed to determine whether short-term respiratory health improvements occurred among those who achieved smoking cessation for 2 weeks or more. Self-reported respiratory symptoms were assessed at baseline and last follow-up. The sample numbered 327, 60% smoked 5–10 cigarettes a day and 56% smoked for 1–5 years. Abstinence periods among those achieving cessation ranged from 2 to 78 weeks. The mean overall baseline respiratory symptom score was 14.3, standard deviation (SD)=11.5. Respiratory symptoms for those achieving cessation were mean=13.3, SD=11.2, decreasing to mean=3.8, SD=5.9 symptom days at the last follow-up. Baseline symptoms for those who continued smoking were mean=14.6, SD=11.6, decreasing to mean=10.3, SD=10.3 at follow-up. Five fewer respiratory symptom days per week were noted for those who stopped smoking (mean=5.2, SD=1.5, P<0.0001). Smoking cessation is associated with reduced respiratory symptoms. Feedback of short-term health consequences may be relevant to younger populations who may perceive smoking hazards as in the distant future.
Introduction
Methods and Materials
Data sources
This report is a secondary analysis of pooled data from 2 randomized controlled trials of behavioral interventions designed to motivate smoking cessation in young adults on college campuses.7–9 The aim for both of the original school campus–based studies was to determine whether the behavioral intervention increased smoking cessation. The interventions used computer-generated smoking cessation counseling with 3 in-person motivational interviewing sessions and health feedback. Participants randomized to the control groups received self-help smoking cessation manuals (see Fig. 1 for study flow).
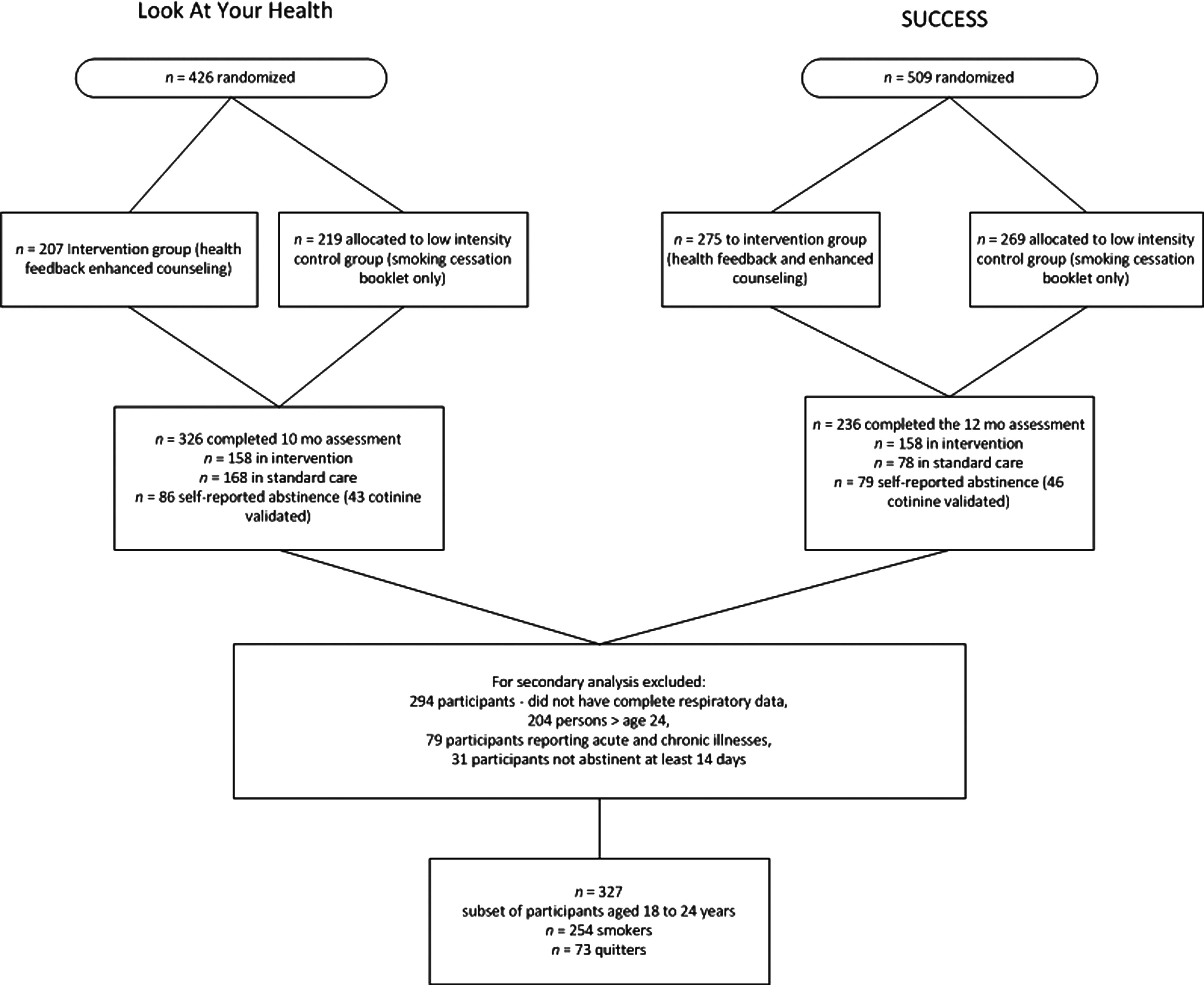
Study flow.
The first study, Project Look at Your Health, recruited 426 smokers attending 15 community colleges, with data collected February 1, 2000, to September 1, 2001. 8 The second study, Project SUCCESS, recruited 509 smokers attending college with data collected January 2, 2005, to December 7, 2007. 9 In both studies, eligibility criteria for inclusion were smoking at least 1 cigarette per day for the last 6 months, speaking and reading English, and being 18–35 years of age. Study candidates had to be interested in encouragement and instructions to stop smoking. The Institutional Review Board of the University of Texas MD Anderson Cancer Center approved the study protocols and participants provided informed consent.
Eligible participants were assessed for respiratory symptoms (self-reported), smoking history, and presence of preexisting asthma and bronchitis. Respiratory symptoms were assessed with a modified version of a respiratory symptom questionnaire (Table 1). 10 Items included the presence of morning cough, coughing during the day, coughing phlegm or mucus, wheezing, shortness of breath when walking and during exercise, pain in chest, and fatigue. Response categories and scores for the respiratory questionnaire are as follows: “never” was coded as 0, “less than once a week” was coded as 0.5, “1–2 times per week” was coded as 1.5, “several times a week” was coded as 3.5, and “every day” was coded as 7. Possible scores for each symptom could range from 0 to 7, thus were interpreted as the number of symptom days per week. Total respiratory symptom scores were calculated by summing the scores for the 8 symptoms for each individual. This analysis excluded those participants from the original studies who were over age 24 and reported chronic respiratory illnesses. This restricted the focus to otherwise healthy, college-aged smokers. Sustained smoking cessation was defined as continuous abstinence for 2 weeks or more prior to the last follow-up assessment available for the participant. Data from 31 participants were excluded from the analysis because smoking cessation was for less than 14 days. The rationale for excluding data for those who achieved less than 14 days of cessation was that it could reduce the degree of improvement seen in respiratory symptoms from cessation. Summary scores were generated for overall respiratory symptoms at baseline and the last available follow-up assessment. The minimum duration of follow-up was 3 months after baseline; the maximum was 12 months.
The response categories for the frequency of respiratory symptoms: every day, several times per week, 1–2 times per week, less than once a week, and never.
Statistical analysis
Demographic data were summarized and expressed as means±standard deviations (SDs) (Table 2). The mean change from baseline to follow-up in the overall respiratory symptoms between those who achieved smoking cessation and those who continued smoking was examined using a t-test. We employed 2-tailed P values at the 5% level to determine statistical significance for the primary outcome. In addition, the mean changes from baseline to last available follow-up in the individual respiratory symptoms between those who achieved smoking cessation and those who continued smoking were also examined using t-tests. In addition, we explored the differences in symptoms by gender and smoking status.
Results
Subjects were young adults (n=327, mean=21 years, SD=1.8), mostly women (54%), and Caucasian (74%). Sixty percent smoked 5–10 cigarettes a day and 56% smoked for 1–5 years (Table 2). Smoking status at the last available follow-up (10–12 months postbaseline) was available for 86% who completed the study (280 of 327). For the 47 participants who did not have smoking cessation status at the last follow-up documented, we accepted self-reported smoking status at 3 months postbaseline. Among the 73 attaining cessation, the mean duration of abstinence was greater than 3 months (median=13 weeks; range=2–78 weeks). We observed that respiratory symptom scores at baseline for participants who achieved cessation and for those who continued smoking are similar to the entire sample, mean=14.3, SD=11.5 (Table 3). Mean overall respiratory symptom scores at baseline for those who achieved cessation were mean=13.3, SD=11.2, and for those who continued smoking scores were mean=14.6, SD=11.6 (Table 3).
Overall respiratory symptoms calculated by summing 8 symptoms and obtaining the average.
Frequency of respiratory symptoms scored as every day=7, several times a week=3.5, 1–2 times per week=1.5, less than once a week=0.5, and never=0.
Comparisons (t-tests) between those who stopped smoking and those who continued to smoke at last available visit: †P≤0.05, *P≤0.008.
SB, shortness of breath.
Overall combined respiratory symptom scores decreased both in participants who continued smoking (mean=−4.3, SD=10.7 days reduction) and in those who stopped smoking (mean=−9.5, SD=11.8) (P<0.0001). Those who achieved cessation reported 5 additional days in reduction of respiratory symptoms per week, mean=5.2, SD=1.5; P<0.0001. Findings for the overall combined respiratory symptom score for those who achieved cessation were mean=−3.8, SD=5.9 versus mean=−10.3, SD=10.3 for those who remained smoking. Each individual respiratory symptom was reduced by approximately 1 symptom day for those who quit smoking with morning cough, daytime cough, and getting tired easily; however, all symptoms decreased. For those who continued smoking, a reduction of approximately 0.6 symptom days was noted (Table 3).
We stratified by gender to show differences and change in symptom occurrence (Table 4). For both men and women who achieved cessation, coughing (morning and daytime) showed the greatest reduction in symptom days at 1 day or greater. A slightly different pattern in symptom ranking was noted between men and women who achieved cessation. The symptom of chest pain was ranked third among symptoms that showed a reduction in days of symptoms for women, mean=1.3, SD=2.1, whereas chest pain ranked eighth among men (Table 4).
P≤0.05, *P≤0.008; SB, shortness of breath.
Discussion
We found substantial improvements in overall respiratory symptoms for young adults who achieved smoking cessation of 14 days or greater. Findings for this study also showed decreases in other less-reported respiratory symptoms—such as chest pain and getting tired easily. The decreases in the coughing items (morning and daytime) are similar to those observed in studies of older long-term smokers who stopped smoking.1–4
Given these results, appeals to promote smoking cessation among young adults who smoke must communicate both the long- and short-term benefits of smoking cessation. Younger persons who smoke may not be cognizant of a cause-and-effect relationship between smoking cigarettes and respiratory symptoms, minimizing their respiratory symptoms as normal. 11 Communication about the immediate benefits of smoking cessation on respiratory symptoms may enhance persuasive smoking cessation messages, increase receptivity to the message, and acceptance for young adults that, in turn, may increase motivation to quit. 11 For those who do quit, short-term improvements in personal respiratory symptoms may result in more positive cognitions and increase the likelihood of long-term cessation. A weakness in this secondary analysis is noteworthy. There could have been possible overreport of cessation by those who continued smoking, which could likely bias respiratory symptom results toward the null.
In conclusion, smoking cessation of 2 weeks or more demonstrated substantial decreases in respiratory symptom scores, with the greatest reductions on subscore items of coughing. Advising young smokers about the short-term reward of a reduction in respiratory symptoms may help in motivating actions to stop smoking.
Footnotes
Acknowledgments
Karen S. Calabro, DrPH, wrote this paper with generous support from Alexander V. Prokhorov, M.D., Ph.D. He mentors Dr. Calabro during her postdoctoral fellowship at MD Anderson Cancer Center. Dr. Prokhorov generously shared these data from 2 behaviorally-based interventions. We appreciated the superb statistical guidance from Beverly Shirkey, Ph.D. We are indebted to the excellent guidance about manuscript revisions from Dr. Harold Farber. The studies described herein were supported by 2 subsequent grants from the National Cancer Institute—CA69425-07 (“Look at Your Health”); Dr. Prokhorov, PI, and 1R01 CA69425-01A1 (Project SUCCESS); Dr. Prokhorov, PI.
Author Disclosure Statement
Karen S. Calabro did not have a personal or author involvement with organizations with financial interest in the subject matter or any conflicts of interests. Alexander V. Prokhorov did not have a personal or author involvement with organizations with financial interest in the subject matter or any conflicts of interests.