
Abstract
Thoracosopic surgery was first introduced in the early 1900s, but advances in the last 20 years have dramatically altered how pulmonary and extrapulmonary thoracic lesions in infants and children are now approached. Advances in equipment and technique now allow for most common thoracic surgeries to be approached through a series of small 3 and 5 mm incisions, using a telescope and digital camera to provide magnified images of the thoracic cavity. Large series of relatively simple procedures such as lung biopsy, and more complex operations such as lobectomy have clearly shown that these techniques are safe and effective, and associated with significantly less morbidity then the standard open thoracotomy.
Introduction
He later reported the first significant experience with a series of over 100 patients. 1 During the next 70 years thoracoscopy gained some favor, primarily in Europe, for the biopsy of pleural based tumors and limited thoracic explorations in adults; however, wide-spread acceptance was minimal.2,3
In the 1970s and 1980s the first significant experience in children was reported by Rodgers.4,5 Equipment modified for pediatric patients was used to perform biopsies, evaluate various intrathoracic lesions, and perform limited pleural debridement in cases of empyema. 6 However, even though there was an increasing recognition of the morbidity associated a standard thoracotomy, especially in small infants and children, there was little acceptance or adoption of these techniques. 7 It was not until the early 1990s with the dramatic revolution in technology associated with laparoscopic surgery in adults that more advanced diagnostic and therapeutic procedures have been performed in children. 8 The development of high-resolution microchip and now digital and high-definition cameras, smaller instrumentation, and better optics has enabled pediatric surgeons to perform even the most complicated intrathoracic procedure thoracoscopically. 9
Indications
Today there are a wide variety of indications for thoracoscopic procedures in children (Table 1) and the number continues to expand with advances and refinements in technology and technique. Currently, thoracoscopy is being used extensively for lung biopsy and wedge resection in cases of interstitial lung disease (ILD) and metastatic lesions.10,11 More extensive pulmonary resections, including segmentectomy and lobectomy, are now being routinely performed for infectious diseases, cavitary lesions, bullous disease, sequestrations, lobar emphysema, congenital adenomatoid malformations, and neoplasm.12–17 Thoracoscopy is also extremely useful in the evaluation and treatment of mediastinal masses. 18 It provides excellent access and observation for biopsy and resection of mediastinal structures such as lymph nodes, thymic and thyroid lesions, cystic hygromas, foregut duplications, ganglioneuromas, and neuroblastomas.19–21 Other advanced intrathoracic procedures such as decortication for empyema, patent ductus arteriosus closure, division of vascular rings, repair of hiatal hernia and congenital diaphragmatic defects, esophageal myotomy for achalasia, thoracic sympathectomy for hyperhydrosis, anterior spinal fusion for severe scoliosis and, and, most recently, primary repair of esophageal atresia have also been described in children.22–31
TEF, tracheo-esophageal fistula and esophageal atresia.
Preoperative Workup
The preoperative workup varies significantly depending on the procedure to be performed. Most intrathoracic lesions require routine radiographs as well as a computed tomography (CT) or magnetic resonance imaging (MRI) scan. A thin cut high-resolution CT scan is especially helpful in evaluating patients with ILD as it can identify the most affected areas and help determine the site of biopsy (Fig. 1) as the external appearance of the lung is usually not helpful. CT-guided needle localization can also be used to direct biopsies for focal lesions that may be deep in the parenchyma and therefore not visible on the surface of the lung during thoracoscopy. This is usually performed just before the thoracoscopy with the radiologist marking the pleura overlying the lesion with a small blood patch or dye. On occasion a wire may be placed as in breast biopsies, but these may become dislodged during collapse of the lung at the time of surgery. As intraoperative ultrasonography improves this may provide a more sensitive way for the surgeon to detect lesions deep to the surface of the lung and make-up for the lack of tactile sensation. Unfortunately, in its current state this technology is still unreliable. 32 An MRI scan may be more useful in evaluating vascular lesions or masses, which may arise from or encroach on the spinal canal or in the case of vascular rings. These studies can be extremely important in determining positioning of the patient and initial port placement.

High-resolution CT scan in a patient with interstitial lung disease. The CT is used to help determine the site of biopsy. CT, computed tomography.
Anesthetic Considerations
Another major consideration for the successful completion of most thoracoscopic procedures is whether or not the patient will tolerate single lung ventilation, thus allowing for collapse of the ipsilateral lung to ensure adequate observation and room for manipulation. Unfortunately, in most cases, there is no specific preoperative test that will yield this answer. However, most patients, even those who are ventilator dependent, can tolerate short periods of single lung ventilation. This should allow adequate time to perform the majority of diagnostic procedures, such as lung biopsy.
Single lung ventilation can be obtained using a number of different techniques, including double lumen endotracheal tubes, bronchial blockers, or in most cases a simple mainstem intubation of the contralateral side is sufficient. We have found that in most cases of congenital lung disease that the children tolerate nonventilation of the affected side without any adverse effect. This is primarily because we are no longer ventilating the diseased lobe, which often adds little to gas exchange in these patients. Usually, there is a slight increase in end tidal CO2, but this can be easily managed by slightly increasing the minute ventilation. These children tolerate the procedures so well that we rarely use direct arterial or central venous monitoring.
In patients with diffuse disease, such as ILD, or diffuse infections in immunocompromised patients, they may poorly tolerate being placed in a lateral decubitus position, let alone periods of single lung ventilation. If a child will not tolerate single lung ventilation, then creation of a mild CO2 tension pneumothorax, with pressures of 4 to 8, is usually enough to create space to work. In addition these patients are usually only undergoing lung biopsy and this procedure should only take a few minutes once the chest is entered.
Each patient must be evaluated and treated separately, and a good working relationship and communication between the surgeon and the anesthesiologist is imperative.
Empyema
Empyema is the most common intrathoracic problem encountered by pediatric surgeons and has traditionally been treated by antibiotics and varying degrees of chest drainage, including pleurocentesis, tube thoracostomy, minithoracotomy, and formal thoracotomy. More aggressive intervention has often been delayed because of the perceived morbidity associated with surgical intervention. This often led to days, weeks, or even months of antibiotics and pulmonary compromise, as these infections were allowed to resolve without adequate surgical drainage. Thoracoscopic debridement offers an opportunity to provide early intervention to diminish the morbidity and recovery period associated with an empyema while limiting the surgical trauma and recovery.33,34 It is rare that thoracoscopic decortication is not an appropriate first step. However, these patients are often septic with compromised pulmonary and cardiovascular status. The patient's condition should be optimized with fluid resuscitation, aggressive pulmonary care, and antibiotics. It is helpful in many cases to have a preoperative CT scan (Fig. 2). This will help in making the decision to proceed with thoracoscopy by determining the amount of loculated fluid, inflammatory peel, and to look for evidence of parenchymal injury.

CT scan of empyema.
In general, the procedure can be performed with just two 5 mm ports. These are placed in the anterior and posterior axillary lines at the fifth or sixth interspace. The primary goal of the operation is to remove as much as the infected fluid and fibrous peel as possible, breakdown any septa, allow for re-expansion of the lung, and provide adequate drainage. All of this can be performed under direct vision with an atraumatic forceps used to grasp the inflammatory peel and strip as much as possible off the lung surface and chest wall (Fig. 3). The more fibrous the peel removed the more effective this is. Once the majority of the peel is removed and all loculations are broken down the chest cavity is irrigated with copious amounts of saline with or without antibiotics. The time of the procedure should be kept to a minimum to avoid a prolonged anesthetic. This procedure should not take more then 60 min and in most cases significantly less.

Mechanical debridement of empyema peel using an atraumatic endoscopic clamp.
A single chest tube is placed thru the posterior port site so it lies in a dependant position. The limited surgical trauma allows aggressive postoperative physiotherapy. Having the patient spontaneously breathe and cough should aid in keeping the lung expanded and airway clear.
Some surgeons have advocated the use of urokinase, tissue plasminogen activator (TPA), or other agents to dissolve the inflammatory peel via a chest tube or in some cases intra or postoperatively.35,36 A recent randomized study by St. Peter et al. compared thoracoscopic debridement with insertion of a 12F chest drain and instilment of 3 courses of TPA spread 24 h apart. 37 They found that there was no significant difference in the days of hospitalization post-treatment days until afebrile, days of oxygen requirement, or analgesic requirements. The only significant difference was the charges associated with the thoracoscopy were higher. Both therapies appear to be effective and are reasonable alternatives. The decision may depend on the particular patient and the resources of the intitution.
In general, post-video assisted thoracic surgery (VATS) patients are followed up at 2 weeks postoperatively with a chest X-ray. If significant clearing is noted, further follow-up and radiographic studies are generally not necessary. Most of these patients return to full function with no pulmonary compromise.
Lung Lesions
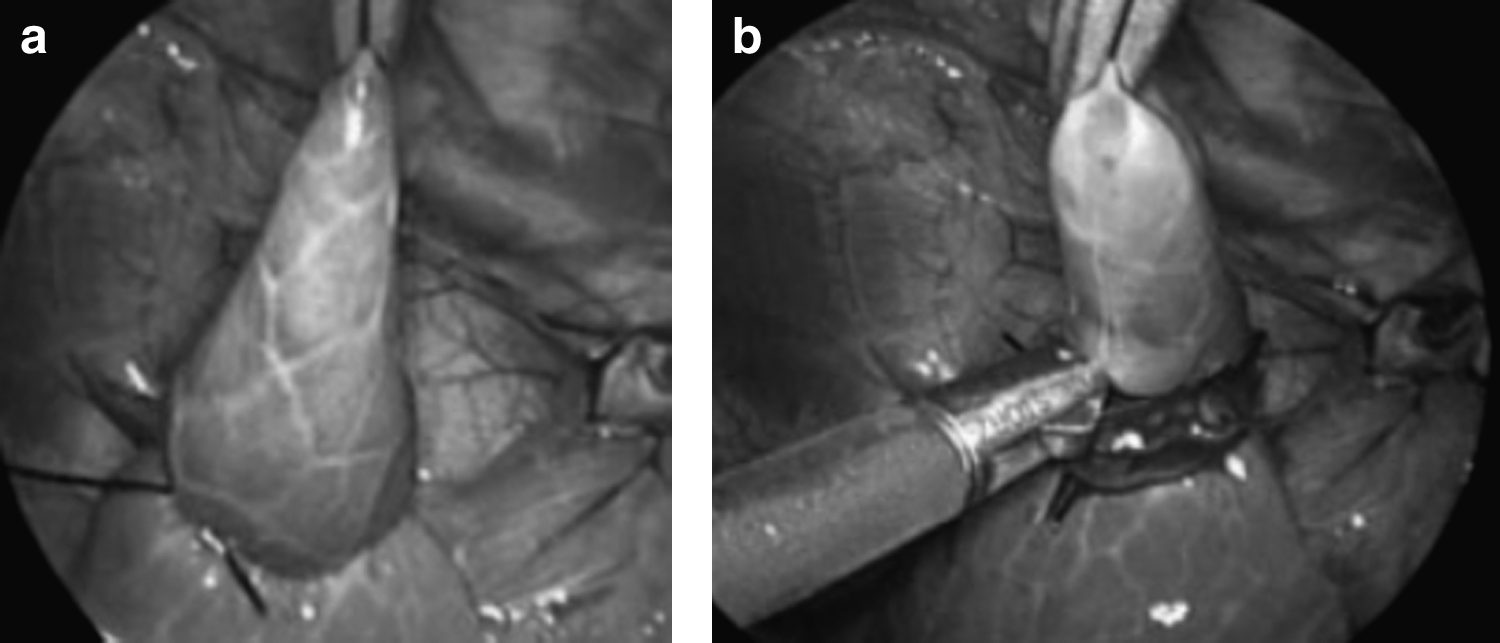
Lung biopsy is one of the most common thoracoscopic procedures performed and it should be the gold standard for obtaining lung tissue in children. The side for the biopsy is chosen based on CXR and CT scan findings. In general, 3 trocars, 3 to 5 mm, are sufficient to perform the biopsy. In cases where an endoscopic stapler is used a 12 mm port is necessary. In smaller patients (under 15 kg) whose chest cavity cannot accommodate the endoscopic stapler, endoloops (pretied suture ligatures) are used to snare and ligate sections of lung. Two consecutive loops are placed at the base of the specimen and the tissue is sharply excised distal to the ligatures (Fig. 4a, b). This provides a hemostatic and air-tight seal equivalent to that obtained with the stapler. 38 Specimens of 2 to 3 cm can be obtained in this manner and are more then adequate for diagnosis and biopsies can easily be obtained from all 5 lobes using this technique. Fan et al. as well as others have shown that thoracoscopic biopsy is superior to both transbronchial and open surgical biopsy in obtaining tissue to direct therapy and minimize surgical morbidity. 39
Metastatic lesions are also well approached thoracoscopically. Although the majority of nodules are peripheral, lesions less the 1 cm in diameter or deep in the parenchyma of the lung may not be readily visible on the pleural surface. In these cases preoperative CT-guided localization as previously described should be carried out. At the time of surgery with the lung collapsed the marked area can easily be identified. If the lesion itself is not visible then the area underlying the blood patch can be wedged out. A frozen section should be obtained to ensure the lesion is included with the specimen. Ongoing improvements in endoscopic ultrasound probes should eventually make this the technique of choice for localization.
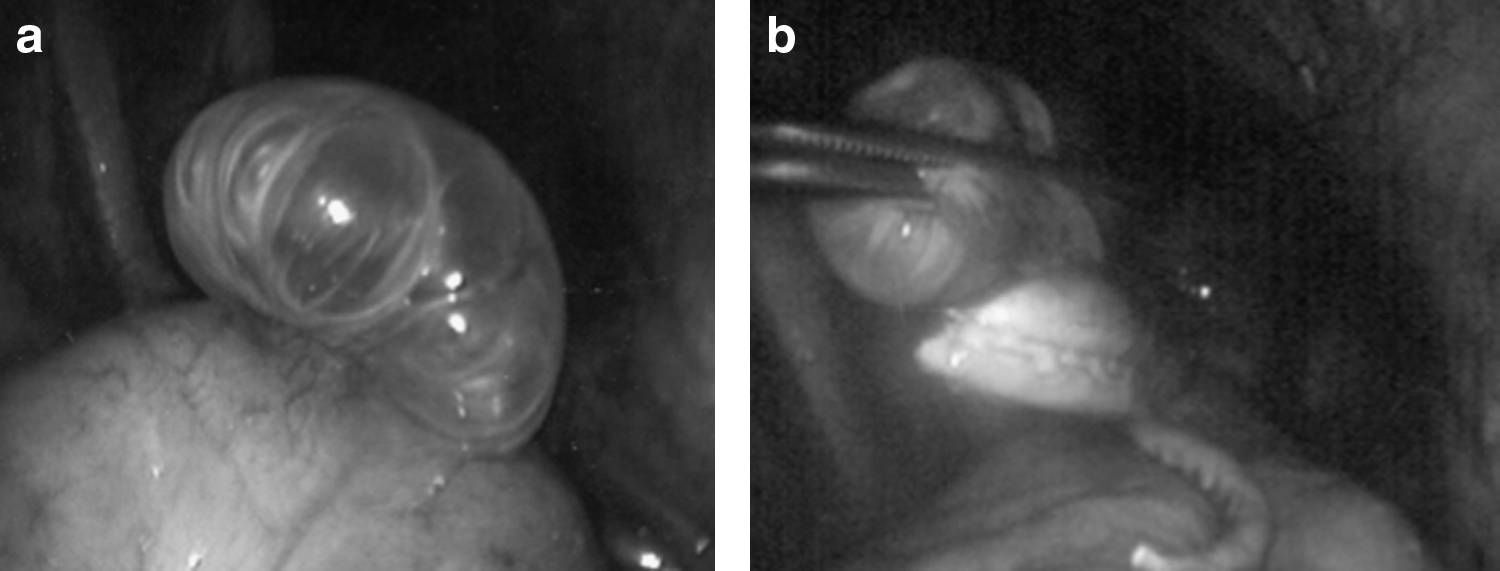
Resection of bullae or infectious cavitary lesions can also be accomplished using a similar technique (Fig. 5a, b). The minimal morbidity associated with thoracoscopy has shifted the algorithm for treatment and earlier surgical intervention is often indicated. 39 In the case of bullous disease presenting with a spontaneous pneumothorax it is usually advisable to combine this with a limited thoracoscopic pleurodesis or pleurectomy.
Once the intrathoracic procedure has been completed a small chest tube is placed through 1 of the trocar sites and the collapsed lung is ventilated. In most cases where there is no concern over adequate hemostasis or malignant effusion the chest tube can be removed before extubation in the operating room if no evidence of any air leak is present. This avoids the considerable discomfort associated with the chest tube in the postoperative period. Ponsky et al. showed that in a series of over 300 thoracoscopic procedures, 175 of which were lung biopsies, no chest tube were left postoperatively and there was no postoperative complications. 40 A chest X-ray is obtained in the recovery room and if the lung is fully expanded no further follow-up films should be necessary.
Thoracoscopic Lobectomy
Initial experience with minimally invasive lobectomy required a video-assisted or VATS approach. This combined the use of 2 to 3 trocars and standard laparoscopic instruments with a minithoracotomy through which standard thoracic instruments and staplers could be more easily passed. These operations were technically demanding and often arduous but did spare the patient the morbidity of a formal thoracotomy. The minithoracotomy was placed in the mid-axillary line and used a total muscle sparing technique. With the improvement in endoscopic staplers as well as energy sources, which can seal both pulmonary vessels and lung parenchyma, the need to employ a minithoracotomy has been eliminated. These procedures can now be done completely through small trocars without the need for any thoracotomy incision.
However, the surgeon's view is limited to a 2-dimensional plane, and it is difficult to do a lot of manipulation of the lobe in an attempt to look at both the anterior and posterior aspects gaining 3-dimensional perspective. Therefore, it is critical that the surgeon have a good understanding of the anatomic spatial relationships between the vessels, lung tissue, and bronchus as these structures may not be visible and cannot be palpated. Lower lobectomies are generally easier then upper as dissection can proceed along the major fissure and any vessel or bronchus crossing it are considered end vessels and can be ligated and divided. Upper lobectomies are much more difficult as dissection must proceed along the main pulmonary artery sacrificing each segmental branch to the upper lobe as it comes off, taking care not to injure the main trunk. Once the lobectomy is completed the lower trocar site is widened slightly and the lung is removed in a piecemeal fashion. Since these lesions do not generally require surgical margins, as the specimens are not malignant, the pathologist can make an appropriate examination even if the specimen is not whole. A chest tube is left in overnight but can usually be removed on the first pot-operative day if no air leak is present.
These advances in imaging and technique have also allowed for more limited, but anatomically correct, resections such as formal segmentectomy. This has been performed in cases of focal bronchiectasis, cystic lung disease, or other malformation. Hopefully, with continued improvements in equipment and imaging, these lung sparing procedures will become more widely accepted and performed.
Multiple series of thoracoscopic lobectomy have now been reported showing the procedure to be safe and efficacious. The majority have been for congenital pulmonary malformations, but many have been performed for infectious and malignant disease as well. The main advantage of this technique is not just in diminishing the pain and recovery associated with the operation, but in avoiding the long-term morbidity of scoliosis, shoulder girdle weakness, and chest wall deformity, that is clearly associated with a thoracotomy performed in an infant or child. In a series of lobectomies performed in infants less than 10 kg with a diagnosis of bronchopulmonary malformation the average operative time was less than 2 h, average chest tube time was 1.2 days, and the average length of stay was 2.4 days. These data support a plan for early surgery in these prenatally diagnosed lesions, operating before the malformations become infected and the surgery more technically difficult. A subset of this group, those patients less than 5 kg, had an average operative time of less than 90 min and average hospital stay of 1. 5 days. These data support intervention in the first few months of life. 41
Thoracoscopic lobectomy is probably the most technically demanding of the thoracoscopic procedures being performed today. It requires not only advanced endoscopic surgical skills, but an intimate knowledge of pulmonary anatomy. While advanced skills alone are adequate to perform procedures such as mediastinal masses, Empyema, and lung biopsy, one could argue that more complicated lung procedures, such as lobectomy, be performed at institutions seeing a large volume of these lesions. Our results show that these procedures can be performed safely, efficiently, and with lower morbidity then the open procedure. However, centers that perform only a few cases a year may not have the same results.
Conclusion
The advances in thoracoscopic surgery have now allowed even the most complex thoracic procedures, such as lobectomy and repair of tracheo-esophageal atresia (TEF), to be performed using minimally invasive techniques. The advantages to the infant and child are significant not only in reducing the short- and long-term morbidity of these procedures, but also by improving the observation and access for the surgeon.
A thoracoscopic approach should be the preferred technique today in dealing with pulmonary and thoracic pathology in infants and children.
Footnotes
Author Disclosure Statement
No competing financial interests exist.