
Abstract
Objective:
Respiratory Syncytial Virus (RSV) is the most common cause of bronchiolitis and viral lower respiratory tract infections in children. It is associated with annual winter epidemics across the United States, typically October through April. Our objective is to describe the clinical characteristics of children hospitalized outside the typical RSV season and to compare them with those admitted during the season.
Methods:
A retrospective chart review was conducted of all patients who were hospitalized at Children's Hospital of Austin from May 2000 to September 2006 and had a positive RSV antigen test. Descriptive statistics, tests of differences, and associations between patients diagnosed in the off-season versus typical season were conducted.
Results:
A total of 850 charts of RSV-positive cases were reviewed. Of these, 45 patients (5.3%) were admitted during the off-season. The following variables were statistically significantly associated with diagnosis in the off-season versus typical season: mean birth weight (2704 g vs. 3204 g respectively, p=0.0001); gestational age at birth less than 36 weeks (OR=4.35; 95% CI: 2.2, 8.6); history of neonatal intensive care unit (NICU) admission at birth (OR=6.04; 95% CI: 2.9, 12.5); and multiple birth (OR=3.38; 95% CI: 1.2, 9.2).
Conclusions:
Infants with RSV infection outside of the typical season were more likely to have been premature, of lower birth weight, the products of multiple births, and admitted to the NICU at birth.
Introduction
Our institution observed a portion of all RSV-related admissions to occur between May and September, usually considered to be the off-season. Our objective is to describe the clinical characteristics of children hospitalized during the typical RSV season and to compare them to those admitted in the off-season.
Methods and Materials
Patients
Charts for 850 patients hospitalized at Children's Hospital of Austin between May 2000 and September 2006 for laboratory-confirmed RSV infection were included in the study.
Study design
A retrospective chart review was performed on all RSV-related hospital admissions that occurred at Children's Hospital of Austin from May 2000 to September 2006. The study was approved by the Austin Multi-Institutional Review Board. RSV hospitalizations were identified using discharge diagnosis, in addition to laboratory records of a positive RSV test. Codes established by the International Classification of Diseases, Ninth Revision (ICD-9) were used for discharge diagnoses, which included RSV bronchiolitis (466.11), RSV pneumonia (480.1), and RSV unspecified (079.6). Only patients with confirmed RSV tests were included in the study.
RSV testing was done by either enzyme immunoassay (EIA) or by culture. Our laboratory utilized the Kallestad Pathfinder® EIA (Sanofi Diagnostics Pasteur Inc, Chaska, MN) and the Directigen™ EIA (Becton Dickinson Microbiology Systems, Cockeysville, MD) kits during the study period.
Data collection forms were utilized that included demographic information in addition to hospitalization data. Demographic information included gender, race, gestational age at birth, chronologic age, neonatal intensive care unit (NICU) admission at birth, birth weight, multiple versus singleton birth, and status of RSV prophylaxis (Palivizumab). Information regarding RSV hospitalization included admission date, discharge date, admission less than 24 hours, RSV test performed, test type, test result, date of test, discharge diagnoses, outcome of death, greatest absolute lymphocyte count, oxygen requirement, ICU admission for a respiratory condition, and duration of ICU stay.
Study end points
This study aimed to describe the population of children in Central Texas hospitalized with RSV according to personal and hospitalization characteristics. Furthermore, this study was performed to compare characteristics of patients admitted during the typical season to those admitted in the off-season.
Statistical analysis
Patient and clinical characteristics were summarized and presented by season of diagnosis for 850 patients who met study inclusion criteria. Comparison of patient characteristics by season were performed using t-tests for equality of means, chi-square tests for categorical variables, Poisson regression to compare number of admissions by year, and logistic regression to examine the association of patient characteristics with season of diagnosis.
Results
Patient characteristics
Most patients admitted were aged less than 6 months (53% off-season versus 62% typical season). The majority (n=637) were term infants (i.e.,≥36 weeks gestation). Admissions occurred in each month of the off-season throughout the study period with the greatest number of cases (31% of off-season admissions) occurring in September, as shown in Figure 1. Although the number of admissions in the off-season varied from year to year from 3 to 10 admissions, cases occurred without statistically significant differences in incidence each year (Fig. 2). Additional characteristics of the patient population are described in Table 1.

Off-season distribution of RSV-confirmed hospitalizations at Children's Hospital of Austin, May 2000 to September 2006, total count by month of admission. RSV, respiratory syncytial virus.
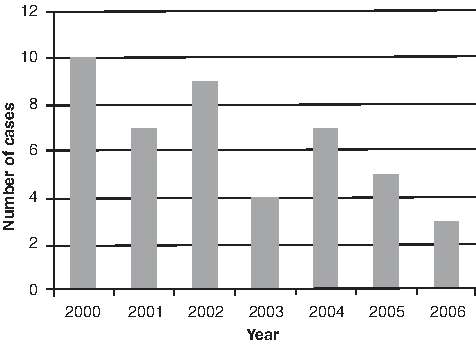
Off-season distribution of RSV-confirmed hospitalizations at Children's Hospital of Austin, May 2000 to September 2006, total count by year of admission.
RSV, respiratory syncytial virus. *NICU: neonatal intensive care unit; **RAD: reactive airway disease; ***Includes findings for pneumonia or bronchiolitis. p-value calculated using Pearson chi-square test.
Hospitalization characteristics
A full admission (≥24 hours) was required for 786 (92.5%) patients. The primary reasons for hospitalization were cough and respiratory distress (Table 1). Categorical observed characteristics of the hospital course due to RSV illness are listed in Table 1. An ICU admission was needed for 79 (9.3%) patients.
There were two deaths, both with a history of a NICU admission and comorbidities. One patient was admitted during the off-season, had received prophylaxis during the previous RSV season, and the primary cause of death was identified as respiratory failure. The other patient was admitted in January, did not receive prophylaxis, and the primary cause of death was multiple organ failure.
Off-season patient characteristics
A total of 45 (5.3%) patients were admitted during the off-season. There was no difference noted for patient gender or race when comparing the two seasons. Patients admitted during the off-season tended to be of younger gestational age; 33% were 36 weeks gestational age or less compared to 10% during the typical season. There was a statistically significant difference (chi-square, p<0.001) between the distribution of gestational age categories by season of diagnosis. Gestational age categories included babies born at less than 32 weeks gestation, between 32 and 36 weeks, and more than 36 weeks. During the off-season, 22.2% of admissions were born at less than 32 weeks gestation compared with only 4.6% of cases in the typical season (Table 1). Although not statistically significant, patients admitted during the off-season were chronologically older upon admission; mean of 8 vs. 10 months respectively. A comparison of notable patient characteristics, measured with continuous variables, between seasons is illustrated in Table 2. Babies who were premature (<36 weeks gestation at birth) were 4.35 times more likely than term infants to be admitted during the off-season (95% Confidence Interval [CI]: 2.2, 8.6). Patients with a history of multiple birth were 3.38 times more likely to be admitted in the off-season (95% CI: 1.24, 9.22; Table 3).
comparison of means using t-test. **Calculated for patient population admitted to ICU. ***Calculated for patient population requiring mechanical ventilation.
Outcome defined as RSV diagnosis during off-season.
A greater percentage of patients from the off-season had a history of NICU admission at birth. Patients with a history of NICU admission were 6.05 times more likely to have been admitted in the off-season (95% CI: 2.9, 12.5) when compared to those with no history of NICU admission (Table 3). Length of stay in the NICU was not statically significantly different by season.
A statistically significant difference was found between the two groups for birth weight. The data were categorized into very low birth weight, weighing less than 1,500 grams at birth and low birth weight babies, weighing 1,501 grams to less than 2,500 grams at birth. Chi-square tests showed statistically significant differences in both groups between the typical season and the off-season. The larger difference was seen in the very low birth weight group. In the off-season, 11.1% of babies admitted had a history of birth weigh less than 1,500 grams compared to only 3.2% in the typical-season. Additional variables listed in Table 1 were not found to be statistically significant.
Discussion
RSV infections in the United States typically occur during annual community outbreaks at regular, predictable intervals in the late fall, winter, and early spring. 3 Based on the definition of widespread RSV activity used by the National Respiratory and Enteric Virus Surveillance System (NREVSS), RSV outbreaks are rapid in onset and last 2–5 months. However, studies from South Texas and Southeastern Florida have found considerable variability in the RSV season from year to year.3,4 Between 1996 and 2007 in South Texas, Fergie et al. found that only one RSV season lasted 16 weeks (the average duration for the southern United States), with the median duration being 21 weeks. 5
There are two reports from regions in the southern United States of increased RSV illness during summertime months. In 1992, Washburn et al. reported a 21% incidence of RSV infection among children with respiratory symptoms during the summer in Louisiana over two consecutive years. 5 Their data showed no significant difference between degrees of illness. In Florida, Halstread et al. reported a persistent RSV epidemic between July 1993 and December 1996. 6 They concluded that RSV is endemic in that region and can be detected consistently during the summertime months. Similarly, Light studied Southwest Florida over a 4-year period and found RSV detected above epidemic levels in all but 6 out of the 48 months studied. RSV cases were still present during those 6 months, but did not reach the threshold considered by the NREVSS to be epidemic. 4 However, there is little data in the literature regarding these off-season illnesses.
Our goal is to compare RSV illness, which occurs during the typical winter epidemics, to the illness that occurs more sporadically during the off-season. Our data demonstrate that particular infants may be at risk for admission for RSV illness during the off-season. These infants were more likely to have been premature, have had low birth weights, have been the products of multiple births, or have a history of NICU admission. Severe RSV-related respiratory illness was observed during the off-season in our study, including the need for mechanical ventilation and prolonged ICU stay. Of note, among children admitted to the ICU, those admitted during the off-season remained in the ICU twice as long as those admitted during the typical season.
These results suggest that a group of children may remain at risk for RSV infection during the off-season, at a time that the virus is circulating at low levels. In an attempt to correlate RSV activity in relation to geographic climate, humidity, and weather patterns, Welliver found that RSV activity is nearly continuous throughout the year in subtropical regions with warm weather and high humidity. 7 Our institution is in a geographic locale that may predispose to such activity. Weather conditions that affect the viability of the virus may also explain the variability of off-season cases among the years. 8
A review of the RSV testing data over 10 years has been conducted to help define the variability in community RSV season timing. During the years 1990–2000, it was observed that the RSV seasons in the South began significantly earlier and lasted longer than seasons in the rest of the nation. 9 Beginning in 1999, mention is made regarding sporadic detections reported throughout the year to the National Respiratory and Enteric Virus Surveillance System.10–13
Texas has been compiling data from major centers providing care to children since 2004 regarding the results of RSV testing to attempt to define RSV epidemiology in our state. Our institution contributes to this. Although we do not have complete data for the period of time in this study, data from 2002 to 2006 show percent positive RSV test rates during the off-season ranging from 0 to 11%. 14 However, the relatively low total number of tests performed during the off season months may artificially inflate the percent positive.
This study is subject to several limitations. Our study is retrospective in nature, and limited to patients who were ill enough to be admitted; we do not have information regarding patients who may have had similar symptoms and were not admitted. We also do not have information about other viral infections that may have been circulating during the study period, and caused co-infection in the identified patients with RSV infection.
Another limitation of the study is the possibility of increased false positive diagnostic test results during a period of low prevalence of infection. This phenomenon is well described. 15 Due to the retrospective nature of the study, we do not have the benefit of a more complete evaluation for viral infection in these patients; rather, tests were as ordered by physicians based on clinical judgment.
Diagnostic methods for RSV infection include viral culture, rapid antigen capture assay, immunofluorescent staining, and polymerase chain reaction. The laboratory at our institution used RSV EIA as the most frequently used diagnostic method of testing during the study period, with proper procedures for result positive and negative controls. RSV culture may be insensitive and has been called into question for diagnosis.16,17 Methods of diagnosis such as polymerase chain reaction may be more sensitive, but were not widely available at our institution during the study period.
Conclusions
We found that particular infants may present with significant RSV infection in the off-season, at a time when RSV may circulate at low levels in certain geographic areas. 8 These infants were more likely to have been premature, have had low birth weights, have been the products of multiple births, or have a history of NICU admission. Pediatricians should be aware of the possibility of infection in such patients who present with a consistent clinical presentation.
Footnotes
Acknowledgments
We would like to thank Carey Bush, Olivia Hauger, Rebecca Wren, and Jaquelyn Marroquin who assisted with data collection. Financial support was provided by a grant from MedImmune, Inc.
Author Disclosure Statement
SBH and WG have received unrestricted grants from MedImmune, Inc. SBH has been a speaker for MedImmune, Inc regarding vaccines and RSV immunophrophylaxis. No competing financial interests exist for the other authors.