
Abstract
Background:
Fractional exhaled nitric oxide (FENO) levels are increased in children with asthma and in infants with recurrent wheezing, but the role of FENO in the acute phase of bronchiolitis is still not defined.
Objective:
The aim of this study is to evaluate FENO values in the acute phase of bronchiolitis, compare them with healthy infants, and relate those values with the appearance of other wheezing episodes.
Methods:
FENO values were determined in infants between 2 months and 2 years affected with RVS bronchiolitis by offline method. The FENO values collected in the acute phase were related with the respiratory clinical symptoms presented in the 2 years following the episode.
Results:
A total of 30 patients were recruited: 15 in the bronchiolitis group and 15 in the control group. The average of the FENO values in the acute phase was 18.74 ppb (range 2–88) in the bronchiolitis group, and 8.75 ppb (range 2–24) in the control group. However, these results showed no significant statistical differences (p=0.176). Nevertheless, we found a positive correlation between the FENO values and the clinical score (Downes) of the bronchiolitis episode (p=0.023). In infants that presented other wheezing episodes in the 2 years after, the average of FENO in the acute phase of the first episode was 23.1 ppb (average of 10.25 ppb) versus 8.4 ppb (average 5.4 ppb) in the group of patients with no other episodes. The comparison of averages has no statistical significance.
Conclusion:
We found no differences in FENO between infants with bronchiolitis and healthy ones. The FENO values in the acute phase seems to be related to the severity of the disease but do not predict the appearance of wheezing episodes in the following 2 years.
Introduction
Once its role in asthma had been established, the possible role in the handling of infants with recurrent wheezing appeared. In 1999, Baraldi et al. 3 showed that in the acute phase of exacerbation of infants with recurrent wheezing, the FENO values were higher and decreased to normal levels with corticosteroid treatment. Other more recent studies, such as Gabriele et al., 4 have shown that infants younger than 2 years with recurrent wheezing have higher FENO in comparison to healthy infants.
More than a third of children younger than 2 years suffer bronchiolitis. This condition has been described as the most frequent cause of childhood hospitalization in developed countries. 5 Respiratory sincitial virus (RSV) bronchiolitis in the toddler period is also a risk factor for later development of asthma. 6 The role of eosinophilic inflammation has been studied in those patients. The high levels of eosinophils and cationic protein (in blood7,8 and nasal secretions9,10) during the acute phase of bronchiolitis predict the appearance of other wheezing episodes. However, there is still little data on FENO values in the acute phase of bronchiolitis. A high FENO value in the acute phase could also be related with subsequent clinical symptoms, and offers another non-invasive marker that could help in the treatment and follow-up of these patients.
The two objectives of this study are: (1) to evaluate FENO values in the acute phase of infants with first episode of bronchiolitis and compare them with healthy infants; and (2) to relate those values with the appearance of other wheezing episodes.
Material and Methods
The study was divided into two parts in relation with the objectives.
Phase 1
The FENO values were determined in infants of ages ranging from 2 months to 2 years affected with the first wheezing episode associated to acute respiratory infection by RSV that came to the Emergency Room (ER) during the epidemic period between October and April 2007. The RSV infection was confirmed by positive inmunofluorescence test and culture of nasopharyngeal secretions. The measure of FENO was performed during the first 5 days of clinical respiratory symptoms (acute phase of the disease). We consider the start of illness depending on parental reports of respiratory symptoms. This index group was performed on patients with mild to moderate respiratory distress. No severe cases were included because the measurement of FENO is not compatible with oxygen therapy. In this way, the FENO values were collected in a control group of patients who were admitted to hospital not due to respiratory or infectious disease, and most were patients admitted for surgical intervention or neurologic studies. This control group had the same age range and was healthy from a respiratory point of view.
We excluded patients that had presented other wheezing episodes or suffered other chronic respiratory or cardiac diseases, those born preterm with fewer than 35 weeks of gestation, or those who had previously received treatment with oral or inhaled corticosteroids.
The clinical history (family medical records of asthma, maternal smoking during pregnancy, diagnosis of atopic dermatitis), as well as the severity score (Downes Score), are related with the FENO values obtained in the two groups. The study was approved by the local ethics committee. Parents were informed both verbally and in writing, and informed consent was collected from all patients.
To measure the exhaled nitric oxide, we used the offline method with patients breathing to tidal volume, according to American Thoracic Society/European Respiratory Society (ATS/ERS) recommendations. 11 We collected the exhaled air by means of a facemask. A manual pressure was exerted around the edge of an inflatable mask to avoid air leaks. The mask was connected to a bag of inert material (Tedlar; Cole-Parmer Instrument Co, London). The baby was awake and in the arms of the mother breathing quietly in a compliant manner. The control of the atmospheric nitric oxide was performed by rejecting the samples where the atmospheric nitric oxide was higher than 10 ppb. The resistance of the system (measured previously) was of 5 cm H2O, which avoids the nasal contamination by means of closing the soft palate. Later, the measurement was performed by chemiluminescence by means of a Sievers Instruments (Boulder, CO) 280i NOA analyzer. The time between sample collection and analysis was always less than 12 h according to standard recommendations.
In five patients from each group, we measured the FENO values in two independent samples, checking measurement reproducibility. In all cases, the difference between the two samples was less than 5%.
Phase 2
Follow up of the patients recruited in the first phase was carried out prospectively for 2 years. The annual numbers of wheezing episodes during this period, as well as other clinical and epidemiological data of interest based on the questionnaire derived from the Phase 3 ISAAC study, were telephonically registered.
The FENO values collected in the acute phase of bronchiolitis (phase 1) were related with wheezing episodes diagnosed by a clinician in the 2 years following the first one. We divided the bronchiolitis group into patients that presented new wheezing episodes and those that did not.
In the case of qualitative variables (e.g., presence or not of wheezing), a comparison of the measures was performed by means of a non-parametric test. In the case of quantitative variables (e.g., number of wheezing episodes in the following 2 years), correlation was found by means of the Spearman test.
We used statistical software SPSS version 12.0 (SPSS, Inc., Chicago, IL).
Results
A total of 30 patients were recruited in the first phase: 15 in the bronchiolitis (9 males) and 15 in the control group (eight males). In the bronchiolitis group, the average age was 3 months, and in the control group 4 months. There was no statistical difference in epidemiological data between the groups (see Table 1). The variables associated to the predictive asthma index described by Castro 12 were analyzed with no differences between the groups. There was no difference in the ambient nitric oxide (NO) between the groups.
SD, standard deviation; NO, nitric oxide.
The average of the FENO values in the phase 1 was 18.74 ppb (range 2–88) in the bronchiolitis group and 8.75 ppb (range 2–24) in the control group, but these results showed no significant statistical differences (p=0.176; see Fig. 1).

Exhaled nitric oxide (NO) levels in children with acute phase of bronchiolitis and control group.
No correlation between the FENO values, in acute phase of bronchiolitis, and atopia or maternal smoking during the pregnancy was found.
The median Downes score in the index group was 3.6 (range 2–7), which correlates with mild to moderate distress. A positive correlation between the FENO values and the clinical score (Downes) of the bronchiolitis episode was found (p=0.023).
In the second phase of the study, the follow-up on 15 patients from the bronchiolitis group and 13 from the control group was completed. From the collected data, we controlled variables such as the kindergarten attendance and the number of siblings (see Table 2).
In infants that presented other wheezing episodes in the 2 years after, the FENO average in the acute phase of the first episode was 23.1 ppb (median of 10.25 ppb) versus 8.4 ppb (median 5.4 ppb) in the group of patients with no other episodes. Nevertheless, the observed differences were not statistically significant (p>0.05; see Fig. 2).
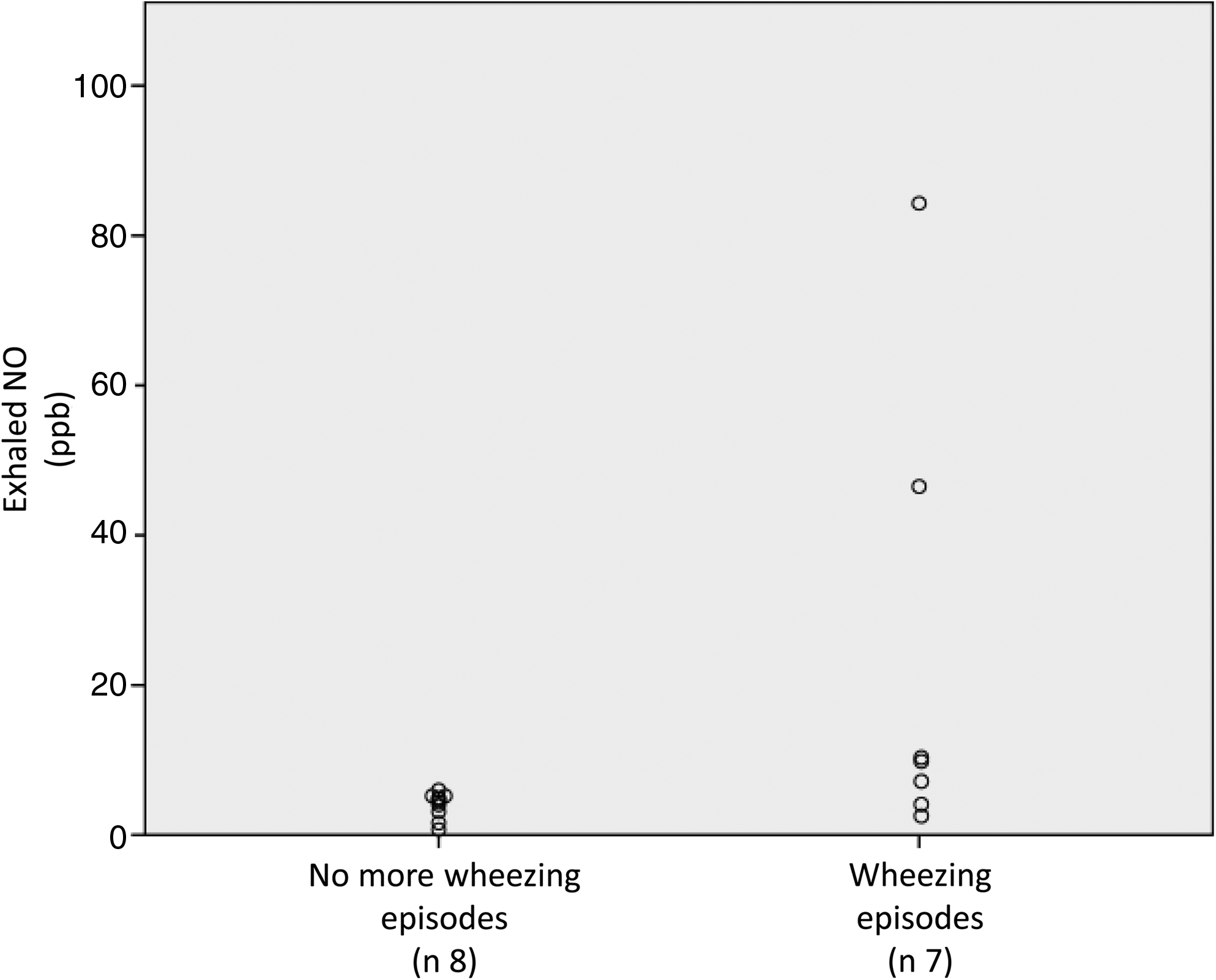
Exhaled nitric oxide levels measured in acute phase of bronchiolitis in children with or without other wheezing episodes.
Discussion
We found no statistical differences in the FENO values between the bronchiolitis group and the control group. Despite finding greater mean values in the bronchiolitis group, the sample size is not enough to confirm these differences. The FENO values in the acute phase seem to be related to the severity of the disease, but they do not predict the appearance of wheezing episodes in the following 2 years.
The inflammatory bronchial response in acute infection is variable. The discussion as to whether the immune response during the acute infection by RSV is predominantly Th1 or Th2 is still open. However, it has been described how the in vitro stimulation of the epithelial bronchial infection by RSV provokes the recruitment and degranulation of eosinophils. 13 A recent study suggests that the alpha tumoral necrosis factor could play an important role in this eosinophilic inflammation of the bronchial mucosa. 14 It has been related with the appearance of respiratory symptoms during the 2 months following the infection. 10
Sigurs et al. 15 followed up of patients who were hospitalized due to RSV bronchiolitis during the first year of life and compared the incidence of asthma, recurrent wheeze, and allergy disease with healthy patients. They found an increased prevalence, at the age of 18, of asthma/recurrent wheezing (39% vs. 9%), clinical allergy (43% vs. 17%), and sensitization to perennial allergens (41% vs. 14%). This again suggests the role of RSV in allergic diseases.
The studies in the literature that show the FENO values in the acute phase of bronchiolitis are scarce and with very different results. Ratjen compared the FENO values in the acute phase of bronchiolitis with the values of healthy and preterm children. He found lower FENO values in the acute phase of bronchiolitis with respect to the other groups. 16 Gadish et al. 17 obtained the same results. They measured fractional FENO levels in infants during acute respiratory syncytial virus (RSV) bronchiolitis and during convalescence, and their study shows that FENO levels during acute RSV bronchiolitis are significantly decreased and levels increase back to normal levels and beyond during convalescence.
Baraldi 3 carried out measurements of FENO in three groups: acute phase of wheezing in a group of patients with other previous episodes, acute phase in first episode of wheezing, and a control group of healthy children. With a similar sample size to ours, in this study they found significant differences between the group of recurring wheezing and the healthy patients. However, this was not the case between the group of first wheezing episode and healthy children. Neither of them relates the FENO values during the acute phase of the first episode with the respiratory clinical symptoms in the successive months.
The measurement of FENO by the offline method has been standardized since the ATS recommendations in 2005. 11 However, the offline method, used in this study, with patients breathing to tidal volume, could be criticized for the absence of flow control. The variability of results (standard deviation for sample 6.8 ppb) could be explained by this. This measurement system is less reliable than the online method but is the most feasible in clinical practice. The flow control demands a sedation that in our group of patients with respiratory distress would not be either recommendable or ethically justifiable. Other works have used this method in patients with similar characteristics, demonstrating the usefulness of the technique. 18
The relation between atopia and FENO has been described since the first months of life. In infants with a history of maternal atopia, the FENO values after birth have been related with an increase of the risk of having respiratory symptoms in the following years. 19 These records modify the effect of other wheezing risk factors, such as maternal smoking. 20 Moeller 21 with a wide sample of 391 patients showed that, in a group of patients until 4 years with recurring wheezing, those who had a predictive index of positive asthma 12 (history of atopia etc.) presented higher FENO values than those with a negative one. At 4 years, those patients diagnosed with atopia or asthma also presented higher FENO values than the healthy patients. 22
Tepper compared the FENO values in children with a history of allergy to eggs or milk in the first 2 years of life and no episodes of previous wheezing with those not sensitized, and there were no significant differences. 23 These data show that a background of atopia and bronchial hyperactivity are related to FENO values. In our study, we cannot demonstrate that patients with a background of atopia present high values of FENO in the acute phase of the first episode.
It is interesting to note the correlation observed between the clinical score of the acute episode and the FENO values. This finding could be explained from two points of view: (1) greater eosinophilic inflammation means more severe disease and (2) more severe disease means more obstruction of the airway, which is related to less flow and thus higher FENO values. 24
The infants that presented later wheezing episodes already presented higher FENO values in the first table. This group could include the asthma phenotype of the adult, which presents high FENO values, and this marker is useful both in the diagnosis and the control of the illness. 25 The consistency of these data is limited by the absence of statistical significance that we mainly attribute to the lack of sample. This sample based on previous similar studies3,17 was insufficient to determine significant differences but it does show a clear trend in the FENO values. After analyzing the results, we calculated the sample size that would be necessary to determine statistical significance with this study design, and we would need 42 patients in each group (alpha error level 5%, beta error level 20%).
The results of the related studies, some of them with opposite findings, suggest that the lack of standardized technique in this group of age. Gabriele et al. 26 in a recent review describe how several factors related to the measurement conditions have been found to influence values. Expiratory flow, which can be related with severity of respiratory distress, the ambient NO, and nasal contamination should be controlled. Furthermore, the exposure to pre- and postnatal risk factors for respiratory morbidity has been shown to influence FENO values. FENO measurements in this group can be useful, but it is important to evaluate and control these factors.
The acute phase of bronchiolitis (or first wheezing episode) has a similar route in the majority of the infants, but its later evolution and the appearance of the so-called “postbronchiolitis hyperactivity” is nowadays difficult to predict.
We believe that non-invasive markers such as FENO could help in the handling of these infants. Its measurement by means of the offline method to current volume is minimally invasive and compatible with the clinical state of the patient.
The results of this study show that a group of patients affected by positive RVS bronchiolitis could present eosinophilic inflammation from the first episode. These findings could be related with a greater risk of presenting later episodes. Early detection in these patients could help both in the management of acute episodes and also later handling.
Other similar studies are necessary with a larger number of patients and standardized technique of FENO measurement. It could open new perspectives in the handling of such a prevalent condition as recurring wheezing episodes.
Footnotes
Author Disclosure Statement
This work was supported by a grant of Carlos III Institute (Spain). FIS 00/0450.