
Abstract
Relapsing polychondritis (RP) is a rare multisystem disorder characterized by inflammation and destruction of cartilaginous tissue. Atypical initial symptoms and signs may cause difficulties in the diagnosis of RP for pediatricians. In this article, we report a 9-year-old male who presented with stridor and hoarseness indicating upper respiratory tract involvement in the setting of chronic polyarthralgia. Flexible bronchoscopy revealed subglottic stenosis. Increasing awareness of early respiratory manifestations of RP will prevent life-threatening complications.
Introduction
Case
A 9-year-old boy was referred to our clinic with a history of recurrent dyspnea, stridor, and hoarseness in the previous 3 months. His medical history revealed that he had had polyarthralgia of the major joints during the last 6 months, which had been diagnosed as reactive arthritis and treated with non-steroidal anti-inflammatory drugs with partial relief. His respiratory complaints were unresponsive to inhaled bronchodilators and inhaled corticosteroids. Increased work of breathing was noted even during sleep. Review of systems was unremarkable other than the respiratory symptoms and polyarthralgia. He had no fever, dysphagia, or muscle weakness. The rest of the past history was unremarkable. He had no risk factors for tuberculosis. Family history, as well as personal, social, and environmental histories, were non-contributory. Hoarseness was evident in the initial encounter; physical examination findings including vital signs and anthropometrics were within normal limits. Examination of the joints revealed no deformities, limitation of motion, or tenderness.
Presenting symptoms of the patient were indicative of airway involvement. In the setting of a chronic history of polyarthralgia, differential diagnoses included systemic diseases with airway involvement, as well as airway compression from intrathoracic mass secondary to lymphadenopathy from tuberculosis or sarcoidosis. Initial laboratory testing revealed normal blood count and differential. Erythrocyte sedimentation rate was elevated at 64 mm/h. Urinalysis was normal. Chest X-ray and spirometry were normal. Tuberculin skin testing revealed an induration of 8 mm. Given the prominent upper airway symptoms, flexible bronchoscopy was performed. Nearly 50% narrowing just below the vocal cords was observed (Figs. 1 and 2). The patient was then referred to the pediatric rheumatology and otorhinolaryngology departments for further evaluation. Further diagnostic testing was performed. Immunoglobulin A, G, and M were normal for age. Major laboratory markers for rheumatologic diseases such as rheumatoid factor, anti-nuclear antibody, perinuclear and cytoplasmic anti-neutrophilic cytoplasmic antibodies were negative. Ultrasound of the abdomen was within the normal limits.

View of the larynx showing the narrowing of the glottic area with fibrosis. Color images available online at www.liebertonline.com/ped
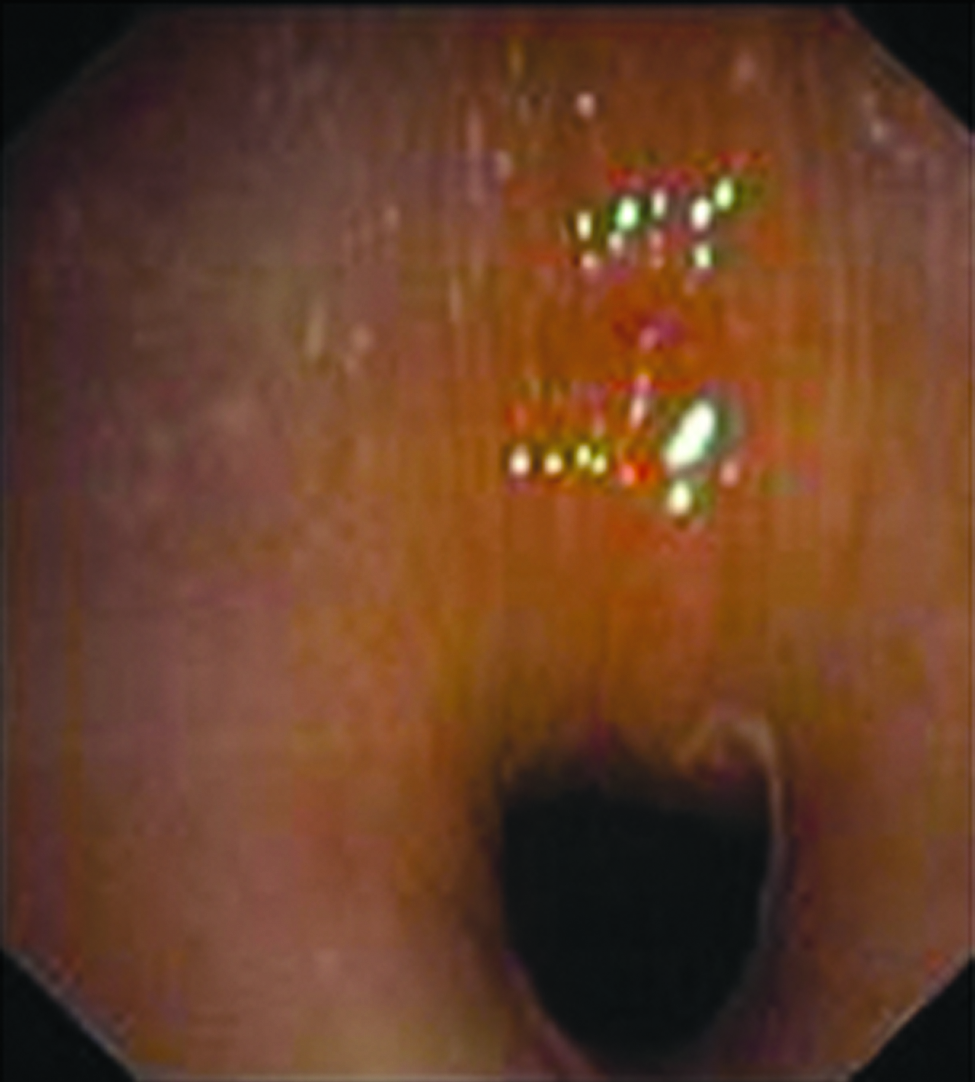
Closed view of bronchoscopic image of nearly 50% occlusion of the glottis with fibrosis just below the vocal cords. Color images available online at www.liebertonline.com/ped
Fifteen days after the bronchoscopy procedure, the patient was seen at the emergency department with sudden onset of respiratory distress necessitating emergent tracheotomy. He was admitted and a tracheostomy tube was inserted. In the interim, he had developed biauricular chondritis and saddle-nose deformity. He was diagnosed with RP according to the criteria established by McAdam et al. 1 High dose steroids in the form of metylprednisolone (30 mg/kg/day) were given for 3 days followed by a tapering regimen. He was discharged after 25 days. He has been followed at the Pulmonary, Rheumatology and Otorhinolaryngology Clinics for 2 years now and maintained on 0.5 mg/kg/day of prednisolone and 2.5 mg/day of methotrexate. He remains tracheostomized and receives regular pulmonary toilet and chest physiotherapy with no complications of tracheitis or lower respiratory tract infections. He is ambulant, maintains an active life, and attends school.
Discussion
RP is a connective tissue disorder characterized by widespread destructive inflammatory lesions of cartilaginous structures throughout the body. 4 Although onset may vary from birth to the ninth decade, only a few cases have been reported in childhood. 2 The diagnosis of RP is empirically established by the presence of three or more of any of the following features: (1) bilateral auricular chondritis; (2) nonerosive seronegative inflammatory arthritis; (3) nasal chondritis; (4) ocular inflammation; (5) respiratory tract chondritis; or (6) audio-vestibular damage. 1 A biopsy is unnecessary in most cases. 4 More than half of the patients reported have been found to have respiratory tract manifestations. The larynx and upper trachea are affected most frequently, but the disease may involve subsegmental airways.5,6
Various diseases can cause inflammatory or granulomatous lesions of the larynx and subglottic region, including Wegener granulomatosis, sarcoidosis, tuberculosis, amyloidosis, and rheumatoid arthritis. 6 In our patient, there were no findings suggesting vascular and renal involvement, which excluded a possible diagnosis of Wegener granulomatosis and amyloidosis. Furthermore, there was no history of chronic sinusitis and rheumatologic markers such as rheumatoid factor, anti-nuclear antibody, perinuclear and cytoplasmic anti-neutrophilic cytoplasmic antibodies were negative. The diagnosis of pulmonary tuberculosis was excluded in the absence of risk factors or tuberculous contacts, unremarkable PPD test, and chest X-ray findings. The absence of lymphadenopathy on exam and unremarkable chest X-ray excluded sarcoidosis. Our patient was diagnosed with RP based on the presence of bilateral auricular chondritis, nonerosive seronegative inflammatory arthritis, nasal chondritis, and tracheal chondritis.
When the initial manifestation of RP is respiratory, there will be a delay in diagnosis in most cases. The clinical symptoms, which include cough and dyspnea only partially responding to steroids, are nonspecific and usually attributed to more common diseases such as asthma and infectious processes such as acute tracheobronchitis or acute bacterial membranous tracheitis. 7 The sensitivity of conventional chest radiography is not high enough for an accurate visualization of tracheobronchial chondritis. Physical examination is often unremarkable, and when there is an abnormal finding it is most commonly stridor. In our patient, flexible bronchoscopy was performed given the prominence of upper airway symptoms and revealed subglottic stenosis. Bronchoscopy is useful in elucidating the nature and severity of airway involvement in RP.8,9 Inflammatory and fibrotic alterations of the mucosa, as well as tracheobronchial stenosis and collapse, are characteristic bronchoscopic findings. 5 Involvement of the airways in RP can lead to obstruction during the active stages of the disease due to inflammation; dissolution of the tracheal or bronchial cartilage and scarring can occur during the later stages of the disease. Tracheal and bronchial obstruction is often complicated by pulmonary infections due to impaired airway clearance, which are responsible for approximately 50% of mortalities. 10 Our patient in fact required emergent tracheotomy and eventual placement of a tracheostomy tube shortly after initial presentation to our clinic.
Most cases of relapsing polychondritis can be managed medically, including patients with airway involvement. Treatment with corticosteroids alone, or in combination with other immunosuppressive agents, has been traditionally employed. Although its efficacy has not been assessed in randomized trials, it is the most effective treatment and can result in a dramatic response. Optimal dose and duration of therapy has not been systematically evaluated. A reasonable regimen is 1 mg/kg/day of prednisolone once daily for 8–12 weeks followed by a tapering regimen to the lowest dose possible while maintaining disease control. Lifetime treatment may be necessary in patients with aggressive disease. Drugs such as cyclophosphamide, dapsone, azathioprine, and methotrexate have been considered for their steroid-sparing effect. 4 Approaches to treatment of airway involvement are varied. In disease limited to the larynx and upper trachea, a tracheostomy may be performed. Other invasive techniques include placement of endobronchial polymeric silicone stents to help maintain airway patency. 7
In conclusion, respiratory manifestations, specifically that of stridor signifying upper airway involvement, may be the presenting symptom that brings a patient to the attention of a physician even in the setting of more chronic rheumatologic symptoms. Respiratory obstructive complications can result in significant morbidity and mortality in patients with RP, in and of itself, a rate autoimmune syndrome and infrequently diagnosed in children. Flexible bronchoscopy is a useful tool in rapid and accurate diagnosis among patients with persistent and atypical stridor and in this case, contributed to the diagnosis of RP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.