
Abstract
The 6 Minute Walk Test (6 MWT) has been shown to be a better test for submaximal exercise capacity than other submaximal exercise tests. The cystic fibrosis (CF) Health-Related Quality of Life Cystic Fibrosis Questionnaire-Revised (CFQ-R) has been used in CF patients in order to assess the quality of life. There are a few studies that examine measurements of multiple endpoints simultaneously [e.g., pulmonary function test (PFT), exercise capacity, CFQ-R] with treatment in CF pulmonary exacerbation. We hypothesize that the 6MWT is safe to perform during pulmonary exacerbation, and that 6 MWT, CFQ-R, and PFT improve with treatment in CF pulmonary exacerbation. We further hypothesized that the improvements in 6MWT, CFQ-R, and PFT are related. We performed 6 MWT, PFT, and CFQ-R in 21 CF subjects (age 7–20 years) admitted for pulmonary exacerbation. 6 MWT, PFT, and CFQ-R were completed at admission, at the end of week 1, and at the end of week 2. No complications were noted during the 6MWT.The 6MWT, PFT [forced expiratory volume in one second (FEV1), FVC and forced expiratory flow25%–75% (FEF25%–75%)], and CFQ-R domains (Respiratory and Physical) improved significantly at week 2. The physical domain change correlated with the 6MWT improvement, whereas the respiratory domain change correlated with the FEF 25%–75% improvement at week 2. There was no significant relationship observed between the 6MWT and PFT improvements. In conclusion, 6MWT is a safe and well-tolerated test, and it can be utilized as an adjunct or alternative outcome measure to PFT in acute CF pulmonary exacerbation. In addition, multiple outcome measures, including 6MWT and HRQOL, should be utilized to assess the efficacy of treatment in CF pulmonary exacerbation.
Introduction
The 6 Minute Walk Test (6 MWT) is a simple and inexpensive test that reflects overall fitness and the activities of daily life.3,4 It is easier to administer, more reflective of activities of daily living, and better tolerated than the other walk tests such as shuttle walk test and so on.3,5 It has been widely used to evaluate submaximal exercise capacity in adults with lung diseases,6–10 but it is used less commonly in the pediatric population. A significant correlation has been shown between 6MWT distance and peak oxygen uptake (V'O2 max) in children, suggesting that the 6MWT may be used to measure aerobic fitness. 11 Previous studies have also documented that 6MWT is a reliable and valid test in children with CF.12,13 However, it has not been examined in CF pulmonary exacerbations as an outcome measure of acute improvement with treatment.
The CF Health-Related Quality of Life Ouestionnaire (HRQOL) has been used in CF patients to assess the effect of the disease on the quality of life.14,15 However, its use as an objective outcome measure of treatment in acute pulmonary exacerbation has not been tested as thoroughly. 16 The U.S. Food and Drug Administration has also encouraged the use of patient reported outcomes in studies of patients with chronic disease and, thus, the inclusion of these outcomes in an exacerbation study provides critically needed information about these measures. There are even fewer studies that have examined the change in lung function, exercise capacity, and HRQOL as outcome measures of treatment in pulmonary exacerbation as a whole. 17 Moreover, none of these studies have used 6MWT, which is a better test for assessing submaximal exercise capacity, compared with other functional tests.
Thus, in this pilot study, we aim at investigating (a) whether 6MWT is a safe test to be performed during CF pulmonary exacerbation; (b) how 6 MWT, HRQOL domains score, and PFT change with treatment in CF patients hospitalized for pulmonary exacerbation. (c) Do the changes in 6MWT, HRQOL domains, and PFT correlate with each other? We hypothesize that the 6MWT is safe to be performed during CF pulmonary exacerbation and that 6MWT, HRQOL domains score [using Cystic Fibrosis Questionnaire-Revised (CFQ-R)], and PFT improve with treatment in CF patients hospitalized for pulmonary exacerbation. We further hypothesize that the improvements in 6MWT, CFQ-R domains, and PFT correlate with each other.
Methods and Materials
Subjects
Twenty-two subjects with CF (ranging in age from 7 to 20 years) who were admitted between December 2008 and August 2009 to the Children's Hospital Los Angeles (CHLA) with the diagnosis of pulmonary exacerbation were recruited. All patients were recruited consecutively. Twenty-three patients were approached for this study based on age criteria; however, 1 patient declined to participate in the study. The CHLA institutional review board approved the study (CCI-08-00210), and written informed consent was obtained from the patients/parents and/or legal guardians. Assent was also obtained from appropriate subjects. A respiratory culture was obtained from each subject on admission. Respiratory culture data were recorded based on the culture results from 1 year earlier until this admission. Pseudomonas aeruginosa was defined as being multi-drug resistant if it was resistant to all agents in at least two of the following groups of antibiotics: β-lactams, aminoglycosides, and fluroquinolones. Patients were treated as per published guidelines for the treatment of CF pulmonary exacerbation. 18
6 minute walk test
The 6MWT was conducted as per the American Thoracic Society guidelines. 3 It was conducted within 3 days of admission, then at the end of week 1, and at the end of week 2. All patients received the same orientation before each testing session. The patients were instructed to walk as far as possible in 6 min on a standard indoor course, and the total distance walked was measured at the end. Oxygen saturation (SpO2) and heart rate were recorded before and immediately after the 6MWT using a pulse oximeter (Nellcor, Hayward, CA).
Cystic fibrosis questionnaire—revised
The CFQ-R is a self-reported reliable and validated HRQOL measure that is specifically designed for patients with CF.19,20 It consists of 44 items on 12 generic and disease-specific scales. The CFQR-child version (6–13 years old) and the CFQ-R Teen/Adult Version (14 years and older) were used in this study. The CFQ-R child version has eight domains: Physical, Emotional, Social, Body Image, Eating, Treatment Burden, Respiratory, and Digestion. In addition to these eight domains, the CFQ-R Teen/Adult version has the following four domains—Role, Vitality, Health Perception, and Weight. The scores in each domain range from 0 to 100. The better HRQOL is represented by a higher score. The CFQ-R was completed by the patients on the day of each 6MWT session.
Pulmonary function tests
PFT were measured within the first 3 days of admission and at least weekly thereafter until discharge. Tests were performed in the pulmonary function laboratory of the Children's Hospital Los Angeles, located near sea level. The maximum expiratory flow rates (FEV1, FEF25%–75%) and forced vital capacity (FVC) were obtained using a computerized spirometer (Creative Biomedics International, San Clemente, CA or Viasys Sensor medics VMAX system, Yorba Linda, CA). The lung volumes were measured with a body pressure plethysmograph (Sensor medics 2800Autobox, Yorba Linda, CA). The values were collected as raw values and as a percent of predicted values based on standard reference values.21,22
Statistical analysis
Data were described using mean, standard deviations, and ranges. The change in variables from admission to the end of week 2 was evaluated using a paired t-test. Data were further divided on the basis of age to assess the effect of age on improvements in PFT and 6MWT, and analyzed using a two-sample t-test. Spearman's rank correlation was done to examine the association among changes in 6MWT, CFQ-R domains, and PFT at the end of week 2. Comparisons among various distributions of 6MWT, FEV1, and CFQ-R domains (Physical and Respiratory) from admission to week 1 and week 2 were illustrated using box plot graphs. A P-value of<0.05 was considered statistically significant.
Results
Data from 21 CF subjects (10 males, age range 7–20 years, 15 Hispanics, 5 Caucasians, and 1 African American) were analyzed (Table 1). One subject was excluded from data analysis because of incomplete data points. The mean FEV1 at admission was 56.2%±19.7% predicted with a range of 26%–103% predicted, indicating the wide range of severity of illness in our subject population. Thirteen patients showed colonization with pseudomonas aeruginosa, and seven of these patients had multi-drug-resistant pseudomonas. Five subjects were colonized with Achromobacter xylosoxidans, whereas only one subject was colonized with methicillin-resistant staphylococcus aureus.
BMI, body mass index; FVC, Forced vital capacity; FEV1, forced expiratory volume in one second; FEF 25%–75%, forced expiratory flow 25–75%; RV, residual volume.
No complications were noted during the 6MWT. All subjects were able to complete the test at admission, at week 1, and at week 2. Subjects tolerated the procedure well with no significant dyspnea or fatigue. There were no significant episodes of hypoxemia or tachycardia noted immediately after the test. The mean SpO2 at the beginning of 6MWT done at admission was 95.9±2.9, which was not significantly different from that at the end of the test (95.9±2.8; P=0.92). The mean heart rate increased from 103.9/min to 107.4/min (P=0.042) at the end of the test, which, although statistically significant, is unlikely to have clinical importance.
Figure 1 shows the serial plot of 6MWT for each subject. There was an individual variation at the end of week 1, but all subjects (except one) showed improvement at week 2 as compared with on admission. Mean 6MWT continued to improve from admission to the end of week 2 (Table 2 and Fig. 2). As expected, FEV1, FVC, and FEF25%–75% also improved from admission to the end of week 2 of IV antibiotics (Table 2 and Fig. 2). In addition, the physical and respiratory domains of CFQ-R improved significantly from admission to the end of week 2. (Table 2 and Fig. 2).
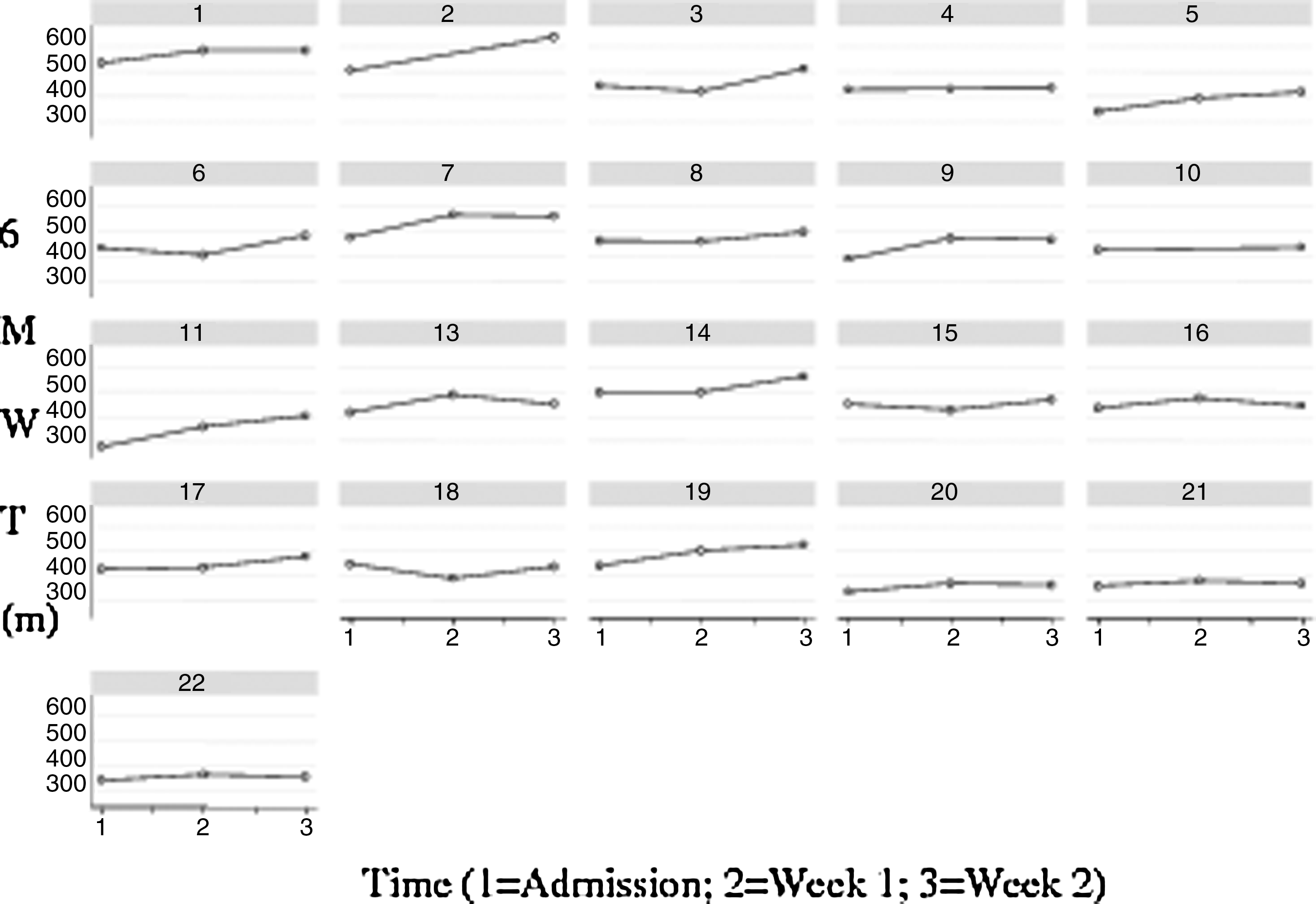
Serial 6MWT plot of each subject from admission to the end of week 1 and week 2. 6MWT, 6 Minute Walk Test.

Comparison among various distributions of
Week 2 variables compared with admission (Paired t-test).
Significant P-value < 0.05.
6MWT, 6 Minute Walk Test; CFQ-R, cystic fibrosis questionnaire–revised.
In order to assess the potential effect of age on the observed changes in 6MWT, the subjects were divided into two groups of < 12 years or ≥ 12 years. Both groups had comparable FEV1 (% predicted) at admission. In < 12 years age group, two out of seven patients had pseudomonas aeruginosa, and both these subjects had multi-drug-resistant pseudomonas. In older children, 11 out of 14 were psuedomonas aeruginosa positive. Five of these 11 patients had multi-drug-resistant psuedomonas. Children younger than 12 years showed substantial improvement in FEV1 with treatment but did not show as substantial improvement in 6MWT when compared with older subjects. In contrast, while older children (≥12 years) showed substantial improvement in 6MWT, they did not display the degree of improvement in FEV1 seen in the younger age group (Table 3).
Change (% change) from admission to week 2.
Comparison between the 6MWT change and the FEV1 change between groups.
Significant P-value<0.05.
To assess the relationship among changes in 6MWT, PFT, and CFQ-R at the end of week 2, Spearman Correlation was performed. Although both 6MWT and PFT parameters improved significantly compared with at admission, there was no significant correlation found between the change in 6MWT and the change in any PFT parameter. The improvement in 6MWT was significantly correlated with the physical domain of CFQ-R at the end of week 2. (r=0.48, P=0.029). There was a significant correlation found between improvements in FEF25%–75% and the respiratory domain of CFQ-R after 2 weeks of IV antibiotics (r=0.45, P=0.038; spearman correlation). At the end of week 2, the relationship between changes in FEV1 and the CFQ-R respiratory domain was moderate but did not reach statistical significance (r=0.38, P=0.08).
Discussion
Our study showed that the 6MWT is a safe and well-tolerated test in CF patients hospitalized for pulmonary exacerbation. The 6MWT, PFT parameters (FEV1, FVC, and FEF25%–75%), and CFQ-R domains (respiratory and physical domains) improved significantly with treatment. After 2 weeks of IV antibiotics, the change in the CFQ-R physical domain correlated with the 6MWT improvement, whereas the change in the respiratory domain correlated with an improvement in FEF25%–75%. However, there was no significant relationship seen between 6MWT and PFT improvements.
There are limited studies in the literature evaluating the utility and safety of the 6MWT in CF patients, especially in the pediatric population. In adults, Chetta et al. concluded that cystic fibrosis patients with mild to moderate lung disease experienced a significant fall in oxygen saturation and an increased breathlessness perception during 6MWT. 23 With regard to children, Rubinowicz et al. performed 6MWT in CF patients for four consecutive years along with spirometry and clinical parameters. They concluded that CF patients had significant desaturation during the test. 24 However, none of the studies just mentioned were performed during an acute pulmonary exacerbation, which is an important component of CF disease. To our knowledge, our study is the first study that objectively assesses the usefulness of 6MWT as a clinical outcome in CF pulmonary exacerbation. Despite the fact that our subjects were acutely ill, the 6MWT was well tolerated, and no complication was noted, including hypoxemia.
Previous investigators have assessed changes in sub-maximal exercise capacity in CF children hospitalized for pulmonary exacerbation. Cox et al. showed that the multiple shuttle test performance improved in CF hospitalized children, which is similar to our results. 25 They also observed an improvement in FEV1 but did not find any significant correlation between the change in multiple shuttle test performance and FEV1. Similarly, Pike et al. demonstrated an improvement in exercise tolerance (using the 3 min step test) as well as lung function (FEV1, FVC, and FEF25%–75%) in pediatric patients with CF admitted for pulmonary exacerbation. 26 For our study, we chose 6MWT, because it has shown to be superior to other functional tests in assessing sub-maximal exercise capacity.3,5
We also measured HRQOL (using CFQ-R) in these patients to assess the impact of treatment on the quality of life. Although CFQ-R is frequently used in the outpatient setting as a HRQOL measure, it has not been utilized thoroughly in acute settings of pulmonary exacerbation.14,15 In a previous study done during CF pulmonary exacerbation, Modi et al. showed that the respiratory domain score improved significantly after IV antibiotic treatment, which is consistent with our results of improvement in physical and respiratory domains. 16 We also observed in our subjects that the change in the CFQ-R physical domain correlated with the 6MWT improvement, whereas the change in the respiratory domain correlated with the improvement in FEF25%–75%. This may be due to the fact that 6MWT assesses the overall fitness, whereas the PFT measures the ventilatory function only. Quittner et al. in a study done on CF patients with pulmonary exacerbation reached a similar conclusion that CFQ-R measures different aspects of clinical efficacy as compared with those measured by physiologic variables. 27 Thus, using one test as an outcome measure for the treatment of pulmonary exacerbation may not be adequate.
We did not observe any significant correlation between the improvement in PFT parameters and the 6MWT distance. Interestingly, we demonstrated that the pattern of improvement in 6MWT and FEV1 differed in children younger than 12 years and 12 years and older, even if they had similar baseline FEV1, which suggests that there may be an interaction between 6MWT and age. In addition, this difference could be due to the fact that PFT is an assessment of ventilatory function only, whereas 6MWT assesses functional capacity, which is influenced by not only ventilatory function but also cardiovascular, muscular, inflammatory, and metabolic factors. There is evidence that intolerance to exercise in patients with CF is multifactorial, and that pulmonary function, nutritional state, and bronchial colonization agents play a role in that regard.17,26,28 This highlights the fact that simply relying on one test as an outcome measure may provide incomplete information. Multiple outcome measures can provide a better and more complete picture that provides further direction in clinical decision making. Particularly, we have observed that an important subset of patients with severe CF disease may display minimal change in PFT parameters with the treatment of acute exacerbation. In these individuals, the 6MWT and CFQ-R can be used to assess the response to treatment along with PFT. Hence, 6MWT and CFQ-R can be a useful adjunct to PFT in assessing overall clinical improvement in CF patients hospitalized for pulmonary exacerbation.
There are very few studies in the literature examining the measurement of multiple measures simultaneously (e.g., change in PFT, exercise capacity, and HRQOL) with IV treatment in CF pulmonary exacerbation. Bradley et al. performed pulmonary function testing, modified shuttle testing, and an HRQOL questionnaire in adult CF patients hospitalized for pulmonary exacerbation to assess the effect of IV treatment with multiple outcome measures. 17 There was significant improvement in lung function, exercise capacity, and quality of life after treatment, which is similar to what was observed in our study. However, this study was done in older patients (mean age 23 years) in contrast to our study, where we had a younger population (mean age 13.1 years). This study along with our study provides evidence that exercise capacity and HRQOL should be included along with PFT in the overall assessment of CF pulmonary exacerbation treatment. So far, the most commonly used objective measure of the end point of treatment is PFT only, which may provide a limited index of the outcome.
A significant number of subjects in our study were Hispanics (71%). This is the strength of the study given the relative paucity of data on patients with CF who are non-Caucasians. The training effect of 6MWT can be a potential limiting factor of our study. There is literature on adults that describes the possible effect of training on 6MWT performance.29,30 However, in these studies, the 6MWT was done on consecutive days. We believe that in our subjects, the training effect may not have such a significant impact, because the tests were conducted a week apart. Moreover, in our study, the orientation was provided before each test, which we expect to have also minimized the training effect to a certain extent. A potential limitation of our study relates to assessment of the 6MWT change based on published normative pediatric values of 6MWT. 31 All male and female subjects (except one) in our study were below the 3rd percentile on the reference percentile curves for normal children. Thus, it was not practical to assess the change based on normative values. However, we do not believe that the inability to normalize the data significantly impacts the validity of our results. In this study, each subject functioned as his or her own control, and correlations were executed across the tests carried out for each subject. A final limitation relates to our sample size, which was not sufficient to assess the effect of age, gender, and ethnicity on the relationship among changes in 6MWT, CFQ-R domains, and PFT with treatment.
In conclusion, the 6MWT is a safe and well-tolerated test, and it can be utilized as an adjunct or alternative outcome measure to pulmonary function testing in CF patients hospitalized for pulmonary exacerbation. In addition, multiple outcome measures, including 6MWT and HRQOL assessment along with PFT, should be utilized to assess the efficacy of treatment in CF pulmonary exacerbation and to guide clinical decision making. We speculate that the use of multiple outcome measures as end points in clinical trials will afford a more complete picture of the impact of new therapeutics in patients' functional capacities and quality of life.
Footnotes
Acknowledgments
This study was partly supported by a grant from the Webb foundation. The authors would also like to acknowledge Frederick Dorey, PhD, for aid in statistical analysis and the patients and their families for participating in this study.
Authors' Contributions
Rajeev Bhatia: Performed the tests, interpreted and analyzed the data, and wrote the article. Daniel J. Lesser: Performed some tests, and reviewed the article. Marlyn S. Woo: Helped formulating the design of the study, and reviewed the article. Thomas G. Keens: Supervised the study, interpreted and analyzed the data, and reviewed the article.
Author Disclosure Statement
None of the authors have any conflict of interest to declare that is related to this article.