
Abstract
Obesity rates have increased dramatically among children in many parts of the world, especially in North America and several other English-speaking countries. The impact of obesity on pediatric health has become a major prevention initiative by the Obama administration and several public health organizations. Children with obesity are at increased risk for developing asthma, which is already one of the most common chronic diseases among children. The cause underlying obesity's impact on asthma risk is unknown. Commonly cited potential etiologies include airway smooth muscle dysfunction from thoracic restriction, obesity-related circulating inflammation priming the lung, and obesity-related comorbidities mediating asthma symptom development. Each of these theories does not fit precisely with all of the data that have accumulated over the last decade. In this review, I will explore other possible causes including: (1) dietary characteristics common in Westernized countries that might lead to both obesity and asthma; (2) reductions in physical activity; and (3) genetic alterations that increase the propensity to both obesity and asthma together. Next, I will review the current data on how obesity affects common characteristics of asthma such as airway inflammation, lung function, risk of exacerbation, atopy, and response to treatment. Obesity in children with asthma appears to be associated with greater airflow obstruction and a mildly diminished response to inhaled corticosteroids. Little objective evidence in children suggests that obesity significantly heightens the risk of exacerbation or worsens disease stability in children. Lastly, I will discuss the current literature that suggests that obese children with asthma generally should receive the same guidelines-based management as lean children. However, interventions that encourage daily physical activity, weight-loss, normalization of nutrient levels, and monitoring of common obesity-related sequelae should be considered by healthcare providers managing obese children with difficult-to-control asthma.
Introduction
Obesity is now a serious public health problem and has been identified as an area of needed focus in order to improve the nation's health. 2 Obesity is associated with reduced quality of life and excess risk for several chronic diseases. Obesity prevalence is highest among adults. However, the change in obesity prevalence in recent decades has been greatest among children (Fig. 1).3,4 It is also important to note that obesity in children is not a problem limited to North America. Worldwide there are now more than 40 million overweight or obese children below the age of 5.5,6 This fact makes the appreciation for the relationships between obesity, nutrition, and lung disease important for any clinician who cares for children in the fields of allergy, immunology, or pulmonology.

Prevalence of obesity during childhood by age group, United States, 1963–2008. Obesity is defined as body mass index ≥95th percentile for age and gender. Taken from Morbidity and Mortality Weekly Report (MMWR) January 21, 2011 Vol. 60, No. 2.
This article will discuss potential mechanisms that explain the evidence linking obesity with asthma risk in children. I will also discuss how obesity affects the characteristics (or endotype) of asthma in children. While covering the topics of asthma-risk and asthma-endotype, I will draw attention to how specific nutritional factors may contribute. Lastly, I will assess the latest data and discuss management considerations for obese children with difficult to control asthma.
If Obesity Leads to Asthma, What is the Mechanism?
More than 15 longitudinal cohort studies have been conducted in adults7–14 and children.15–21 When lean and obese non-asthmatics are followed prospectively, almost universally obese participants are found to be at higher risk of developing true asthma, confirmed by specialist diagnosis 22 and objective measures of disease. 17 Several theories have been proposed that address the link between obesity and asthma risk.23–25 Theories that involve mediating factors stemming from the obese state include abnormal circulating inflammation and oxidant stress, chest restriction with airway narrowing, and obesity-related comorbidities (Fig. 2). Largely through the work of Shore et al., molecular and physiologic characteristics of the murine model of obese asthma are currently being elucidated.23,26–34 However, assessing lung inflammation and lung responses among obese children remains challenging and limited by current technologies. Studies in children involving bronchodilator responsiveness, bronchoconstricting agonists (e.g., methacholine challenge), and airway inflammatory markers have yet to show the same consistent pattern of hyperresponsiveness that have been demonstrated in mice. Therefore, discussions about the etiology of obesity-related asthma in children remain speculative.
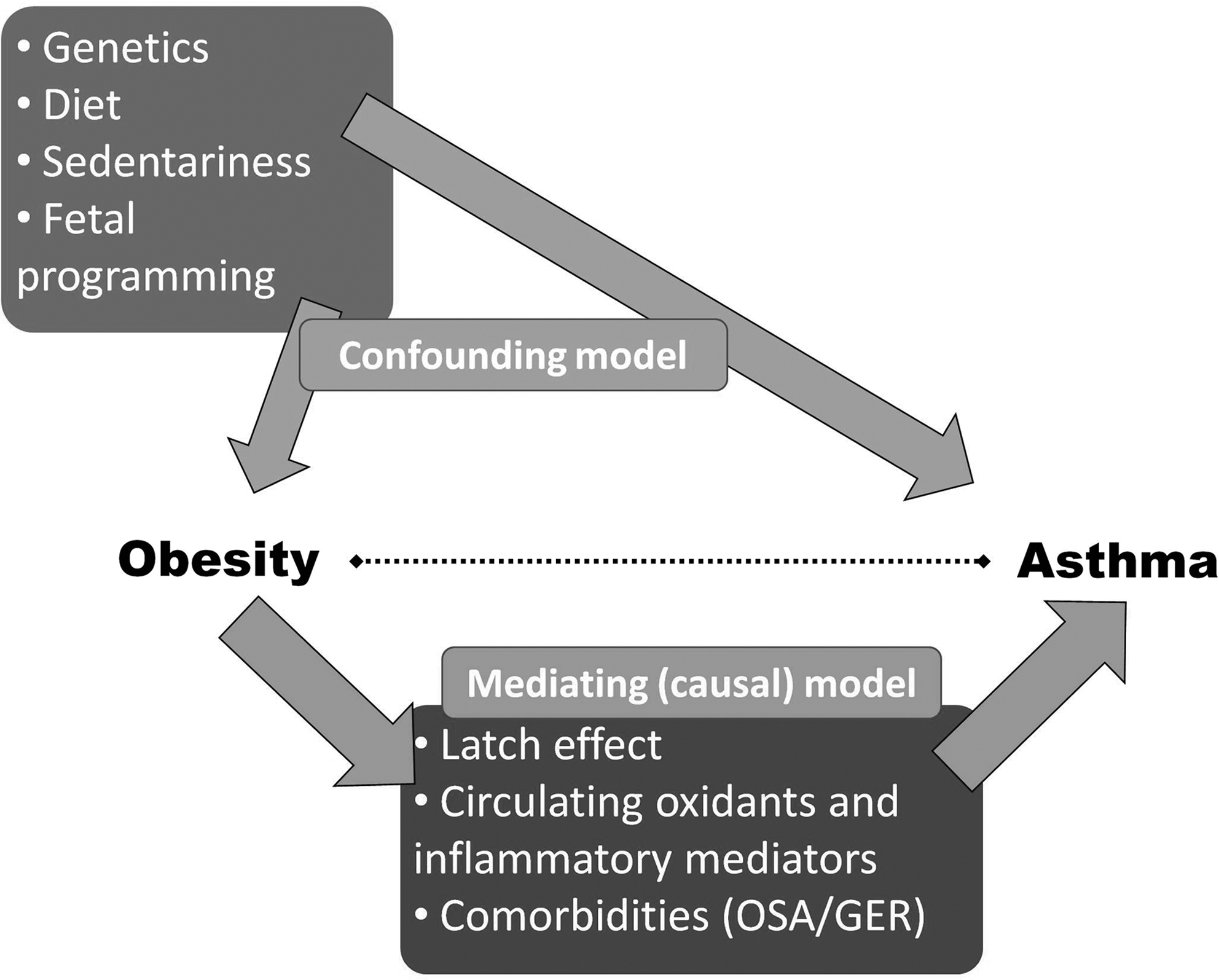
Potential models of association between obesity and asthma. OSA: obstructive sleep apnea; GER: gastroesophageal reflux.
One hypothesis for the obesity–asthma link is that obesity-related systemic inflammation primes the lung for exaggerated responses to environmental triggers, leading to asthma-like symptoms. Adipose tissue releases pro-inflammatory ‘adipokines' (e.g., adiponectin, IL-6, TNFα, leptin) that influence multiple organ systems, including the lung's responses to external stimuli.29,33,35–37 Therefore, obesity-related inflammation may play a role in the development and severity of asthma. 38 However, further work is needed in children.
Some data in adults suggest that obesity may lead to reduced lung volumes39,40 and greater airway responsiveness.41–43 These observations have led to the hypothesis that obesity-related chest wall restriction and the resultant breathing at low lung volume leads to airway obstruction, reactivity, and an asthma-like phenotype. These physiologic characteristics seen in some obese adults appear less commonly in children,44–49 perhaps due to a reduced duration of obesity in children relative to adults. Obesity's effects on airway mechanics and airway reactivity among asthmatic children require more investigation.
Lastly, obesity-related comorbidites such as gastroesophageal reflux and sleep apnea have yet to be conclusively linked to increased asthma risk in children.
A Case for Confounding?
The consistency of the obesity–asthma link suggests that this association is not spurious. However, two other explanations must be considered. These include reverse causality and the presence of a hidden third factor that is associated with obesity and that promotes asthma (e.g., a confounding variable). In the case of obesity and asthma, asthma could occur first and then lead to a higher risk for obesity due to reduced exercise or to frequent corticosteroid therapy. However, to date, there is not convincing evidence that this directionality (asthma causing obesity) is the best explanation, while there is ample evidence that obesity precedes and is a risk-factor for incident asthma.
Another consideration must be the possibility of an extrinsic factor that is closely related to obesity and constitutes the real driver of asthma risk. This factor would be said to be confounding the obesity–asthma relationship. Well-designed cohort studies attempt to anticipate potential confounding variables through statistical adjustment or using a stratified design. However, it can be hard to anticipate, measure, and adjust for all potential confounders. Several factors have been associated with obesity that could plausibly lead to asthma. These include dietary factors, sedentariness, fetal programming, and genetics.
Dietary factors
Diet constitutes an environmental factor that patients are exposed to literally every day, and by way of the maternal diet, it may be a major contributor to asthma development through the mechanism of fetal programming. There is evidence that a Western diet (high in calories, fats, and processed food, and relatively low in fresh fruits, vegetables, and fish) may contribute to both obesity and asthma. Obese children are more apt to have feeding disinhibition, 50 greater fast-food and saturated fat consumption,51,52 and a diet with lower nutritional content. 53 Reduced fruits, vegetables, and fish, and increased saturated fats, burgers, and fast food appear to increase the risk for asthma. 54 Consistent with this, epidemiologic data suggest a relationship between low maternal vitamin E and vitamin D and infant asthma risk.55,56 It is biologically plausible for a high-fat, low-antioxidant diet to lead not only to obesity, but also to an increased risk for asthma. Biochemically, saturated fats may increase activation of the innate immune system and increase circulating mediators such as IL-6, TNFα, and leptin—factors shown to be important in inducing asthma. Within hours of eating a high fat load, NF-kB pathways are induced to create a pro-inflammatory state and excess oxidative stress. Toll-like receptors (TLR), which are known to reside on several types of airway inflammatory cells, serve to activate NF-kB, proinflammatory mediators, and the innate immune system. Importantly, TLR can also be activated by some dietary fatty acids. It should not be surprising that elevated dietary saturated fatty acids have been associated with asthma risk57,58 and asthma severity. 59
Low antioxidant intake and serum levels have been associated with asthma risk and severity. Asthmatics have increased airway and circulating markers of oxidative stress. 60 The antioxidant system, which is equipped to protect the lung from damaging oxidants, is impaired in asthma. 61 Some antioxidants that neutralize reactive species can only be obtained in the diet (including carotenoids, vitamin E, and vitamin C). Children with low dietary intake of vitamins A, C, and E have significantly lower lung function,62,63 suggesting this may be a causative mechanism in obese asthma. These antioxidants are likely to work synergistically, suggesting that a diet consistently rich in fruits and vegetables may be most effective in maintaining lung health.
The effects of a diet high in fat may also depend on the relative composition of fatty acids. The typical Western high-fat diet contains up to 25 times more omega-6 (n-6) polyunsaturated fatty acids (PUFA) than n-3 PUFAs. n-6 PUFAs are found in eggs and most vegetable oils that are now commonly used in cooking, while n-3 PUFAs are contained in cold water fish (such as salmon, tuna, swordfish), mussels, and various seeds. The current 25:1 omega-6:omega-3 fatty acid ratio is much higher than the <2:1 ratio that was typically present during the majority of human evolution.64–66 The Western diet with abundant n-6 PUFA promotes a low leukocyte n-3:n-6 PUFA plasma membrane ratio and appears to increase cellular expression of 5-lipoxygenase pathway products (such as leukotrienes), TNFα, and other molecules important in asthma pathogenesis.67–70 Increases in dietary and inflammatory cell n-3:n-6 PUFA ratio have been associated with improvements in asthma outcomes.71–75 Interestingly, a Mediterranean diet higher in n-3 fatty acids and antioxidants appears to protect young children from recurrent wheezing. 76
Obese children on average consume more n-6 dietary PUFAs, have a reduced n-3:n-6 ratio in their diet, 77 and have reduced n-3:n-6 PUFA serum levels compared to similar leans. 78 A high-fat meal can acutely induce inflammatory airway changes among healthy volunteers. 79 Wood et al. recently showed that a high fat challenge can lead to excess inflammation in the airway and diminished lung function following bronchodilator administration. 80 These observations suggest that a high fat diet consumed chronically may contribute to greater risk of both obesity and asthma.
A patient's vitamin D status also may confound the relationship between obesity status and asthma risk. Vitamin D sufficiency is associated with a healthy diet that is rich in fish and fortified whole grains, and is also associated with sun exposure during outdoor activity. We have found that hypovitaminosis D is highly prevalent in children with poorly controlled asthma, and that serum levels are significantly negatively correlated with BMI (Lang, unpublished). Low 25-hydroxy vitamin D (25(OH)D) levels might increase asthma risk through several biologically plausible mechanisms, including impaired clearance of respiratory pathogens and reduced maturation and functioning of suppressor T-cells and airway smooth muscle cells. 81 Several birth cohorts evaluating 25(OH)D levels in the maternal diet or cord blood have suggested an increased risk in childhood asthma symptoms.82–84 It is possible that low 25(OH)D may be driving some of the asthma risk among obese children. However, further investigation is greatly needed.
Sedentariness
Sedentary behavior is a risk factor for obesity and is a plausible factor leading to asthma.85,86 Children who are overweight sustain less routine physical exertion than their lean counterparts. 87 Repeated exercise promotes hyperventilation, cyclic airway smooth muscle stretch, and bronchodilation. Therefore, exercise and exhaustive play could protect against the development of asthma. Lucas et al. have raised the concern that past cohort studies have not adequately controlled for reduced physical activity and that reduced activity may be promoting asthma risk. 88 Castro-Rodriguez has pointed out that precise measures of exercise and TV watching, plus other potential confounders (e.g. tobacco exposure and family history) may need to be measured more precisely to untangle the relationships among activity level, obesity, and asthma. 89
Shared genetics
It would also be rational to hypothesize that both obesity and asthma stem from common genetic origins.25,90 Our current genetic understanding has stemmed from discovering associations between obesity and asthma phenotypes and candidate gene variants. For example, several promising genomic areas that contain genes connected with both obesity and asthma (5q23-32, 6p21-23, 11q13, and 12q13-24) have been identified.24,25,90–94 Only five genes have polymorphisms that have been associated with both obesity and asthma.95,96 These include β2-adrenergic receptor gene (ADRB2), the TNFα gene, the lymphotoxin-α (LTA) gene, vitamin D receptor (VDR) gene, and protein kinase C-α (PRKCA). Further interrogation of these and other genetic loci is needed among cohorts with and without obesity, and with and without asthma, in order to understand better the nature of the obesity–asthma link.
Obesity and Asthma Endotype in Children
Currently there is not a consensus among clinicians and researchers. does obesity affect asthma disease characteristics in children. I will explore current data on severity, atopy status, oxidation and inflammation in the airway, lung mechanics, and response to rescue and controller asthma therapy in obese and non-obese children.
Asthma severity
There is not currently a consensus about whether obese children with asthma experience greater disease severity. Severity describes the intrinsic intensity of the disease process and includes lifestyle impairment, risk of exacerbation, and level of therapy needed for symptom control. 97 Several reports suggest that asthma is more severe among obese children,38,98–105 while others have found no real difference.106–111 Two large population-based studies have reported greater asthma severity among obese asthmatics based on either patient symptom reporting or physician reporting of diagnostic severity.38,103 Though these results come from excellent epidemiologic studies, they reflect subjective questionnaires or clinician diagnoses rather than objective measures of asthma and thus may be vulnerable to biases. Obese asthmatic children and adults do generally report reduced asthma-related quality of life compared to normal weight asthmatics.98,104,112,113 However, when well-phenotyped pediatric cohorts are examined for an effect of obesity on disease severity using objective measures, very little difference in asthma severity can be found.106,111,114 Recently, we described a cohort of school age children and adolescents with generally mild asthma. 115 The obese adolescents had very similar symptom reporting compared to their non-obese counterparts, while the 6–11-year-old obese asthmatics had improved asthma symptoms compared to leans.
Asthma severity in the urgent care setting has been assessed among obese children in four recent reports.101,102,107,108 Obesity was associated with a significantly higher rate of hospitalization (34% vs. 25%). 102 However, asthma severity using the Modified Pulmonary Index Score was the same in obese versus lean asthmatics. Ginde et al., using a similar index score, also saw no greater asthma severity among obese children in the setting of acute disease. 107 Luder found that obese asthmatics were more likely to be on a greater number of asthma medications, 105 while Vargas did not. 100 We evaluated 10,291 lean and obese children diagnosed with asthma at four Nemours Children's Clinics pediatric asthma clinics over a 10-year period. We found a small but statistically significant increase in odds for severe asthma diagnosis and advanced treatment (EPR-3 treatment step 5 or higher) in obese versus lean children with asthma (Lang, unpublished). However, obese children with asthma seen in our clinic were not more likely to be experiencing an exacerbation. Overall, the data in children do not suggest that obesity leads to a higher risk for severe exacerbation.
The other major domain influencing asthma severity is the level of therapy required to control symptoms. Data suggest that obese asthmatics are at least as hard to control as their lean counterparts, and in some adult reports, are less responsive to conventional therapies.101,102,114,116–120 Evidence suggests that this reduced treatment efficacy may be rooted in true glucocorticosteroid resistance. 116 Recently, Forno et al. showed that obese children may also be less responsive to inhaled corticosteroids. 121 More investigation is needed to evaluate how obesity in children affects response to asthma medications.
Lung function
Obese adult asthmatics generally have similar lung function (or modest reductions in vital capacity) and bronchodilator responsiveness compared to lean asthmatics.114,122 Fewer studies have reported spirometric outcomes in lean and obese children with asthma. Unlike in adults, obesity does not appear to reduce vital capacity or total lung capacity substantially,98,104,106,109 and in some reports may be associated with greater volumes and capacity. 123 However, obese children with asthma may have a mild obstructive impairment in airway flows,22,105,111,115,124 though this has not been a universal finding.98,106,109,125
Airways hyperresponsiveness (AHR) is excessive constriction triggered by innocuous stimuli, and is an important phenotypic component of true asthma. Both AHR and the response to bronchodilator correlate with airway inflammation126–128 and help assess asthma control and future exacerbation risk. Obese children with asthma appear to have similar or even reduced responsiveness to bronchoprovocation compared to lean asthmatic children. 98 Additionally, obese children with asthma appear to have similar or even reduced response to bronchodilators104,111,125 compared to leans. These results provide some evidence that obesity-related risk for new asthma, and possible increases in asthma severity are not due to increases in traditional airway inflammation. Instead, it seems more likely that obesity-related symptoms in children are related to greater airflow obstruction.
Atopy
Though there are some reports of obesity being a risk factor for atopy among adolescent girls,129–131 obesity does not appear to consistently increase the risk for atopy. Both ISAAC and NHANES III data sets have shown no association between obesity and atopy.132,133
Airway inflammation
The measurement of airway inflammation in the obese asthmatic patient is an area in need of further study. Currently there is little evidence that obesity leads to greater allergic airway inflammation in children. Exhaled nitric oxide levels (a surrogate of eosinophilic inflammation) among obese asthmatic children may be the same or even reduced compared to similar leans.134–138 A few studies in adult obese asthmatics have shown reduced eosinophilic inflammation compared with similar leans.112,113 Obese asthmatic children did not have elevated airway LTB4. 134 Recent adult studies suggest that obesity may enhance neutrophilic airway inflammation 139 and systemic leukotriene production, 140 though this has not been evaluated in children. Since inhaled steroids are generally ineffective against neutrophilic inflammation, the discovery of neutrophilic inflammation in obese asthmatics is consistent with findings of reduced corticosteroids efficacy in the obese.
Leukotriene-driven inflammation may play a more prominent role in the obese asthma phenotype. Leukotriene production may be upregulated in patients with obesity.140,141 There is also preliminary evidence that genes, more common among the obese, may affect the leukotriene pathway. We previously determined the allele frequencies of the addition/deletion promoter polymorphism in the ALOX5 gene among a population of lean and obese asthmatics.142,143 The relative risk of obesity in individuals carrying the variant allele was 2.04 compared to carriers of the wild type (p=0.0165; Lang, unpublished). It is rational to hypothesize that obese, non-asthmatic persons may be at enhanced risk for incident asthma due in part to greater upregulation of the leukotriene pathway.142,144 Lastly, data do suggest that relative response to montelukast (a leukotriene receptor antagonist) does increase with increasing BMI. 145 Asthma and obesity are conditions involving excess oxidative stress. Airway 8-isoprostane, a marker of arachidonic acid oxidation, is elevated in obese adult asthmatics. 146 Excess oxidative stress and injury is possibly a second mechanism making the obese–asthma phenotype less responsive to inhaled corticosteroid therapy.
Though the exact nature of the obese–asthma phenotype in children is far from clear, some patterns are emerging (Table 1). In addition, patient factors such as age, age of asthma onset, gender, race, and other factors may modify the effect of obesity on asthma phenotype.
AHR: airway hyperresponsiveness; FENO: fractional exhalation nitric oxide; FVC: forced vital capacity; FEV: forced expiratory volume; LTRA: leukotriene receptor antagonist; GER: gastroesophageal reflux; LDL: low density lipoprotein; † compared to non-obese; NAEPP: National Asthma Education and Prevention Program; GINA: Global Initiative for Asthma.
Weight loss
Both adults and children who are overweight and have asthma are advised by current recommendations to lose weight. Data in adults are encouraging.147–151 However, no studies have been conducted in children determining the impact of weight loss on asthma. Of the adult studies, only a handful has focused on asthma as a primary outcome (Table 2). Most studies had methodological limitations, including small sample sizes and unclear diagnostic criteria for asthma cases. The most commonly noted improvements following weight loss were subjective reporting of asthma symptoms, rescue medication use, and quality of life. 151 It may be important to note that surgical weight loss has yielded improvements in lung volumes and asthma symptoms, but has yet to show consistent improvement in asthma-specific outcomes such as airway reactivity or airflow obstruction. From the studies to date, it is difficult to decipher general improvements in cardiorespiratory health that typically follow weight loss from asthma-specific improvements. Dixon et al. recently reported on 23 adult asthmatics who underwent (primarily Roux-en-Y) weight loss surgery. Following surgery, patients on average had significant weight loss, improved asthma symptom and lung volumes, and reduced airway reactivity. Weight loss did not lead to significant changes in airflow obstruction measured by FEV1/FVC. Surgery-induced weight loss was also associated with increased bronchoalveolar lavage (BAL) lymphocytes and serum and BAL adiponectin. Interestingly, weight loss among asthma patients with elevated IgE did not improve airflow obstruction or airway reactivity, two central characteristics of asthma.
FEF, forced expiratory flow; PF, peak flow.
Fewer studies have been published assessing the effect of weight loss by calorie restriction on asthma outcomes. When obese asthma patients have lost weight with dietary restriction, studies have documented improved objective markers of airway stability and airflow obstruction,149,152 as well as asthma symptoms, rescue medication use, and risk for asthma exacerbation. These data are encouraging and suggest that either reduced calories or changes in particular components of the obese diet may improve asthma outcomes, separate from the beneficial effects of reduced weight. However, further work in this area, especially involving children and involving larger asthma cohorts with well-characterized disease, is greatly needed.
Though the impact of weight loss in obese children with asthma has not been adequately studied, weight loss is an Evidence B recommendation of the Expert Panel 3 Report (EPR-3). 97
Management Considerations
Pharmacotherapeutics
Current research does not support major deviations from current GINA and NHLBI EPR-3 guidelines when considering the management of the obese asthmatic child. However, recent studies may provide important insights for the clinician caring for the obese asthmatic patient. Evidence suggests that obesity may blunt the response to inhaled corticosteroids116,118,145 and low-dose theophylline, 114 and obese patients may respond more favorably (compared to the non-obese) to montelukast. 145 Glucocorticoids inhibit inflammatory gene expression (in part) through activation of MAP-1 phosphatase, which negatively regulates mitogen-activated protein kinase signaling pathways. Therefore, MKP-1 is generally a reasonable marker of steroid signaling and responsiveness. Similar findings of poor steroid response were also seen among airway inflammatory cells. Little is known if the same mechanisms are present in children. A recent report suggests a possible genetic explanation for this pattern of reduced steroid response that may also be coupled with enhanced montelukast response. 153 These findings in conjunction with evidence of superior adherence, 154 suggest that montelukast may be particularly useful in the obese asthmatic population.
Comorbidities
Since the impairment domain of asthma assessment stems from subjective symptoms and quality of life, clinicians should attend to obesity-related sequelae that might interact with asthma symptoms and quality of life. Some obese patients with gastro-esophageal reflux and cough may improve with anti-reflux medications, though empiric treatment for “silent” gastro-esophageal reflux does not seem warranted. 155 Clinicians should maintain a high-index of suspicion for sleep-disordered breathing and metabolic syndrome. Lastly, depression with anxiety is associated with both obesity and asthma, and is commonly overlooked. 156 For these reasons, some children with obese asthma may need more intensive self-management education and help with coaching and adherence. Since mood can affect self-mastery, a home asthma management plan that jointly considers all of the patient's comorbidities may be most effective.
The most universally effective management plan for obese children with persistent asthma continues to involve weight loss, daily exercise, and repeated asthma education about an asthma control plan, inhaler technique, and trigger avoidance. Pharmacologic controller therapy with inhaled corticosteroids and leukotriene modifiers should be first-line therapies. Response variability will likely exist among obese asthmatics, as it does among lean asthmatics. 157 Because of the flat dose–response curve and steroid resistance seen among obese asthmatics, initial step-up therapy for obese asthmatics with poor control should include ICS plus montelukast. However, regardless of the step-up therapy chosen, close patient follow-up is critically important to reassess and reiterate proper inhaler techniques, weight control, low-fat diet, daily exercise, and monitoring of asthma symptoms and medication side-effects.
Dietary interventions
The Centers for Disease Control and Prevention (CDC) and U.S. Department of Agriculture strongly recommend that children adhere to a balanced diet generally low in saturated fats and with half their meal plate consisting of fruits and vegetables. 158 However, many children and families struggle to achieve these recommendations. In addition to supporting our primary care and public health colleagues and reminding asthma patients about these key health initiatives, we as asthma specialists should be aware of the impact diet and weight status may be playing in innate asthma severity and the response to therapy (Table 3).
Modified from the Food and Nutrition Board, The Institute of Medicine, National Academies of Sciences. 1: Daily caloric recommendations are based on age, sex, physical activity, body size, and other factors. The recommendation for the school age child is for an 8-year-old female exercising 30–60 minutes per day. The recommendation for the adolescent is for a 14-year-old female exercising 30–60 minutes per day. More specific recommendations can be accessed through http://www.choosemyplate.gov/. 2: Moderate-to-vigorous physical activity. For toddlers and small children to age the recommendation up to around 120 minutes per day. 3: Primarily salmon, tuna, trout, and swordfish.
There is evidence that suggests that maintaining key antioxidant at normal levels may be helpful in maintaining asthma control. Children with asthma and low antioxidant blood levels appear to have reduced symptom control. When intervention trials have been undertaken supplementing one vitamin alone, the results have been disappointing.159–161 However, intervention with a combination of antioxidants has been more successful.162,163 Similarly, vitamin A, C, and E supplementation together has been shown to ameliorate ozone-induced bronchoconstriction. 164 It is too soon to recommend daily supplementation with antioxidant multivitamins for the treatment of asthma. However, encouraging patients with poor symptom control to commit to a healthier diet replete with the current recommendations for vitamins A, C, E, and selenium may be helpful for asthma control.
Vitamin D
Currently the data are encouraging for the potential future use of vitamin D supplementation as an adjuvant therapy for persistent asthma. Though more investigation is needed, basic research suggests that vitamin D may be important in viral defense,165,166 reduction of virally induced airway inflammation, 167 and response to steroid therapy.168–170 Cross-sectional data in children suggest a significant negative association between 25(OH)D and asthma symptoms,171,172 and a significant positive association between 25(OH)D and both lung function and steroid response. 169 One longitudinal study in children has shown an increased risk for asthma exacerbation among those with vitamin D insufficiency (25(OH)D ≤30 ng/ml). Researchers gave children with persistent asthma either inhaled steroid plus placebo or inhaled steroids plus 500 IU/day of vitamin D3 for 6 months. They found that the D3-treated patients had a significantly reduced rate of asthma exacerbation. 173 However, at this time, the data are not yet strong enough to recommend supplementation beyond the standard daily allowance. However, many children with asthma have low vitamin D. For the many children with difficult-to-control persistent asthma, clinicians should consider hypovitaminosis D as a potential factor. It is for these difficult-to-control patients that adherence to the vitamin D Dietary Reference Intakes (600 IU/day for ages 1–18 years) and serum concentration of 25(OH)D >30 mg/ml (>50 nmol/L) may be most important (Table 4). The best dietary sources of vitamin D are fatty fish, fish liver oil, and fortified foods such as milk, orange juice, yogurt, and breakfast cereal.
Taken from the National Institutes of Health's Dietary Supplement Fact Sheet: Vitamin D, Office of Dietary Supplements (ODS), 2011. IU: International Units; RDA: Recommended Daily Allowance.
Conclusions
Obesity rates have increased dramatically among children in many parts of the world, especially in more Westernized regions. Children with obesity are at increased risk for developing asthma. The cause underlying obesity's impact on asthma risk is unknown and may involve one or more causes. It is likely that interactions between smooth muscle dysfunction and oxidative stress compounded by exercise and genetic and dietary factors are playing major roles. Obesity in children with asthma appears to be associated with greater airflow obstruction and a mildly diminished response to inhaled corticosteroids. Obesity does not appear to worsen risk of exacerbation or objective measures of asthma severity significantly. Obese children with asthma generally should receive the same guidelines-based management as lean children. However, interventions that encourage daily physical activity, weight loss, normalization of nutrient levels, and monitoring of common obesity-related sequelae should be considered by healthcare providers managing obese children with difficult-to-control asthma.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.