
Abstract
Children with empyema are managed differently depending on local practice. There are 2 main approaches: a primary surgical debridement using either a video-assisted thoracoscopic surgical (VATS) approach or an open procedure and primary medical treatment using a chest drain plus intrapleural fibrinolytic drugs. This difference in approach has engendered sufficient passion to produce 2 head-to-head randomized controlled trials (VATS versus fibrinolytics), and neither trial could demonstrate a difference in length of stay or other outcome measure. Other evidence shows that fibrinolytics are successful in between 85% and 95% of cases and that a primary medical management strategy is less costly than surgery.
Introduction
Infection affecting the adjacent lung results in increased permeability of local capillaries, and locally released inflammatory mediators diffuse into the pleural fluid, in turn, activating pleural mesothelial cells. This sets off an inflammatory cascade with activated pleural mesothelial cells, releasing a number of cytokines, including interleukin (IL)-1, IL-6, IL-8, tumor necrosis factor alpha, and platelet-activating factor. As bacteria enter the pleural space, there is activation of the coagulation cascade leading to a procoagulant activity and decreased fibrinolysis, encouraging deposition of fibrin in the pleural space. 1 Thus, infection in the pleural space results in hugely increased fluid production and fibrinous blockage of parietal lymphatic pores (Fig. 1). How should this problem best be managed?
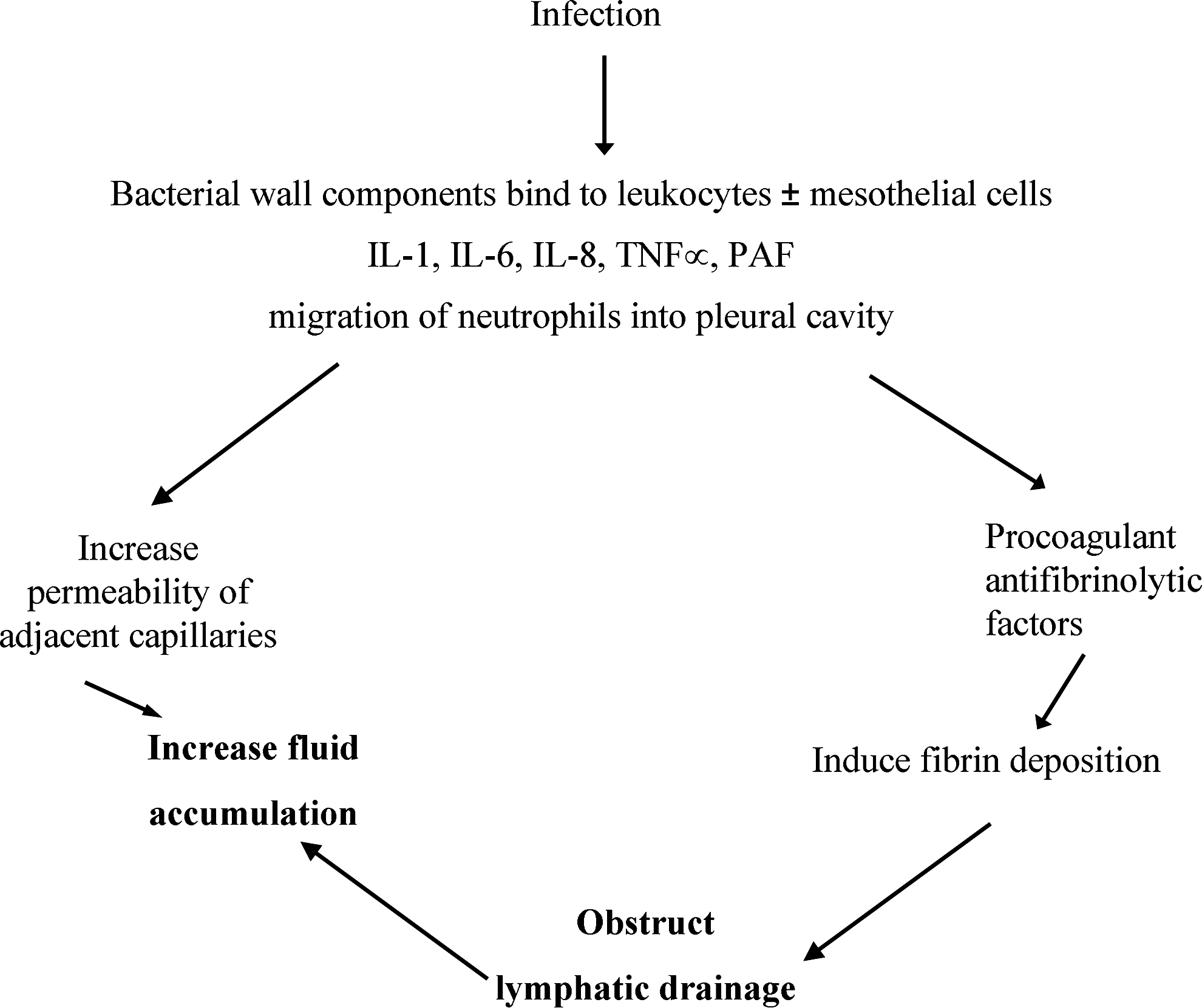
Schemata of cascade in the pleural space leading to empyema.
The aim of empyema management is to treat the infection and thus shut down the inflammatory drivers, restoring the normal pleural circulation, and ultimately restoring the normal lung function. This is achieved with antibiotic therapy, directed to the likely causal organism, either alone or in combination with drainage of the pleural space. Drainage can be achieved by using a simple chest drain, a drain plus fibrinolytic, or by surgical drainage commonly performed as video-assisted thoracoscopic surgical (VATS). This article will present the arguments and evidence supporting chest drain plus intrapleural fibrinolytic for the management of empyema.
Evidence Supporting Fibrinolysis
Intrapleural fibrinolytics have been used in empyema since the 1950s. Initially, naturally derived streptokinase (bacterial derived) was used. This was followed by urokinase (human) and a more recently manufactured tissue plasminogen activator (alteplase). In theory, fibrinolytics disrupt fibrin production, leading to more effective drainage of the pleural space. This occurs both through the pleural drain and by re-establishing effective lymphatic drainage. In rabbit models with tetracycline-induced pleural injury, both proenzyme single-chain urokinase and tissue plasminogen activator reversed loculations at 96 h after injury. 2 In children, fibrinolytics can be instilled and drainage can be achieved through soft small-bore (6–12 FG) chest drains. There have been no formal studies comparing small- and large-bore drains in children.
There have been 2 randomized controlled trials in children comparing intrapleural fibrinolytics to placebo. Thomson et al. 3 compared intrapleural urokinase to intrapleural placebo (normal saline). Fifty-eight patients with empyema aged 6 months to 18 years (median age, 3.3 years) underwent drainage if they had a persistent fever (>38°C) 24 h into treatment with parenteral antibiotics, or if they had a collection causing respiratory distress. Patients were randomized to receive either urokinase, 40,000 units in 40 mL twice daily, or placebo. The primary outcome measure was the length of hospital stay post-intervention. Study results showed a statistically significant shorter length of stay in the treatment group (7.4 days versus 9.5 days; P=0.027). Ninety-three percent (27/29) of children who received urokinase did not need surgery.
Singh et al. 4 compared intrapleural streptokinase (15,000 units/kg/day) to intrapleural placebo (normal saline) in a prospective randomized controlled trial. They included 40 children, aged 1 month to 12 years, with loculated effusions (Light's classification; 5 and above) Stage 5 being a multiloculated effusion, culture or Gram stain positive; stage 6, an empyema with frank pus and a single locule; and stage 7, a complex empyema with multiple locules. The first dose of placebo or streptokinase was given 24 h after drain insertion with 2 further daily doses. There was no significant difference in outcome measures (duration of persistence of symptoms, fever, and respiratory distress; volume and duration of pleural fluid drainage). However, of those with multiple loculations at onset (Light's stage 7), 0/9 in the streptokinase group and 5/7 in the placebo group had residual pleural thickening on ultrasonography examination performed 30 days after diagnosis and required surgery. The length of hospital stay was not used as an outcome measure.
Between 2001 and 2011, there were 28 reported studies3–30 of fibrinolysis in children, including the randomized controlled trials mentioned above. In total, 979 children were treated with an overall success rate (discharge without surgery) of 85.3%.
What Does Surgery Do?
Managing empyema with surgery dates back to Hippocrates (∼500 B.C). Modern-day practice usually entails a debridement procedure to remove pus and fluid from the pleural space. This is most commonly by VATS or with a limited open procedure (mini-thoracotomy). Is the VATS procedure a real advance from the Hippocrates' time? After surgery, the patient will still have a chest drain in situ to drain any further fluid that is likely to accumulate in the pleural space. Some surgeons will also use fibrinolytics postoperatively. Surgery does not contribute to re-establishing the pleural circulation, nor does it spare the need for a chest drain. It is, however, more invasive and always requires a general anesthetic.
Evidence for VATS Versus Fibrinolytics
There have been 2 well-conducted randomized controlled trials in children comparing chest drain plus intrapleural fibrinolytics to thoracoscopic surgery. Sonnappa et al. 5 compared chest drain plus intrapleural urokinase to primary VATS procedure. Sixty children aged 0–16 years with empyema on chest radiograph and ultrasonography were randomized into either a urokinase group or a VATS group. The urokinase group received 12 hourly doses of intrapleural urokinase for 3 days. Failure of treatment was defined as persistent fever after 4 days with persistent fluid on ultrasonography. These patients went on to have secondary VATS. The VATS group underwent primary VATS (or mini-thoracotomy if VATS inappropriate) and had 1 or 2 chest drains left in situ post-operatively. In both groups, drains were removed when drainage fell to 40–60 mL/24 h. There was no difference in length of hospital stay in either group (6 days in each), and failure rates were similar (5/30 in the urokinase group and 4/30 in the VATS group).
St. Peter et al. 6 compared VATS to fibrinolysis. They randomized 36 children, aged up to 18 years, with empyema to VATS or fibrinolysis (alteplase). The VATS group had a drain left in post-procedure. The fibrinolysis group had their first dose of alteplase given at chest-drain insertion and a further 2 doses given 24 hourly. Drains in both groups were removed if <1 mL/kg/day fluid was drained. Results were remarkably similar to the Sonnappa trial. There was no difference in length of stay or in any other outcome measures between the groups. Two patients required ventilator support in the VATS group post-procedure.
In addition to these randomized controlled trials, there have been a number of retrospective reviews. For example, Gates et al. 11 retrospectively compared outcomes of 53 patients treated in 4 different ways (chest drain alone; chest drain plus fibrinolytic; chest drain plus fibrinolytic and surgery; and surgery alone). They found that the length of hospital stay and critical care stay to be shorter and hospital charges to be lower in the nonsurgical groups than in the surgical groups.
Morbidity Associated with Surgery
There is no convincing evidence that the method of primary management of empyema has an effect on critical-care admission rates. St. Peter et al. 6 had 2 patients from the VATS group admitted to intensive care for ventilator support post-procedure. One in each group was admitted to critical care in the study of Kurt et al. 31 Gates et al. 11 showed a longer length of stay in intensive care in patients undergoing surgery than in the nonsurgical group. The size and type of the chest drain left in post-procedure and the adequacy of pain relief are important determinants of post-operative morbidity. There can also be blood loss at debridement that is sufficient to need blood replacement.
Morbidity Associated with Fibrinolytics
When using fibrinolytics versus chest drain alone, there does not seem to be any difference in admissions to critical care. Thomson et al. 3 had 3 patients admitted from each group. Wells and Havens 20 retrospectively investigated the safety and efficacy of urokinase and alteplase in children with parapneumonic effusions or empyema. There were no major complications in patients treated with either agent. Fibrinolytic instillation can cause discomfort, so intrapleural local anesthetic such as Marcaine can be given to combat this. Streptokinase is known to cause more bleeding and chest wall pain than other fibrinolytics. It can also cause a febrile reaction and rarely can result in an anaphylactoid reaction on repeated exposure. 14 Streptokinase is no longer routinely used in the United Kingdom or the United States for the treatment of empyema in children.
Failure Rates
It is important to consider the failure rates of both of these management options. Six percent of patients receiving urokinase required surgical pleural decortication in the study of Thomson et al. 3 Sonnappa et al. 5 had similar failure rates in both groups; 4 patients in the VATS group had to convert to mini-thoracotomy, and 1 had VATS twice. Five patients in the urokinase group went on to have surgery. Sixteen percent of patients in the fibrinolysis group in the study of St. Peter et al. 6 had to undergo secondary VATS. Single-center data 8 with consistent management showed fibrinolytic failure rates, that is, requiring surgery due to the persistence of symptoms and an inadequate response to medical management, of well under 5%.
Long-Term Outcomes
At 3-month follow-up, 92% of patients who received urokinase had a chest radiograph, which was normal or showed minimal pleural thickening. 3 Singh et al. 4 did not have any abnormal chest X-rays at follow-up in those treated with Streptokinase. At 6-month follow-up, Sonnappa et al. 5 had similar results in both groups, with 21/30 in the VATS group and 18/30 in the urokinase group having abnormal chest radiographs. They did not state what they classified as abnormal, and it is likely that they included minimal pleural thickening as abnormal. There is no comparative long-term lung function data reported.
Costs
Where 2 treatments are equally efficacious, costs are of great importance in considering management options. Four studies have specifically considered the costs of treatment.
Sonnappa et al. 5 found the cost in the VATS group to be significantly higher, by 25% (P<0.001). St. Peter et al. 6 also found there to be a significantly higher procedure charge in the VATS group than in the fibrinolytic group. Cohen et al. 32 compared the projected costs and clinical outcomes associated with 5 competing strategies for the management of pediatric empyema. These were antibiotics±chest drain, chest drain without intrapleural fibrinolytics, repeated thoracocentesis, and chest drain with fibrinolytics and VATS. They found chest drain with fibrinolytics to be least costly ($7,787) and VATS to be most expensive ($2,235 more than chest drain plus fibrinolytic). In their retrospective study, Gates et al. 11 again had lower costs in the nonsurgical groups, but total costs were much higher in all groups (Table 1).
VATS, video-assisted thoracoscopic surgical; CXR, chest X-ray; PICU, Paediatric Intensive Care Unit; ICU, Intensive Care Unit; TPA, tissue plasminogen activator.
Conclusions
It is clear that there is a choice in how to manage a child with an empyema. Insertion of a small soft-chest drain under either procedural sedation or general anesthetic, followed by instillation of fibrinolytics through the chest drain, is a safe and effective treatment in up to 95% of cases (Table 2). This management strategy results in a short duration of hospital stay and a normal long-term outcome. The alternative surgical approach is also effective, but is more invasive, always involves general anesthesia, and has significantly higher costs for no reduction in hospital stay or improvement in either short- or long-term morbidity. It is likely that with further understanding of the inflammatory processes involved in the pleural space that the next generation of fibrinolytic drugs will be able to clear the pleural space and re-establish the pleural circulation more rapidly and effectively.
Footnotes
Author Disclosure Statement
No competing financial interests exist.