
Abstract
Congenital tuberculosis is rare in spite of tuberculosis being a common infection worldwide. Due to the nonspecific nature of the presenting signs and symptoms and fatal outcome in absence of early therapy, the importance of early diagnosis is underscored. Young infants with tuberculosis become infected after birth through exposure to family or household members with contagious pulmonary disease. Routes of infection of the fetus before or during birth are dissemination to fetus via the placenta, aspiration of infected amniotic fluid, and direct contact with tuberculous cervicitis or endometritis. We report a case from India of congenital tuberculosis in a 3-month-old male infant who presented with respiratory failure, hepatomegaly, and diffuse infiltrates in the chest radiograph that persisted despite empiric antibacterial therapy. There was no known exposure to tuberculosis by history. Bronchoalveolar lavage culture yielded Mycobacterium tuberculosis. He was successfully treated with quadruple antituberculous medications reinforcing the potential good outcomes with the correct diagnosis.
To our readers:
We are pleased to introduce a new section in this issue entitled, “Clinical Case of the Month”. We wish to encourage our readers to submit interesting and challenging clinical cases that will generate a discussion and/or comments from an expert in the field. For this issue, we are featuring a case of congenital tuberculosis submitted by Dr. Rashmi Kapoor from Regency Hospital Ltd. in India with expert discussion by Dr. Andrea Cruz of the Department of Pediatrics, Section of Infectious Diseases and Emergency Medicine, Baylor College of Medicine. This exemplifies our commitment to publish material that contributes to our knowledge and has clinical relevance from both local and international perspectives.
Introduction
Case Presentation
A 3-and-½-month-old male infant presented to the Pediatric Intensive Care Unit (PICU) in acute hypoxic respiratory failure after a history of upper respiratory tract infection for 10 days. This was our first contact with the patient. He initially presented with fever that persisted and developed dry cough on the fifth day of illness. He remained alert until a day before admission. He had no symptoms of diarrhea, vomiting, ear discharge, skin rashes, or pallor. He was the product of a consanguinous marriage, delivered term to a 26 year-old G2P1 by primary cesarean section secondary to fetal distress but with no postnatal complications. He was small for gestational age with a birth weight of 2.1 kg. His mother's prenatal history was unremarkable. Immunizations were up to date including Bacillus Colmette Guérin (BCG). He lived in an apartment in an urban dwelling with his parents and elder 7-year-old brother. His family history was unremarkable.
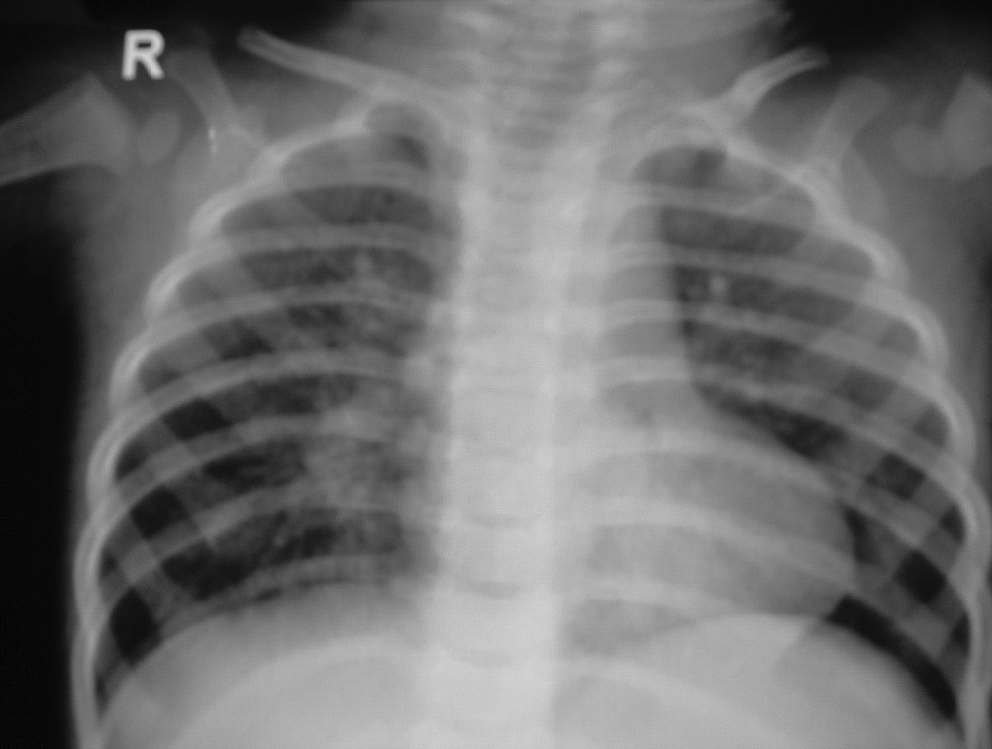
On admission, he was in respiratory distress with a heart rate of 140/min, respiratory rate of 70/min, and his blood pressure was 60 mm systolic. He was febrile with a temperature of 102°F. Sa02 in room air was 80%. His weight was 4.21 kg (3rd%); length, 59 cm (12th%); and head circumference, 40 cm (50th%). Pertinent physical examination findings included chest retractions, diffuse crackles on auscultation, hepatomegaly with liver edge palpated 7 cm below the right midclavicular line, and poor peripheral perfusion. Chest X-ray on admission revealed bilateral extensive alveolar infiltrates (Fig. 1).

Chest X-ray (CXR) showing bilateral extensive infiltrates.
He was admitted to the PICU, intubated, mechanically ventilated for 3 days, and given broad-spectrum antibiotics for 7 days. His general condition improved; however, tachypnea and radiographic findings persisted. Chest computed tomography (CT) scan on day 5 showed multiple necrotic mediastinal lymph nodes with extensive alveolar infiltrates (Figs. 2 and 3). Chest X-ray on day 10 showed generalized miliary shadows (Fig. 4).

Chest computed tomography (CT) scan showing extensive alveolar infiltrates.
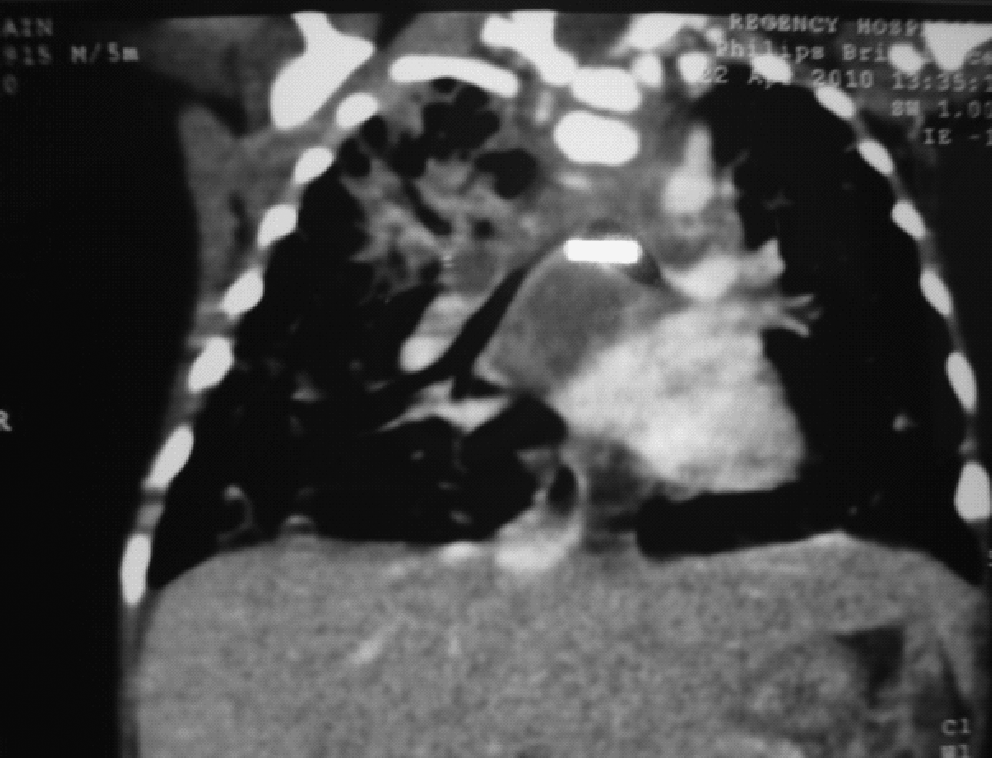
Chest CT scan showing multiple mediastinal lymphadenopathy with central caseation.

CXR at day 10 showing generalized miliary shadows.
The following differential diagnoses were considered:
• Bacterial bronchopneumonia • Tuberculous bronchopneumonia • Cystic fibrosis • Immunodeficiency • Cytomegalovirus (CMV) infection • Pneumocystis carinii pneumonia • Congenital alveolar proteinosis
Results of laboratory tests are summarized in Table 1.
Hb, haemoglobin; Hct, haematocrit; WBC, white blood cells; Diff, differential; CRP, C-reactive protein; BUN, blood urea nitrogen; N, neutrophil; L, lymphocyte; E, eosinophil; M, macrophage.
Sweat chloride was normal at 38 mEq/L. Mantoux test was negative. Immune work-up was normal, and human immunodeficiency virus (HIV) antibody was negative. Bone marrow aspirate exhibited erythroid hyperplasia with biphasic maturation interpreted as a response most likely to nutritional anemia. Ultrasound of the abdomen showed coarse liver architecture with multiple hypoechoic lesions involving liver and spleen. Skeletal survey was normal. Cerebrospinal fluid (CSF) analysis and CT scan of the head were normal, thus ruling out meningeal and central nervous system (CNS) involvement. Bronchoscopy with bronchoalveolar lavage (BAL) was performed on the 10th day. Gross findings included normal airway mucosa and architecture. Cytology of BAL showed many alveolar macrophages along with lymphocytes, occasional polymorphonuclears, and columnar cells. Acid fast Bacilli (AFB) stain was positive. BAL subsequently grew Mycobacterium tuberculosis; bacterial and fungal cultures were negative.
A diagnosis of tuberculous bronchopneumonia was considered, and first line antitubercular treatment was started consisting of isoniazid, rifampicin, pyrazinamide, and ethambutol (HRZE). To identify the source case, immediate family members underwent clinical examination, Manoux test, and chest imaging, the results of which were negative. His mother refused an endometrial biopsy. After 4 months of HRZE, the infant showed good weight gain and resolution of tachypnea. After 9 months of treatment, repeat chest X-ray showed resolution of parenchymal abnormalities (Fig. 5). Repeat ultrasound of liver showed disappearance of the hypoechoic lesions. Medications were discontinued after completing a total of 1 year of treatment with no evidence of any drug-related adverse events during the course of treatment.
CXR after 9 months of therapy showing parenchymal clearing with some hilar lymphadenopathy.
Discussion
Congenital tuberculosis is rare inspite of tuberculosis being a common infection worldwide. Less than 300 cases have been described in literature up to 1989. 1 Subsequently, 58 cases were reviewed by Abughali et al. in 1994, 2 and from 2001 to 2005, 18 more cases have been reported. Only 10 cases have been reported in India. 3
In 1935, Beitzke
4
first suggested diagnostic criteria for distinguishing congenital tuberculosis from postnatally acquired disease. In 1994, in a landmark article, Cantwell et al.
5
suggested the revised criteria requiring documentation of tuberculosis lesions in the infant.
(A) Beitzki criteria
4
(i) Isolation of M. tuberculosis from the infant (ii) Demonstration of the primary complex in the liver (iii) In the absence of primary complex in the liver: (a) Evidence of tuberculosis within days after birth. (b) Absence of contact with a case of tuberculosis after birth. (B) Revised criteria by Cantwell et al.
5
Proven tuberculosis lesions in the infant plus one of the following:
(i) Lesions occurring in the first week of life (ii) A primary hepatic complex (iii) Maternal genital tract or placental tuberculosis (iv) Exclusion of postnatal transmission by thorough investigation of contact
Infection of the fetus can occur via direct spread through the umbilical cord or by direct contact with maternal genital lesions during delivery. 6 In these circumstances, M. tuberculosis has been identified in the amnion, deciduas, and the chorionic villi. 4 Placental involvement does not, however, automatically lead to congenital tuberculosis. During pregnancy, dissemination to the fetus is unusual, especially if the mother is taking effective treatment. More commonly, young infants with tuberculosis become infected after birth through exposure to family or household members with contagious pulmonary disease. Other routes of infection of the fetus before or during birth—aspiration of infected amniotic fluid or from direct contact with tuberculous cervicitis or endometritis–were excluded from the original Bietzke criteria but are included in the modified Cantwell criteria. In the present case, the placenta could not have been examined, as the emergency hospital admission at the age of 3 and a ½ months of age was our first contact with the patient. However, we can infer from his low birth weight and subsequent failure to thrive that he was in a compromised intrauterine environment such as from an undiagnosed maternal genito-urinary TB; thus, the reasonable inference that our patient had congenital TB. Hepatic involvement was confirmed by ultrasonography.
The nonspecific symptoms of congenital tuberculosis often mimic more common neonatal disease such as bacterial sepsis or congenital viral infections. 7 Symptoms may be evident at birth but are usually present at 2–3 weeks of age. Our patient may have had earlier onset of disease as manifested by failure to thrive. The course of tuberculosis in the newborn infant usually leads to dissemination and fatal disease if not treated. The lungs and liver are most frequently involved, usually with a miliary pattern, though widespread disease can involve any organ system. The most common clinical signs and symptoms found in neonates with congenital tuberculosis are described in Table 2. 5
Congenital tuberculosis should be suspected if aggressive broad spectrum antibiotics are ineffective and tests for other congenital infections are negative, particularly if the mother is known to have tuberculosis, more so if recently diagnosed. 5 In our case, a diagnosis of congenital tuberculosis was considered based on symptoms including failure to thrive, persistent respiratory findings despite antibiotic treatment, radiographic pattern consistent with tuberculosis that included mediastinal lymphadenopathy with central caseation, and the isolation of the pathogen, M. tuberculosis from a respiratory culture, in this case from the BAL. The infant presented with hepatomegaly confirmed by ultrasound that represents primary hepatic involvement; liver biopsy, however, was not performed given the rest of the clinical and rradiographic findings supporting tuberculous infection. Virtually all infants have an abnormal chest radiograph, with nearly half showing a miliary pattern. The chest radiograph may be normal immediately after birth, but rapidly progresses with even cavitation being described. If possible, the placenta should be examined and cultured for tubercle bacilli. The tuberculin skin test result is unhelpful, as it is almost always negative initially and can take 1–3 months to become positive.
Perinatal tuberculosis occurs from airborne spread from an infected mother, an adult family carrier, or infectious adult with whom the neonate has had contact including nursing and medical healthcare workers. In this regard, the immediate family members of our patient were evaluated for TB and tested negative. These cases may become more frequent with increasing numbers of both mothers and neonates being infected with HIV, as observed in sub-Saharan Africa. 8 Our patient tested negative for HIV antibody.
Diagnosis rests on clinical suspicion and demonstration of AFB in tissue or fluids, particularly on culture of M. tuberculosis. Early morning gastric washings that are positive for AFB on microscopy should be regarded as indicative of tuberculosis 6 ; gastric aspirates, however, have low yield for AFB. Open lung biopsy has also been used to establish the diagnosis. 9 Testing for tuberculosis in children has traditionally been problematic, as children have lower bacillary loads than adults. Therefore, in children, detection of mycobacterial organisms is difficult using standard microbiologic techniques such as AFB smear, polymerase chain reaction, or culture.
In the present case, an initial first-line treatment was started with HRZE (isoniazid 10 mg/kg, rifampicin 10 mg/kg, pyrazinamide 30 mg/kg, and ethambutal 20 mg/kg) for first 4 months. Then, pyrazinamide and ethambutol were withdrawn, and isoniazid and rifampicin were continued for another 8 months. The American Academy of Pediatrics recommends 9 months of treatment for children with disseminated tuberculosis, and 12 to 18 months for children with tubercular meningitis; the World Health Organization recommendations for disseminated and military tuberculosis is only 6 months. In India, where drug resistance is prevalent along with a high relapse rate, we decided to treat our patient for 12 months. The patient was followed monthly with no adverse events from therapy encountered. Liver enzymes and blood counts remained within normal range.
In conclusion, M. tuberculosis infection can present at any age with a wide spectrum ranging from the absence of symptoms to life-threatening respiratory failure. Congenital tuberculosis is a rare presentation of childhood tuberculosis and on diagnosis, appopriate treatment can result in favorable outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.