
Abstract
The American Academy of Pediatrics recommends the use of an objective means of evaluating the response to a trial of bronchodilator therapy in viral bronchiolitis (VB), but there is an inherent subjectivity with the use of clinical assessments. The goal of this study was to explore the possibility of using respiratory inductive plethysmography (RIP) to serve as an objective measure of change in respiratory function in infants with VB receiving albuterol (ALB) therapy. This was a randomized, double-blind, placebo-controlled study in previously healthy infants hospitalized for VB. Study subjects randomly received either ALB (0.1 mg/kg) or normal saline (NS) by nebulization. RIP data were collected during clinically determined quiet sleep before and after treatment. We enrolled a total of 20 study subjects; 10 received ALB and 10 received NS. Mean tidal breathing measures did not change significantly in either group post-treatment. However, the phase angle fell by >40% of baseline in 3 ALB-treated subjects (30%) and 4 NS (40%)-treated subjects. Using RIP, we observed improvements in the respiratory function in a subset of infants treated with ALB and with NS. It is possible that NS itself has beneficial effects. Our results suggest that RIP can serve as an objective measure of respiratory function in studies of infant VB.
Introduction
Infant pulmonary function tests (PFTs) can serve as an objective measure of respiratory function, and using infant PFTs, investigators have shown that a subset of infants have improved airflow following bronchodilator administration.5,6 These observations indicate that lung function in some infants with VB can improve with bronchodilator therapy. However, infant PFTs require sedation and/or invasive procedures, a high level of technical expertise, and a large amount of time and labor.7–10 These features preclude their use in general clinical practice and limit their use in research. The use of a simple, noninvasive test of infant respiratory function would provide an objective measure of treatment response and greatly enhance the ability to study respiratory diseases in this population.
An alternative approach to assessing respiratory function is by tidal breathing analysis, which can be done either with a pneumotachometer attached to a face mask or respiratory inductive plethysmography (RIP). 11 RIP uses inductance bands placed around the rib cage and abdomen to noninvasively measure their excursion during tidal breathing. 11 Normally, movement of the rib cage and abdominal compartments in infants is very synchronous, but in the setting of obstructive airway disease, such as bronchiolitis, their motion is asynchronous, a phenomenon known as thoracoabdominal synchrony. The phase angle (Φ) is a quantitative measure of thoracoabdominal synchrony. Perfectly synchronous breathing is associated with a Φ of 0°, whereas completely asynchronous breathing (i.e., paradoxical breathing) has a Φ of 180°. Another tidal breathing measure is the ratio of time to peak expiratory flow to total expiratory time (Tpef/Te), which is decreased in the setting of airflow obstruction. 12 RIP can be used to calculate both Φ and Tpef/Te. Numerous studies have reported increased Φ or decreased Tpef/Te in infants and children with a variety of pediatric respiratory diseases, including asthma, cystic fibrosis (CF), and bronchopulmonary dysplasia (BPD).13–19 In some studies, these measures have been shown to correlate with direct measures of lung function, such as lung resistance or spirometry.13,15 However, RIP has not been used as an outcome measure in studies of VB therapy.
The AAP guidelines and the Cochrane review highlight the importance of having objective measures of response to bronchodilator therapy in VB. Infant PFTs have demonstrated the presence of a subset of infants with VB who respond to bronchodilator therapy, but they are an impractical technique for general clinical use. Because it is simple and noninvasive, RIP is an attractive method of assessing infant respiratory function, but it has not been studied in VB. With those facts in mind, our goal was to explore the ability of RIP to serve as an objective measure of change in respiratory function in infants with VB receiving ALB therapy. We hypothesized that RIP would identify a subset of infants with VB whose respiratory function improved after ALB treatment.
Methods
This project took place from 2006 to 2009. Before initiating the study, we obtained approval from our local institutional review board. Study subjects consisted of previously healthy infants ≤12 months of age without chronic lung disease who were hospitalized at Golisano Children's Hospital with the diagnosis of VB. Inclusion criteria for the study were age ≤12 months, full-term birth history (≥37 weeks gestation by dates), hospitalized with a physician diagnosis of VB, and parents who were able to understand the study protocol and provide informed consent. Exclusion criteria were previous history of wheezing or treatment with bronchodilators before current illness, previous treatment with palivizumab or other respiratory syncytial virus (RSV) prophylaxis therapy, history of respiratory infection (e.g., fever, cough, rhinitis) in the 3 weeks before enrollment (other than the current illness), underlying active chronic lung disease (e.g., CF, BPD, congenital lung anomaly), hemodynamically significant congenital heart disease, immunocompromised state, ALB therapy within 6 h of administration of study drug, other conditions that could affect respiratory status (e.g., gastroesophageal reflux requiring medical therapy or neurodevelopmental delay), family unable to provide informed consent or comply with study procedures, and severe VB requiring admission to the Pediatric Intensive Care Unit or inhaled bronchodilator greater than or equal to every 2 h.
After obtaining informed written consent from a parent or legal guardian, we obtained a brief history (including information on family history of asthma and allergy and patient history of atopic disease, such as eczema) and performed a limited physical examination before performing RIP. We obtained information on the etiologic agent causing VB from the clinical laboratory records, which at the time of our study performed viral culture, rapid antigen detection for RSV and influenza only, and no polymerase chain reaction studies. For each infant, we calculated a Respiratory Distress Assessment Index (RDAI) score, a clinical score that has been commonly used in other studies of VB therapy. 20 The RDAI score is calculated by assessing wheezing severity on a 0–8-point scale and retractions on a 0–9-point scale. A higher score is indicative of a more severe disease. Improvement in the RDAI score is based on the Respiratory Assessment Change Score (RACS), which is the difference in the RDAI score before and after treatment. To calculate the RACS, an additional point is subtracted if the respiratory rate decreases 10% from baseline. A decrease of ≥4 points is considered a clinically significant improvement.
We performed RIP using a protocol adapted from a recently completed study that we conducted in preschool children with CF. 17 Briefly, an inductance plethysmography vest system (LifeShirt; VivoMetrics, Ventura, CA) was used. The subject was fitted with an appropriate sized vest and the vest adjusted so the chest inductance band was at the level of the nipples and the abdominal band was at the level of the umbilicus. The fit was snug enough that the bands would move with any thoracic or abdominal motion, but without restricting excursion. Analysis was performed using accompanying software (VivoLogic; VivoMetrics). Infants were continuously observed during the procedure and studied during clinically determined quiet sleep. 21 Data were collected for a minimum of 30 min before administration of ALB. Rib cage and abdominal excursion were internally calibrated against each other using the quantitative diagnostic calibration technique. 22 External calibration of the tidal volume to a fixed known volume was not performed. After collection of baseline RIP and RDAI data, subjects were randomly administered inhaled ALB [0.1 mg/kg in normal saline (NS) for a total volume of 3 mL) or placebo (3 mL 0.9% NS] by a small-volume jet nebulizer. To assess adequate ALB delivery, another observer recorded the heart rate before and after treatment; this information was kept blinded from the investigator team until the time of data analysis. Only those infants with a 10% increase in the baseline heart rate were included in the final data analysis. Post-treatment data collection commenced 10 min after the treatment was initiated, and then continued for at least 15 min.
RIP data were analyzed as previously reported17,18 and based on the protocol of Mayer et al. 23 In brief, 5 epochs of at least 3 consecutive breaths before and after treatment were selected for analysis, and mean RIP values were calculated. To reduce the effect of within subject variability, a total of 30 breaths were used for analysis. 24 Selected breaths demonstrated a stable initial volume baseline, rhythmic motion consistent with tidal breathing, and a smooth tracing when viewed on a Konno-Mead plot (i.e., no “figure of eight” loops). 23 In our previous study in CF preschoolers, we showed that this protocol resulted in an intraclass correlation coefficient of 0.76 for measurement of Φ.17,18
We used change in Φ after ALB as our outcome measure to generate our power and sample size estimates. In a preliminary pilot study, we found that that the mean Φ in infants with VB was 38.1° with a standard deviation (SD)=23.5. Assuming that ALB will lower Φ by 1 SD, then a sample size of 10 infants in each arm of the study would provide 80% power to detect this treatment effect in the ALB-treated infants compared to placebo with an α error of 0.05. Comparisons between the treatment and placebo groups were made using the Mann–Whitney U and Fisher's exact test.
Results
We enrolled a total of 23 study subjects. Three subjects (1 ALB and 2 NS) were excluded because they did not maintain quiet sleep throughout the study procedures or we were unable to obtain acceptable RIP data. Of the remaining study subjects, 10 received ALB and 10 received NS. No significant adverse events were noted in either treatment group. Table 1 shows the clinical features of the 2 groups. Despite the randomized study design, the mean age of the ALB-treated subjects was greater than that of the NS group (20.1 weeks vs. 8.8 weeks, P<0.001). A slightly greater proportion of infants in the placebo group were on supplemental oxygen at the time of testing, but this difference was not significant (P=0.65). The RDAI score did not correlate with Φ (Fig. 1). Similar results were seen when the respiratory rate was compared to Φ (data not shown).

Phase angle versus respiratory distress assessment instrument (RDAI) score.
A total of 23 infants were enrolled, and acceptable RIP data were available for 20. Only mean age was significantly different between the 2 groups (P<0.001).
SD, standard deviation; RIP, respiratory inductive plethysmography.
Table 2 shows the clinical and RIP changes in response to treatment for the ALB and NS groups. There were no significant changes in the mean respiratory rate or oxyhemoglobin saturation in either group. As seen in Table 2, mean RDAI did not change for either group, and no infant had a RACS of >3. Mean Φ was similar in both groups before treatment. In both groups, Φ fell, but the change was not significant (P=0.67 for ALB and 0.41 for NS). However, in 3 ALB-treated subjects (30%) and 4 NS (40%)-treated subjects post-treatment Φ decreased by >40% (>1 SD) compared to pretreatment values. The individual changes in Φ are shown in Fig. 2. Interestingly, one infant (subject no. 7) who was assigned to the ALB group experienced a marked increase in Φ post-treatment, going from a baseline value of 18.3° to 72.1°. There was no association between the ALB response and either family or personal history of atopic disease.
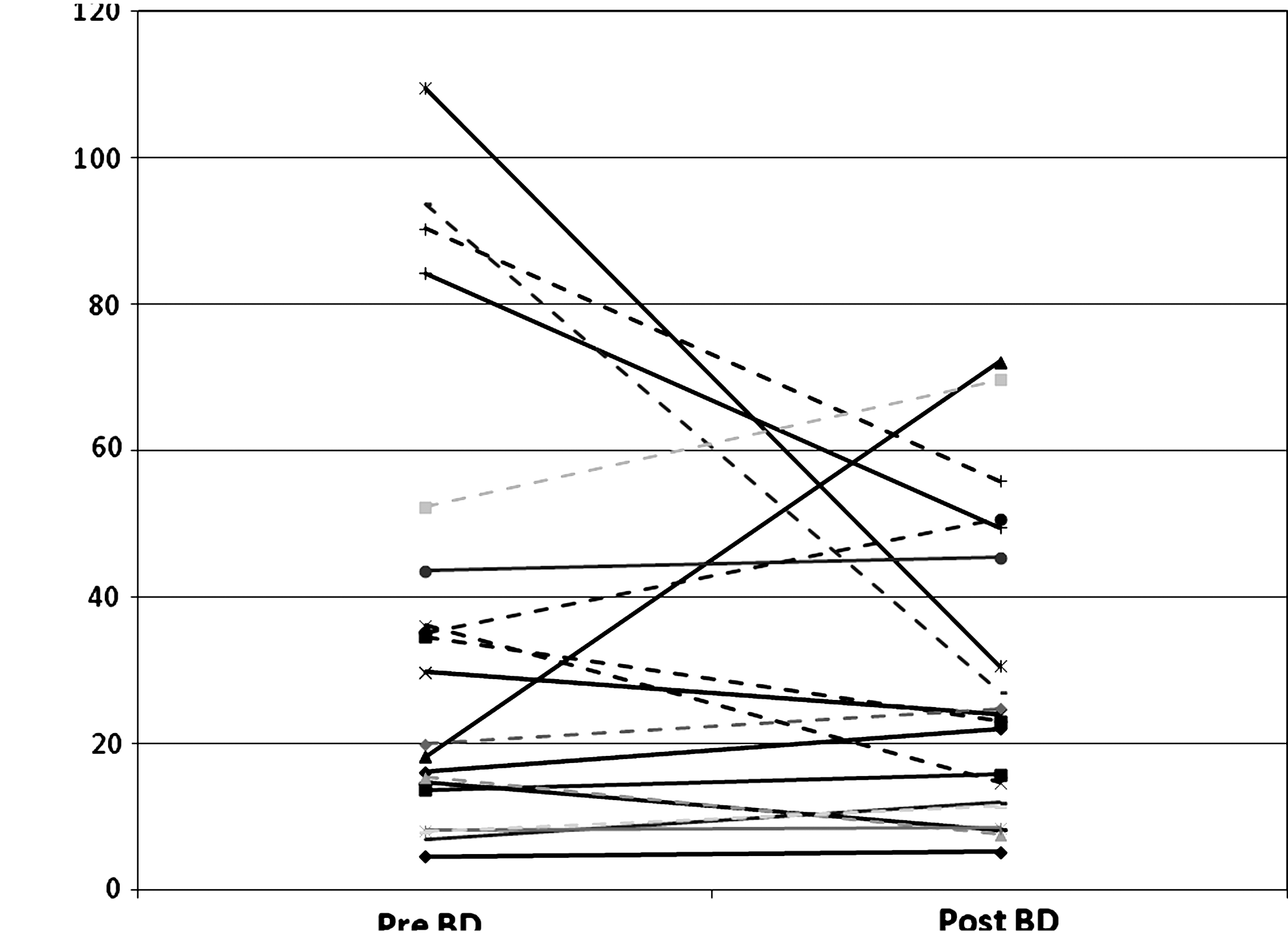
Individual changes in Φ before and after treatment. Subjects who received albuterol are shown in solid lines, while those who received normal saline are shown in broken lines.
RDAI, respiratory distress assessment instrument.
Since a low Tpef/Te has been reported to be associated with airway obstruction,12,15 we also studied the effect of ALB on this measure. Baseline Tpef/Te was similar for both groups (0.47±0.031 in the NS group vs. 0.46±0.26 in the ALB group, P=0.54). It did not change significantly for either group after treatment (NS: 0.48–0.47, P=0.64 and ALB: 0.464–0.465, P=0.98). In contrast to the results seen with Φ, no individual infants had an increase in Tpef/Te after treatment.
Discussion
Studies using clinical scores and infant PFTs have shown that some infants with VB demonstrate an improvement after bronchodilator therapy.4,5,25 The AAP clinical practice guidelines support a trial of bronchodilator therapy in infants with VB, but emphasize the need for careful monitoring with objective measures. 1 To explore the ability of RIP to serve as a simple, noninvasive objective measure of bronchodilator response, we conducted this double-blind, randomized, placebo-controlled study of ALB in infants with VB. We had expected to find a subset of infants whose Φ decreased post-ALB therapy. However, we observed that Φ decreased in some infants in both the ALB and NS groups.
There are several potential explanations for our findings. Studies using infant PFTs have shown a responder subgroup to ALB 5 therapy, but rarely have they included an NS treatment arm. Koumbourlis et al. conducted a study in infants with VB from whom they obtained negative pressure deflation flow–volume curves before and after bronchodilator. 33 They also assessed the effect of inhaled NS in 5 infants. They found a trend toward a lower forced vital capacity and mid-volume expiratory flows, but the changes were not statistically significant. The infants in that study were much sicker than our study population; all of them were on mechanical ventilation and receiving 30%–50% supplementation oxygen. Most all of them had underlying lung disease that may be associated with airway reactivity, such as BPD, whereas our study cohort was composed of normally healthy infants. Taken together, their results and ours suggest that NS probably does not act as a bronchodilator in VB patients. Rather, it may help to mobilize inspissated airway secretions. Infants with underlying chronic lung disease who develop severe VB may have increased bronchial hyperresponsiveness that is worsened by NS.
Although there have been few studies of the effect on NS itself on respiratory function in VB, some information about its effect can be gleaned from other clinical trials in VB, including those using hypertonic saline,26,27 Some studies have suggested that hypertonic saline may be beneficial in the treatment of VB, but in one randomized trial of hypertonic versus NS in the emergency department, the RACS for NS was equal to that of hypertonic saline. 26 Infants in that study had more severe disease compared to our study cohort, which may have accounted for the differences in results. An effect of NS may also account for the high rate of improvement in the placebo arm of randomized trials of bronchodilator therapy in VB. 25 Our results support the hypothesis that NS may have a salutary effect in VB.
Other factors that may have affected our findings include selection bias, subjects' disease severity, sample size, and the sensitivity of RIP in detecting small physiologic changes. We used clinician-diagnosed VB as an inclusion criterion, rather than using a protocol-defined diagnosis. This may have led to some misclassification of infants. For safety reasons, we did not wish to administer placebo to infants who had already been prescribed ALB by the treating physician. This may have removed potential ALB responders from the study cohort that we recruited. Although this was a randomized trial, there was a significant age difference between the ALB and NS treatment groups, perhaps, because of our small sample size. However, infant PFTs studies indicate no difference in bronchodilator response in infants in the age range that we studied. 28 We did not enroll infants in the intensive care unit or very sick infants, so our study cohort had relatively mild disease by the time they received the study medication. Normal reference RIP data for infants in the age range that we studied are not available, but some of our study subjects had baseline Φ within 2 SD of that reported from limited data in normal newborns.13,19 There were more infants in the ALB treatment group with low Φ than in the NS group. Hence, the mild degree of respiratory impairment in our study subjects may have prevented RIP from detecting bronchodilator effects from ALB. We only enrolled a total of 20 infants into the study. However, this met our enrollment target, which was based on our preliminary pilot study and a target treatment effect of 1 SD change in Φ. We did observe a trend in improvement of mean Φ in both the ALB- and NS-treated groups, but the 95% confidence interval for the difference between pre- and post-treatment Φ ranged from −21° to 33°.
RIP does not directly measure physiologic parameters, such as airway resistance, although it has been shown to correlate with these measures. 14 Rather, RIP measures, such as Φ, are dependent upon multiple factors, including neural mechanisms of breathing and muscle strength, not just respiratory mechanics. Thoracoabdominal asynchrony is a normal component of active sleep. Our study protocol called for continuous observation to document the quiet sleep state, and clinically determined quiet sleep has been an accepted method of documenting sleep state in previous studies utilizing infant RIP. Nonetheless, it is possible that infants were in active sleep for part of the RIP study. Because the ultimate goal of our work is to develop noninvasive methods to assess respiratory function, we did not compare RIP to direct measures of lung function obtained with infant PFTs. However, such studies would be helpful in assessing how much RIP is a reflection of an infant's underlying pulmonary physiology.
One infant had an increase in Φ of 53° after receiving ALB. A paradoxical response to bronchodilator in infants with VB has been noted before. 28 Since wall tension of a cylinder is inversely proportional to the radius, 29 bronchodilation can potentially lower wall tension and increase airway compliance, leading to airway collapse and obstruction. The potential for a paradoxical response to a bronchodilator highlights the importance of conducting a carefully monitored trial of bronchodilator therapy in VB, and our results suggest that RIP can provide an objective measure to detect this potentially deleterious effect of ALB.
Our observations underscore the limitations and challenges of using clinical scores as outcome measures in VB.1,30,31 Clinical scores, such as the RDAI incorporate elements, such as the respiratory rate and auscultatory findings, which may be dependent upon factors not directly related to underlying lung disease, such as central control of breathing or expiratory flow efforts. 32 In contrast to clinical scores, RIP has previously been shown to correlate with direct measures of lung function.12–14 In our study, as in previous reports,13,19 RIP measures did not correlate well with clinical measures, such as respiratory rate and RDAI scores.
In summary, using RIP, we observed a decrease in Φ in a subset of ALB-treated infants, and unexpectedly, a subset of NS-treated infants. Although interpretation of our results is limited by the mild degree of respiratory disease present in our study subjects, our study represents the initial steps in developing an objective tool to assess pulmonary physiology in infants with VB. Our findings support the AAP guideline recommendation that ALB should not be used routinely in the treatment of VB, but it is possible that a carefully monitored trial using an objective measure like RIP can identify infants who may benefit from ALB therapy. Future studies should be conducted on the relationship between RIP and infant PFT measures, the feasibility of using RIP in the clinical setting and the relationship between a bronchodilator response noted by RIP and other clinical measures, such as length of stay or need for PICU admission.
Footnotes
Acknowledgments
E.E.S. and S.W. contributed equally to this study. The authors thank Drs. Caroline Hall and Carl D'Angio for their thoughtful review of drafts of this manuscript and their service on Dr. Scarlett's Scholarship Oversight Committee. Portions of this work were supported by grants to C.L.R. from the Strong Children's Research Center and MedImmune, LLC.
Author Disclosure Statement
No competing financial interests exist.