
Abstract
To determine whether a parent survey linked to physician prompts, using a computer decision support system we have designed (the Child Health Improvement through Computer Automation system, or CHICA), affects physician diagnosis of childhood asthma. A randomized controlled trial was conducted in a primary care pediatric clinic for children aged 3 to 11. An asthma module was added to the CHICA system for the intervention group, where parents were asked about asthma symptoms on a prescreener form. If a parent answered yes, then the physician received a prompt to determine whether an asthma diagnosis was appropriate. In the control group, parents received no screening questions, and physicians received no prompt. Over the study period, 2098 patients were randomized. Excluding those children with a previous diagnosis of asthma in the 14 months before the study, significantly more children in the intervention group were diagnosed with asthma than in the control group (8.6% vs. 5.8%, P<0.02). This study showed that the approach utilized by the CHICA system was effective in increasing physician diagnosis of asthma. Computer decision support systems, like our CHICA system, have much potential for increasing asthma case finding through parent questionnaires and tailored physician guidance. (Clinical Trial Registration: Clinicaltrials.gov, ID number: NCT01312805)
Introduction
One approach to improve early diagnosis of asthma is the use of questionnaires with or without assessment of lung function. 5 This population-based asthma detection method has been utilized most often in school settings.5–12 However, they require an additional step of referral, which makes them less likely to succeed. The American Thoracic Society in their 2007 report on asthma screening in children advocated that the primary site of case detection should be the primary care clinician's office. 13 For example, Nichols and colleagues 14 implemented the Health Risk Assessment survey within pediatric outpatient clinics to predict whether a patient is likely to have asthma. However, systems like this are stand-alone products and not part of usual clinical care. Because of this, actual utilization of such systems falls well below 100%. 14
To achieve widespread and consistent use within the real world clinical setting, asthma detection methods need to be seamlessly inserted into the normal workflow of a busy clinical setting. This study sought to determine whether implementation of a parent survey linked to physician prompts using a computer decision support system that we have designed (the Child Health Improvement through Computer Automation [CHICA] system) would increase physician diagnosis of asthma among children.
Methods
The CHICA asthma module
The CHICA system is a decision support and electronic medical record system developed by our research group for use in pediatric primary care clinics and it has been described in previous publications.15–24 The CHICA system uses a paper prescreening form that is tailored to the individual patient in order to collect data from the patient/parent while in the waiting room of the clinic. Once the parent completes the prescreening form, these data are scanned and merged with previously existing data in the electronic medical record and analyzed to generate a second form, known as the provider worksheet. This worksheet includes guideline-based reminders that are tailored to the individual patient.
For this study, an asthma module was added to the CHICA system based on the 2002 Guidelines for the Diagnosis and Management of Asthma published by the National Heart Lung and Blood Institute. 25 The 2002 guidelines were utilized as the start date for this study was July 2005, before the release of the 2007 guidelines.
The asthma module is triggered at patient check-in to the clinic. At that point, the CHICA system reviews diagnostic codes obtained from the electronic medical record to determine whether or not the patient has a previous diagnosis of asthma (i.e., ICD-9 code 493.*). Also at patient check-in, the CHICA system automatically checks to see whether a child has been previously randomized into a study group. If not, CHICA randomizes the child to either the intervention or control group. CHICA then writes the study arm assignment into the electronic record so that it is accessible at future clinic visits.
In the intervention group, if a patient did NOT have a previous asthma diagnosis, then parents were asked about asthma symptoms, including wheezing, coughing, and breathing problems on the prescreening form (Fig. 1). A panel of pediatricians who develop clinic practice policies for our health system developed the wording of this question. The question was designed to be sensitive and not necessarily specific because it was assumed that the physician could make the final determination about the appropriateness of an asthma diagnosis. If the question was answered “Yes,” then the physician would receive a tailored prompt on the physician worksheet helping him or her to diagnose and classify the asthma (Fig. 2). At that time, CHICA also would print out an asthma action plan with criteria that helped the physician distinguish between intermittent and persistent asthma. If the parent answered “No” to the screening question, no asthma prompt was printed for the physician, and the screening question would be asked again after a year.

The Child Health Improvement through Computer Automation (CHICA) PreScreening Form.
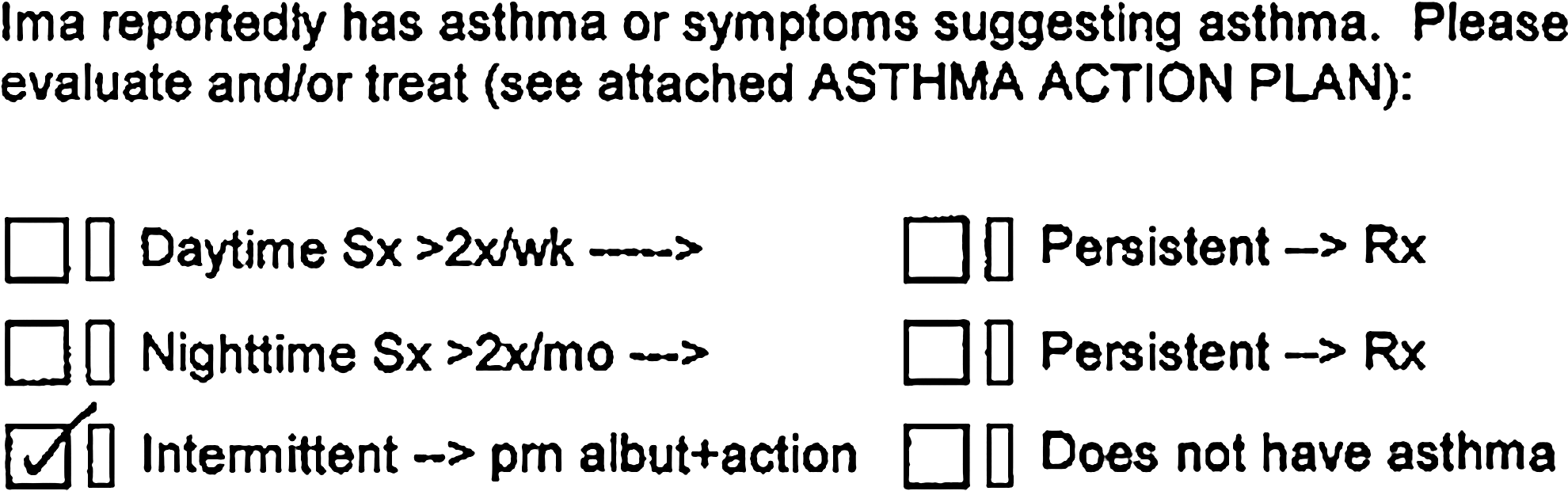
The CHICA Physician Worksheet.
In the control group, parents were NOT asked screening questions about asthma, and the physician received no prompt on the physician worksheet regarding asthma.
Eligibility
All children aged 3 to 11 years seen in our main primary care clinic between July 2005 and April 2007 were eligible for this study and were randomized into an intervention and a control group. The only types of patient visits not included as part of this study were walk-in or urgent care visits.
Data analysis
We hypothesized that the use of the CHICA asthma module would significantly improve the physician diagnosis of asthma in children aged 3–11. To calculate this diagnosis rate, we extracted asthma ICD-9 diagnostic codes from the clinic billing system. The billing system operates independently of the CHICA system so that differences in rates of diagnosis could be attributed to changes in physician diagnostic behavior rather than simple improvements in documentation. We first identified all patients who had a previous ICD-9 diagnosis of asthma in the 14 months before the study. We did this by searching through the claims for all children with ICD-9 codes for asthma (493.*). These patients were excluded from subsequent analyses, as we wished to determine how many newly diagnosed children would result from the CHICA system versus standard care. We did not expand our analysis to look beyond the ICD-9 code of 493.* as our main outcome of interest was specifically rates of detection for asthma as defined by our clinic. We used chi-squared analysis to test this hypothesis. All calculations were performed using the STATA 9.0 statistical package (STATA Corporation, College Station, TX). Informed consent was waived and all methods for this study were approved by the Indiana University School of Medicine Institutional Review Board.
Results
Over the course of this study, 2098 patients were randomized. The control group had 1016 participants, and the intervention group had 1082 participants. Patients enrolled were about equally split between boys and girls, and were mostly Black (47%) and Hispanic (33%). No significant differences in terms of gender or race were found between the two groups after randomization. Because patients who come to clinic more are more likely to be diagnosed with asthma, one data variable we paid particular attention to was the number of return clinic visits that occurred over the course of the study (i.e., between July 2005 and April 2007); the intervention and control groups did not differ significantly in regards to this variable. Summary statistics on the study population are in Table 1.
When data were missing from the medical record, numbers do not add up to N=2098.
Of the 1082 participants in the intervention group, 686 parents (63%) at some time over the course of the study answered the question as to whether their children had “asthma or wheezing, cough or breathing problems that won't go away or keep coming back.” Of those, 164 (24%) answered “Yes” to this question triggering CHICA to prompt the physician to evaluate; the other 76% of the 686 parents answered “No,” denying any asthma symptoms.
Our search of the electronic medical record revealed that the number of children with a previous diagnosis of asthma in the 14 months before the start of the study were 79 (7.8%) in the control group and 72 (6.7%) in the intervention group. This difference was not statistically significant (P=0.33).
Excluding those children with a previous diagnosis of asthma in the 14 months before the start of the study left 937 participants in the control group and 1010 in the intervention group. It is these 1947 children who are included in the main analysis. More children in the intervention group (87) were diagnosed with asthma than in the control group (54) during the study period. This difference (8.6% vs. 5.8%) was statistically significant (P<0.02).
Discussion
This study found that a one-item parent questionnaire linked by computer to a physician prompt resulted in a 2.8% increase (48% relative increase) in the rate of newly recognized asthma by physicians. In this one study clinic alone, this could represent 67 otherwise unrecognized cases of asthma per year. However, due to the limitations of our study design, we are not able to validate the accuracy of the physician's diagnosis. Our study relied on physician judgment to make the diagnosis of asthma—the CHICA system did not instruct them in any way on how to make that diagnosis decision.
There are several other limitations to this study that warrant consideration. It is possible that unmeasured differences existed between those who received the intervention and those who did not, such as the level of asthma symptoms, but randomization at the patient level makes that unlikely as well. Patients who come to clinic more are more likely to be diagnosed with asthma. However, the intervention and control groups did not differ significantly in number of return clinic visits. Diagnosis of asthma is only the first step in the care of asthma patients. It is a necessary one, however, and an important first step.
There are many recommended guidelines and algorithms for health care. Integrating them easily into clinical practice is a challenge. This study demonstrates the outcome of one approach to addressing this challenge. Future studies are needed on use of physician prompts to improve physician adherence to guideline-based recommendations for asthma management.
Footnotes
Author Disclosure Statement
The authors declare no sources of financial support or conflicts of interest.