
Abstract
Laryngotracheal clefts can be a cause of chronic aspiration and cough in children. While there are 4 subtypes, they can be grouped into 2 separate clinical entities. Type 3 and 4 clefts, in which tracheoesophageal communication can extend from the larynx into the trachea and down to the carina, are very rare with early presentation such as dramatic aspiration, bronchial flooding, and respiratory distress. Surgical repair for these anomalies is challenging with a nearly 50% mortality rate. In contrast, type 1 and 2 clefts, which extend to or through the cricoid, can be more difficult to identify. The incidence of type 1 cleft ranges from 0.2% in cadaveric studies to 7.6% in children undergoing direct laryngoscopy for chronic cough or recurrent pneumonia. Patients with type 1 or 2 clefts may go undiagnosed for years with recurrent aspiration, pneumonia, chronic cough, and swallowing difficulties. However, identification and effective management is critical as these patients can go on to develop chronic lung disease from the repeated aspiration events. Careful examination in the operating room with palpation of the interarytenoid region is essential to the diagnosis of type 1 and 2 laryngotracheal clefts. Treatment should include thickened feeds and swallowing therapy. If conservative management fails, endoscopic surgery can also be a minimally invasive way of managing these patients. A high clinical level of suspicion and effective communication between the pulmonologist, gastroenterologist, and otolaryngologist must be maintained to help identify this clinical entity.
Introduction
CN, cranial nerve.
There is no gold standard for the diagnosis of aspiration in children. Several studies are often used together to paint a global picture of swallowing function. Bedside evaluation of swallow, modified barium swallow, flexible endoscopic evaluation of swallow, bronchoalveolar lavage, pH probes, and reflux studies as just a few of the tests that can be ordered. Identification of aspiration can be particularly difficult if it is intermittent. This work up requires a multidisciplinary approach involving pulmonology, otolaryngology, gastroenterology, speech language pathology, occupational therapy, the patient, and his/her family.
The role of the otolaryngologist in this schema is in the evaluation of the larynx and trachea. The larynx acts as the gateway to the trachea and lungs. Via transnasal flexible indirect laryngoscopy, the otolaryngologist can evaluate functional aspects of the pharynx such as vocal fold mobility, glottic incompetence, as well as pharyngeal wall and base of tongue motion. Direct laryngoscopy and rigid bronchoscopy in the operating room are also essential for evaluating the anatomy of the larynx and the trachea.
Embryology
In the ∼20-day-old embryo, the foregut is visible as a recess of the yolk sac and a median pharyngeal groove develops as the first indication of the respiratory system. Starting 1 week later, at 26 days, the respiratory primordial lung bud begins to descend caudally into the mesenchyme ventral to the foregut. 5 This mesenchymal tissue between the respiratory of digestive tubes comprises the tracheoesophageal septum. 6 As this respiratory diverticulum continues to elongate, the median stalk gives rise to the trachea. The separation point remains at a constant somatic-vertebral level, while the tracheal bifurcation descends. 6 The cricoid ring condensation begins laterally at 41 days and proceeds ventrally and dorsally. Formation of the cricoid is complete by 48 days. The embryonic periods ends at 57 days (8 weeks). 5
Pathophysiology
Without an animal model, the pathophysiology of tracheoesophageal anomalies has not been well understood. Merei and Hutson developed an adriamycin rat model to study these rare disorders; however, none of their embryos had evidence of laryngotracheal cleft. 7 However, they theorized that if no upper foregut pouch develops, then the ventral half of the foregut differentiates into the trachea and the dorsal half into esophagus with a communication between, that is the cleft. 7
Historical Perspectives
The first reported case of laryngotracheal cleft was in 1792 when, using his finger to examine the throat, Richter described a newborn in whom the “gullet and the larynx were seen to be a common cavity.” 8 While there were other reported cases of clefts diagnosed postmortem,9,10 it was not until 1955 that Pettersson reported the first successful repair of a cleft, that extended through the cricoid to the lower margin of the thyroid gland. 11 Atkins 12 and Vervat 13 each published case reports of unsuccessful attempted repairs in 1962. Ten years after the first successful repair, Blumberg published the first review of the literature in 1965. He reviewed 13 published cases, with only one surviving case, which was Pettersson's. 8 The second successful repair was published as a case report by Shapiro in 1966. 14 Roth published the first series of 3 surgically repaired cases in 1983. 15 Since the 1980's, the advent of endoscopic laryngotracheal management techniques has dramatically increased the identification and management of this clinical entity.
Epidemiology
The reported incidence of laryngotracheal cleft varies widely throughout the literature. Two studies have examined autopsy specimens. Cameron and Williams published a series of 2000 pediatric autopsies in 1962 and reported 4 cases of cleft (0.2%). 16 In 1997, Moungthong and Holinger performed postmortem exams of 115 infant larynges and identified 11 clefts (9.6%). 17 The difference between the 2 studies may be due to differing definitions of laryngotracheal cleft. Moungthong and Holinger identified 8 (7%) submucous clefts in which there is a defect in the posterior midline cricoid cartilage with intact overlying soft tissue. 17 These were note defined as a clinical entity on the laryngotracheal cleft spectrum until 1987.
In their 1997 paper, Moungthong and Holinger also reviewed 2338 direct laryngoscopies performed at their institution and identified 7 clefts (0.3%). 17 This is more in line with the autopsy data from Cameron and Williams; however, they did not report the indications for the direct laryngoscopies. One year later, in 1998, Parsons reviewed 660 patients who underwent direct laryngoscopy and identified 41 type I laryngotracheal clefts (6.2%). 18 The indications for surgery in Parsons' article were symptoms and signs related to laryngotracheal incompetence such as microaspiration (or macroaspiration), wheezing, recurrent lower respiratory tract infections, chronic cough, or feeding difficulties. 18 More recently, Watters and Russell (2003) reviewed 168 patients who underwent direct laryngoscopy and noted 12 patients with type 1 laryngotracheal cleft (7.1%). 19 In 2006, Chien and Hartnick et al. reviewed 264 patients who underwent direct laryngoscopy for cough or chronic aspiration and noted 20 cases of type I cleft (7.6%). 20 The variance between Moungthong's data versus Parsons, Watters, and Chien may be related to referrals to a tertiary referral center or the pretest selection in the indications for direct laryngoscopy. There is a higher incidence noted in children with chronic cough or aspiration as opposed to all-comers for direct laryngoscopy.
Classification
The most commonly used classification schema was described by Benjamin and Inglis in 1989. 21 This is the classification system that will be used throughout this review with the addition of the submucosal laryngotracheal cleft, which was initially described by Tucker and Maddalozzo in 1987. 22 Classification aids in communication between clinicians about these relatively rare disorders. In addition, it can help in planning of the medical and surgical management.
Submucous cleft: a defect in the posterior midline cricoid cartilage with intact overlying soft tissue. Some consider this a subtype of a type 2 cleft.
Type 1: supraglottic interarytenoid cleft, which is located above the vocal-fold level. Type 2: cleft extends below the vocal folds into the upper cricoid cartilage. Type 3: cleft extends through the cricoid cartilage and possibly into the cervical trachea. Type 4: cleft extends into the thoracic trachea and extends variably toward the carina.
Clinically, children with submucous, type 1 and 2 clefts present and behave very differently from type 3 and 4 clefts.
Clinical Presentation
The clinical presentation varies with the type of cleft. Due to the extensive communication between the trachea and esophagus, type 3 and 4 clefts are usually identified in the newborn period. They can have severe aspiration, bronchial flooding (Fig. 1), and respiratory distress requiring intubation. 17
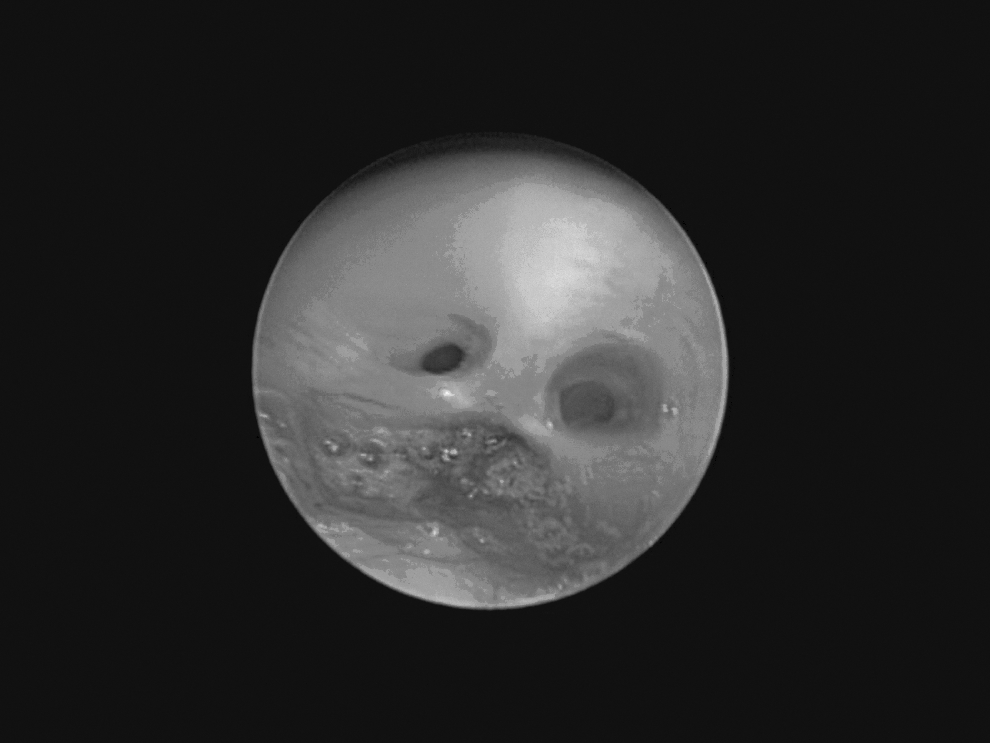
A newborn with a type 4 laryngotracheal cleft. The mainstem bronchi can be seen anteriorly (superior on the photo) with reflux of gastric secretions from the esophagus posteriorly.
In type 1 clefts, the presentation can be more insidious with failure to thrive, wheezing or asthma-like symptoms, chronic cough, or recurrent pneumonia (Table 2). Glossop, in 1984, described 10 cases of laryngotracheal clefts, 4 of which were described as above the vocal-fold level (type 1) and concluded that these smaller clefts were largely asymptomatic. 23 In contrast, Evans reported that all 10 of his patients with type 1 cleft presented with stridor in infancy. 24 Due the subtlety of the symptoms, Parsons, in his 1998 review of 41 type 1 cleft patients, found an average delay in diagnosis of 2 years and 10 months. 18 These patients often present first to pulmonology as opposed to otolaryngology. Rahbar et al. found that 60% of their 28 patients with type 1 cleft and 35% of 21 patients with type 2 cleft were treated with inhaled steroids initally. 25 There are many more studies looking at the clinical presentation of type 1 laryngotracheal cleft in comparison to type 2 (Table 2). There are many fewer reported cases of type 2 clefts compared to type 1with an incidence that may be more similar to type 3 and 4 clefts.
Associated Anomalies
Evans, in 1995, reported up to 50% associated anomalies. 26 In 2006, Chien reported 5%–8% have associated tracheoesophageal fistula. 20 Other associated anomalies include tracheomalacia, cleft lip/palate, anomalous right subclavian artery, pyloric atresia, imperforate anus, pancreatic ectopia, congenital heart defect, and congenital subglottic stenosis. Two syndromes, which are associated with laryngotracheal cleft include Pallister-Hall and Opitz-Frias (G syndrome). 27 Laryngotracheal cleft can also be associated with VACTERL (Vertebral anomalies, Anal atresia, Cardiac anomalies, Tracheoesophageal fistula, Ear anomalies, Renal anomalies, and Limb anomalies) association and CHARGE (Coloboma, Heart disease, choanal Atresia, growth and mental Retardation, Genital anomalies, and Ear anomalies).28,29
Diagnosis
Radiographic tests for the work up of chronic cough or recurrent pneumonia include chest x-ray (CXR) and computed tomography (CT). Williams et al. reviewed 67 laryngotracheal cleft patients and found that in 69% of patients, CT improved the evaluation of the distribution and extent of lung disease over CXR. Findings included consolidation (56%), reticular opacities (44%), and lung parenchymal abnormalities in the upper (12.5%) or lower (87.5%) lung zones. 30
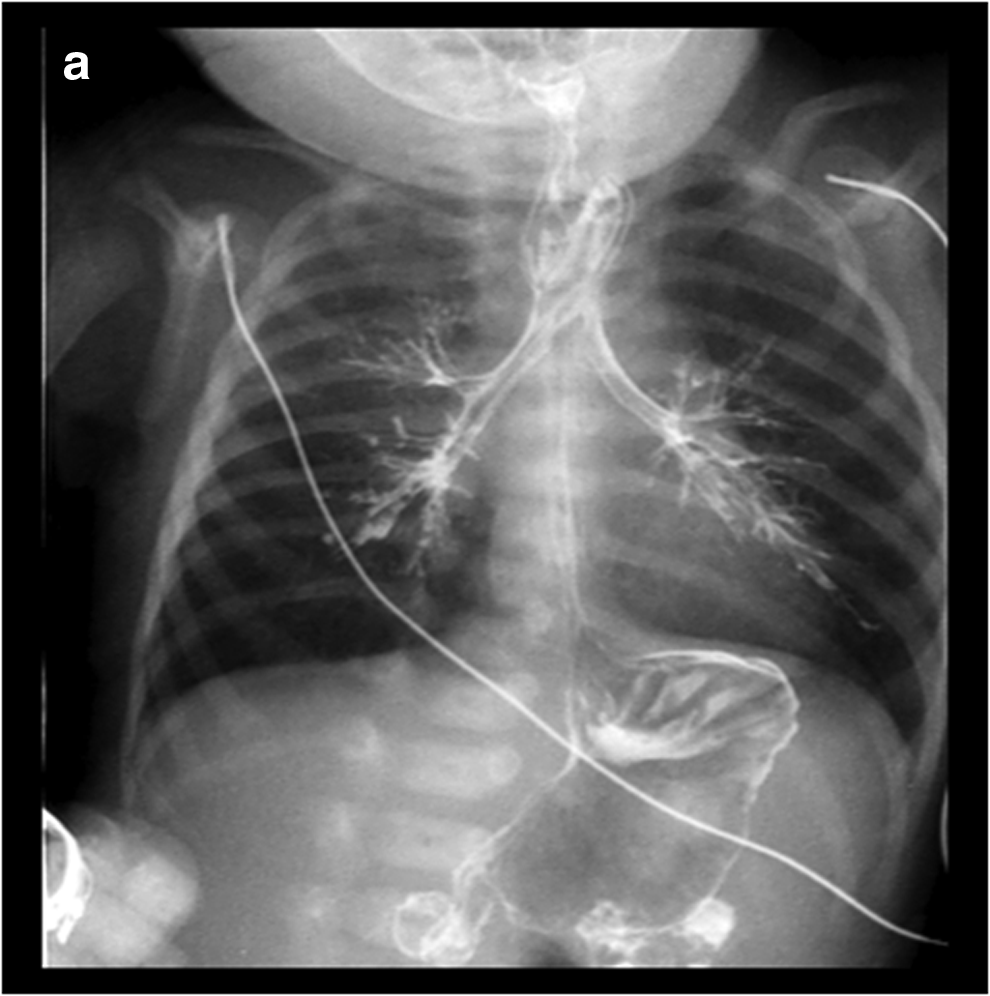
In the evaluation of a patient for possible aspiration, modified barium swallow performed in conjunction with speech language pathology is a valuable diagnostic tool. While the anomalous connection between the trachea and the esophagus can be suggested on barium swallow (Fig. 2), the diagnostic technique of choice is direct examination of the larynx and the trachea in the operating room. It is easy, however, to overlook the diagnosis of laryngotracheal cleft if the surgeon is not careful to look and palpate the posterior glottis. Heaped-up tissue may be noted in the posterior glottis (Fig. 3). In 1977, Pillsbury and Fischer developed a measuring gauge to determine the length of clefts. 31 That same year, Bell described using a laryngeal spatula to palpate the posterior glottis. 32 Holinger used laryngeal forceps to spread apart the larynx for closer examination of the interarytenoid region in 1985. 33 In their 1989 article, Benjamin and Inglis described the use of an anterior commissure laryngoscope to separate the posterior glottis. 21 In 1990, when microlaryngoscopy was becoming increasingly prevalent at more institutions, Eriksen et al. advocated its use in the identification of laryngotracheal clefts. 34 This can also combine with bimanual palpation of the posterior glottis.
Type 1 cleft can be the most difficult to identify. In 1998, Parsons described a technique using a 90° probe placed between the arytenoid processes. 18 This probe is then rotated side to side with in the larynx. In the normal larynx, the tip of the probe touches the false vocal fold. In the type 1 cleft, the tip may be at the level of the ventricle or true vocal fold (Fig. 4). This technique allows for assessment of arytenoid mobility with lateral palpation as well assessment for absence or atrophy of the interarytenoid muscle. Even with this technique it can be hard to identify subtle clefts. It is also important to ensure that the tip of the right angle probe is not allowed to angle forward into the larynx and cause potential over identification. 18

Using a right angle probe to evaluate a type 2 laryngotracheal cleft.
Management
Medical
Type 1 clefts can often be managed medically with antireflux therapy, thickened feeds, and positioning during feeds. Parsons' 1998 article reported that all 41 of his patients improved with medical management. 18 Chien et al., in 2006, reported that 4 of 20 (20%) type 1 laryngotracheal cleft patients improved with conservative therapy. 20 This was judged as improved cough and resolution of aspiration. Watters and Russell, in 2003, found that 2 of the 12 patients (25%) diagnosed with type 1 laryngotracheal cleft improved with conservative therapy. 19
Endoscopic surgery
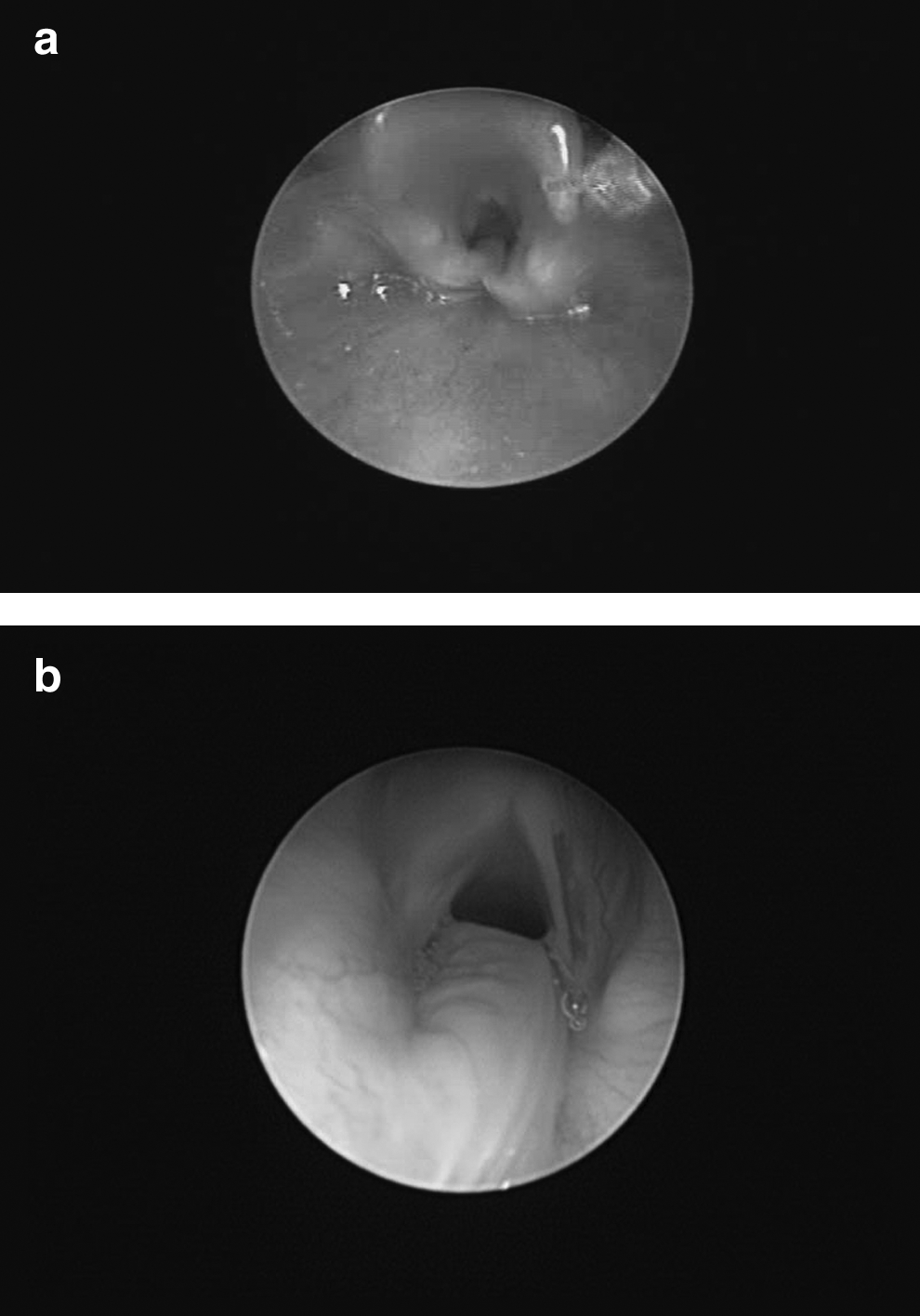
For type 1, 2, and small type 3 clefts, endoscopic repair has been advocated with reported success rates between 80% and 100%.19,20,26,35–38 This approach is performed transorally using a binocular microscope via an operating laryngoscope that is placed in suspension. Ideally it is performed under spontaneous ventilation without an endotracheal tube. The medial surfaces of the cleft are demucosalized using cold instruments or laser. The raw surfaces are then reapproximated to eliminate the aberrant communication between the larynx/trachea and esophagus (Fig. 5). Other reported endoscopic approaches include the injection of various materials, including collagen or gelfoam into the cleft.39–42 Some surgeons have advocated the use of a temporary injection to determine the clinical significance of a small cleft. 40 The advantage of an endoscopic approach as that it is minimally invasive with a shorter recovery time. However, it is technically more challenging for both the surgeon and the anesthesiologist.

Type 2 laryngotracheal cleft after endoscopic repair.
Open surgery
An open approach is required to access the distal portion of the cleft. This is particularly true for type 3 and 4 clefts. The approach can be lateral, which can risk injury to the recurrent laryngeal and pharyngeal nerves injuries, or an anterior translaryngotracheal approach via a laryngofissure (dividing the thyroid cartilage and anterior commissure of the vocal folds). 43 Concerns have been raised regarding postoperative laryngeal stability and altered laryngeal growth after laryngofissure. Froehlich et al. felt in their 1993 report of 2 children that the larynx can exhibit normal growth after laryngofissure. 44
For type 3 or 4 clefts, which extend into the chest, an open approach must be combined with a thoracotomy or sternotomy.26,45,46 In 1983, Roth et al. reviewed 14 patients with type 4 clefts and noted a 93% mortality rate. 15 More recent reviews place the mortality rate at 50%–55%.27,47–49 A critical component to the management of these patients is the management of the gastrointestinal system via G-tube, Nissen fundoplication, or even gastric exclusion. Intraoperative airway management can be very challenging requiring bifurcated tubes, tracheotomy, cardiopulmonary bypass, 50 or extra corporal membrane oxygenation. 51 Postoperatively, tracheomalacia can pose a problem, in up to 2 thirds of patients.47,49 This can be managed with custom bifurcated tracheotomy tubes to stent the airways,48,49,52 excision of the malacic segment, 53 aortopexy,48,54 or positive pressure ventilation.52,55
For all types of clefts combined, the percentage of revision surgeries ranges from 11.2% 56 to 50%. 36
Discussion
Clinically, laryngotracheal clefts should be considered as 2 separate entities. Type 3 and 4 cleft are very rare with early presentation with dramatic aspiration, bronchial flooding, and respiratory distress. Surgical repair for these anomalies is challenging with a nearly 50% mortality rate.
In contrast, type 1 and 2 cleft can have subtle clinical findings. These patients pose a more difficult diagnostic problem. They may go undiagnosed for years with recurrent aspiration, pneumonia, chronic cough, and swallowing difficulties. However, diagnosis and effective management is critical as these patients can go on to develop chronic lung disease from the repeated aspiration events. Modified barium swallow and flexible endoscopic evaluation of swallow, while helpful if diagnostic of aspiration, are nonspecific and can be negative in cases of intermittent aspiration. Not only are the symptoms relatively ambiguous, but the laryngotracheal cleft itself may be difficult to visualize endoscopically. Many surgeons do not regularly palpate for a cleft and it is an entity that can be easily missed. The surgeon must be careful not to apply too much force to the interarytenoid tissue, because this may lead to a false-positive result. Binocular microscopy (versus rigid endoscopy) can be useful, because it allows for depth perception when examining the area. Regardless of the endoscopic technique, it can be hard to distinguish a normal variant from a type 1 cleft.
Once a cleft has been identified, the controversy remains regarding medical versus surgical management. While thickening feeds and swallow therapy can help many patients manage gross aspiration, there is no gold standard for the measurement of intermittent aspiration or microaspiration. In addition, many of patients with laryngotracheal clefts have other associated anomalies that can affect their swallowing function. These co-morbidities can make predicting surgical outcomes more challenging. It can also affect the decision process for or against surgery.
Conclusion
Patients with chronic lung aspiration, especially if it is intermittent, can pose a diagnostic challenge to the medical team. Laryngotracheal clefts are relatively rare; however, if found, a cleft can be a treatable cause of aspiration. Especially for small clefts, the otolaryngologist must be diligent to closely examine the interarytenoid region in the operating room. A high clinical level of suspicion and communication between the pulmonologist, gastroenterologist, and otolaryngologist must be maintained to help identify this clinical entity.
Footnotes
Author Disclosure Statement
There are no personal or financial disclosures or conflict of interest.