
Abstract

Introduction
Case Presentation
A 3-year-5-month-old female toddler was transferred to our emergency department (ED) from a nearby hospital with the complaint of new-onset hemoptysis. The patient had a fever, cough, fatigue, decreased appetite and activity, nasal congestion, rhinorrhea, and diarrhea for 3 days prior to presentation at the ED. Of note is that her brother had upper respiratory infection (URI) symptoms as well. Two days prior, she had one episode of coughing that produced a small-sized red “chunk.” On the day of admission, she had expectorated approximately 3 ounces of blood. This patient had been previously treated at our institution for neuroendocrine cell hyperplasia of infancy (NEHI). She was delivered at 36 6/7 weeks vaginally with a 2-week confinement at the Neonatal Intensive Care Unit (NICU) for respiratory distress, requiring mechanical ventilation for 4 days. She was diagnosed with chronic lung disease with bronchiectasis, tracheomalacia, and gastroesophageal reflux disease (GERD). She also had a history of pneumonia and asthma. She had intermittently received home oxygen such that when her parents noted that her oxygen saturation had dropped from her baseline of 94–97% on room air to 88%, supplemental oxygen was provided at 1/2 LPM via nasal cannula. Her home medications included levalbuterol, montelukast, and fluticasone oral inhalation. Her past surgical history consisted of left lower lung biopsy, Nissen fundoplication, and gastrostomy tube placement 3 years ago. She had no known allergies; immunizations were up to date. Her family history was unremarkable. The patient had no history of travel outside of the country, but had contact with a preschool teacher who recently returned from South Korea and a family friend who recently returned from the Philippines, neither of whom were sick. She had no contact with institutionalized individuals or the homeless.
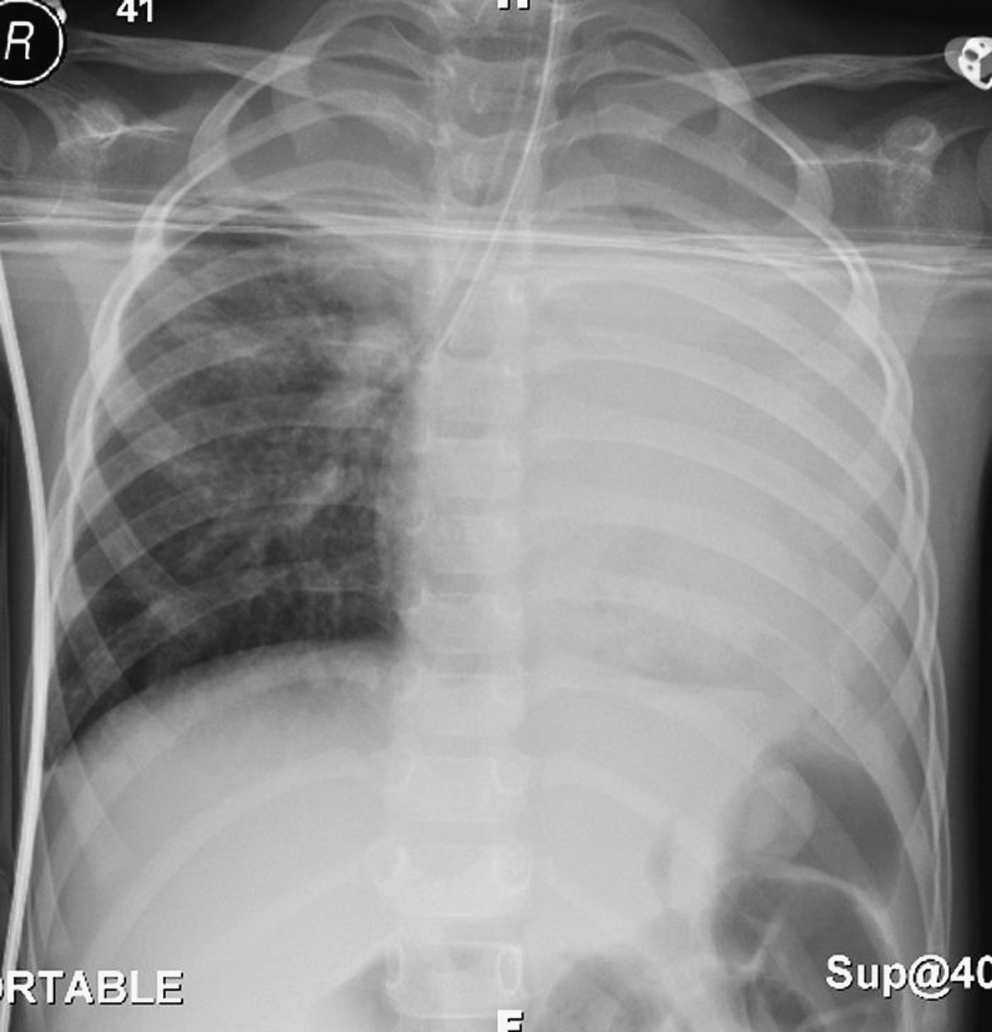
On presentation, she was in no distress. She was playful and interactive. Vital signs were oral temperature 38°C, heart rate 133 beats per minute, blood pressure 82/46 mm Hg, respiratory rate 52 breaths per minute, SpO2 on room air 96%, and weight of 14.2 kg (50th percentile). Her exam was notable for rhinorrhea, decreased air movement in the left lung fields with no wheezes or crackles auscultated; the rest of the exam findings were unremarkable. Initial laboratory tests revealed a white blood cell count of 13.4 cu mm, hemoglobin 6.7 g/dL, platelets 507k, normal comprehensive metabolic panel, and normal urinalysis except for a high specific gravity of >1.030. The chest x-ray revealed extensive left lower lobe infiltrate with involvement of the left upper lobe, as well as diffuse bronchial wall abnormality and bronchiectasis (Fig. 1).

Antero-posterior and lateral chest radiographs show an extensive opacity in the left lower lobe and partial involvement of the left upper lobe. There is marked bronchial wall thickening, most prominent in the left lower lobe. Pleural spaces and the right lung are clear.
Repeat laboratory testing after a fluid bolus revealed persistently low hemoglobin of 5.3 g/dL, normal coagulation studies, ESR 89 mm/h, and CRP 14 mg/dL. Pediatric pulmonary and gastroenterology consults were requested. The patient was scheduled for flexible bronchoscopy and upper endoscopy to determine the source of bleeding. In addition, considering her severe anemia without associated signs of significant cardiovascular compromise, the Hematology Service was consulted. Acute hemorrhage was deemed to have occurred in the setting of a more chronic state of anemia; thus rapid high-volume transfusions could result in cardiac compromise. Transfusion of 5 mL/kg of packed red blood cells was done, which increased the hemoglobin to 7.5 g/dL.
Given the persistently low hemoglobin, cross-matched red blood cells were made immediately available. Prior to the scheduled procedures, the pediatric anesthesiologist, pulmonologist, and gastroenterologist reviewed the plan of action to be taken in the event of significant hemorrhage, which included the type of airway device and its internal diameter, and the manner and ease of lung isolation. Endotracheal intubation with a micro-cuffed tube was preferred to placement of a laryngeal mask airway to secure the airway. The plan was to advance this cuffed tube into the unaffected mainstem bronchus should hemorrhage occur during the procedure. Selective placement of a bronchial blocker was considered. The differential diagnoses remained quite extensive at this time, but primarily included three sources of bleeding: upper airway, gastrointestinal, and pulmonary. The potential diagnosis included acute pneumonia, pulmonary hypertension, or bleeding from the known interstitial lung disease or from a gastrointestinal source given previous surgeries.
Rapid sequence intubation was facilitated by profopol and rocuronium. The patient was easily intubated with a cuffed, 4.5-mm inner diameter endotracheal tube. There was no blood appreciated on direct laryngoscopy. Anesthesia was maintained with propofol and remifentanil. A 20-guage peripheral IV was placed in the left saphenous vein to provide additional access should rapid transfusion be needed. Bronchoscopy with bronchoalveolar lavage (BAL) and endoscopy proceeded uneventfully. There was evidence of thin old blood in the left lower lobe bronchi, but no discreet source of bleeding could be identified.
Upon reversal of neuromuscular blockade and return of spontaneous ventilation, the patient began to have significant hemorrhage that backed up through the endotracheal tube and into the anesthesia circuit. At this time, the blood pressure remained stable but the heart rate increased up to 150 beats per minute. The endotracheal tube cuff was immediately deflated and advanced into the right mainstem bronchus; the cuff was re-inflated to protect the right lung from any hemorrhage. Anesthesia was re-induced and the patient was emergently transfused with 10 cc/kg of cross-matched packed red blood cells. The patient remained stable and well oxygenated during one-lung ventilation. Endotracheal tube positioning was confirmed clinically, by direct visualization with the bronchoscope and radiographically (Fig. 2). Pediatric surgery, interventional radiology (IR), and the pediatric intensive care unit (PICU) were notified. While the patient was being transfused, an arterial line was started. The initial arterial blood gas (ABG) revealed a respiratory acidosis with pH 7.17, paCO2 56 torr, paO2 132 torr, and HCO3 20; hemoglobin was 7.1. The patient was transferred to the PICU on one-lung ventilation and sedated in anticipation of potential additional procedures by IR.
Antero-posterior chest radiograph shows the endotracheal tube (ETT) into the right mainstem bronchus with partial right upper lobe collapse, left lung atelectasis, and minor shift of the mediastinum to the left.
The patient's vital signs on arrival to the PICU included a blood pressure of 74/40 mm Hg and heart rate of 134 beats per minute. Blood gases throughout the night continued to show a respiratory acidosis with pCO2 in the 50s to mid-60s. After almost 12 hours of one-lung ventilation, she continued to exhibit respiratory acidosis with pH 7.11 and paCO2 83 torr. The pulmonologist and the intensivist decided that a gradual withdrawal of the endotracheal tube into the trachea under direct visualization by flexible bronchoscopy was the best course of action. The tube was successfully repositioned without any signs of further bleeding. Blood gases improved and the patient was successfully extubated later in the day.
The BAL cultures including viral panels and antigen assays were negative. The patient continued to do well and completed 7 days of antibiotics in the hospital for community-acquired pneumonia and was transitioned to oral antibiotics for an additional 2 weeks. While the source of bleeding was not definitely identified, the conclusion was that the patient most likely acquired a necrotizing pneumonia in the lobes previously affected by interstitial lung disease as an infant. She was noted to have an upper respiratory infection shortly after discharge and received an additional course of azithromycin given her recent history. She required neither additional transfusions nor hospital readmissions.
Discussion
Pediatric pulmonary hemorrhage is a rare but serious illness. Due to its relatively infrequent occurrence, physicians encountering this condition may have limited or no experience at all. Thus it is important that all specialists involved in the care of these patients review their roles in management of the worst possible scenarios or outcomes.
During fiberoptic bronchoscopy, the pulmonologist and anesthesiologist are working together in a confined space necessitating continuous communication to optimize patient outcome. Hemoptysis is a serious concern and significantly drives the decision to secure the airway with an endotracheal tube during endoscopy or bronchoscopy rather than proceed with a laryngeal mask airway or any level of conscious sedation. Furthermore, the largest possible tube that can be accommodated should be used to facilitate bronchoscopy and continued air exchange while allowing mainstem intubation if necessary. If mainstem intubation is needed, the microcuff will protect the intubated bronchus, thus preventing the spread of blood to the lung facilitating all gas exchange. Even in patients with bilateral lung disease, the choice may remain the same because frank hemorrhage may develop more severely in one lung than the other.
Communication with the primary service facilitated prompt arrangement for packed red blood cells to be made available for emergent transfusion. A large-bore intravenous line was placed in a low-resistance venous system attached to a primed warming system to allow speedy transfusion. The patient was rapidly stabilized during the acute hemorrhage in the operating room, as all participants in the procedures had reviewed and prepared for this complication. Continuing and ongoing communication between the pulmonologist, anesthesiologist, intensivist, surgeon, and interventional radiologist ensured an eventually satisfactory outcome.
Footnotes
Author Disclosure Statement
No competing financial interests exist.