
Abstract
Ivacaftor is a small-molecule potentiator of the cystic fibrosis (CF) transmembrane-conductance regulator and was recently approved for use in CF patients with at least one copy of the G551D mutation. Two clinical trials have proven its efficacy in CF patients 6 years of age and older with mild-to-moderate lung disease. In this article, we report the efficacy of ivacaftor in a 12-year-old CF patient with very severe lung disease and clinical features of cepacia syndrome.
Introduction
Case
A 12-year-old Caucasian boy with CF, whose mutation analysis revealed one copy each of the delta F508 and G551D mutations, initially presented to our center at age 7 years with bronchiectasis, pancreatic insufficiency, chronic malnutrition (BMI 16.1), and colonization with mucoid Pseudomonas aeruginosa and Burkholderia vietnamiensis (Genomovar V). He subsequently developed glucose intolerance that necessitated subcutaneous insulin during intermittent illnesses. His long-term management included pancreatic enzyme-replacement therapy, enteral nutritional supplements, airway clearance using high-frequency chest wall oscillation, inhaled dornase alfa, and hypertonic saline. He received regular alternating 28-day cycles of tobramycin inhalation solution and aztreonam lysine for inhalation. He typically required intravenous (IV) antibiotics every 2–3 months.
He presented with increased cough and mucous production, weight loss of 2 Kg, and fever to 40°C (Fig. 1). He was hypoxemic with room air oxygen saturation of 90% and had an acute decline in forced expiratory volume in 1 second (FEV1) to 37% predicted (Fig. 2). He was then admitted to our hospital. He had leukocytosis with left shift (WBC 25.34×103/UL with 88.5% neutrophils and 57.1% segs). Sputum culture grew clindamycin-resistant, methicillin-susceptible Staphylococcus aureus. Additionally, 2 strains of B. vietnamiensis were identified by pyrosequencing. One strain of B. vietnamiensis was resistant to all tested antibiotics, while the other demonstrated intermediate susceptibility to ceftazidime, minocycline, and meropenem. The presence of these organisms and his clinical status met criteria for the diagnosis of cepacia syndrome. During his 3-month hospitalization, he was treated with multiple combinations of antibiotics, including nafcillin, minocycline, ceftazidime, colistin, trimethoprim-sulfamethoxazole, and chloramphenicol. Subsequent cultures grew Klebsiella pneumoniae in addition to his usual organisms, for which he received cefotaxime. The patient's condition continued to deteriorate with worsening hypoxemia, a decline in FEV1 to 21% predicted progressive weight loss, and persistent spiking fevers to 40.2°C despite aggressive antibiotic therapies, airway clearance, and enteral and parenteral nutritional support. His hospital course was further complicated by a human Rhinovirus infection and by 2 episodes of moderate hemoptysis of ∼60 mL each. Chest computed tomography demonstrated new bilateral patchy consolidations with worsening diffuse bronchiectasis and volume loss (Fig. 3).
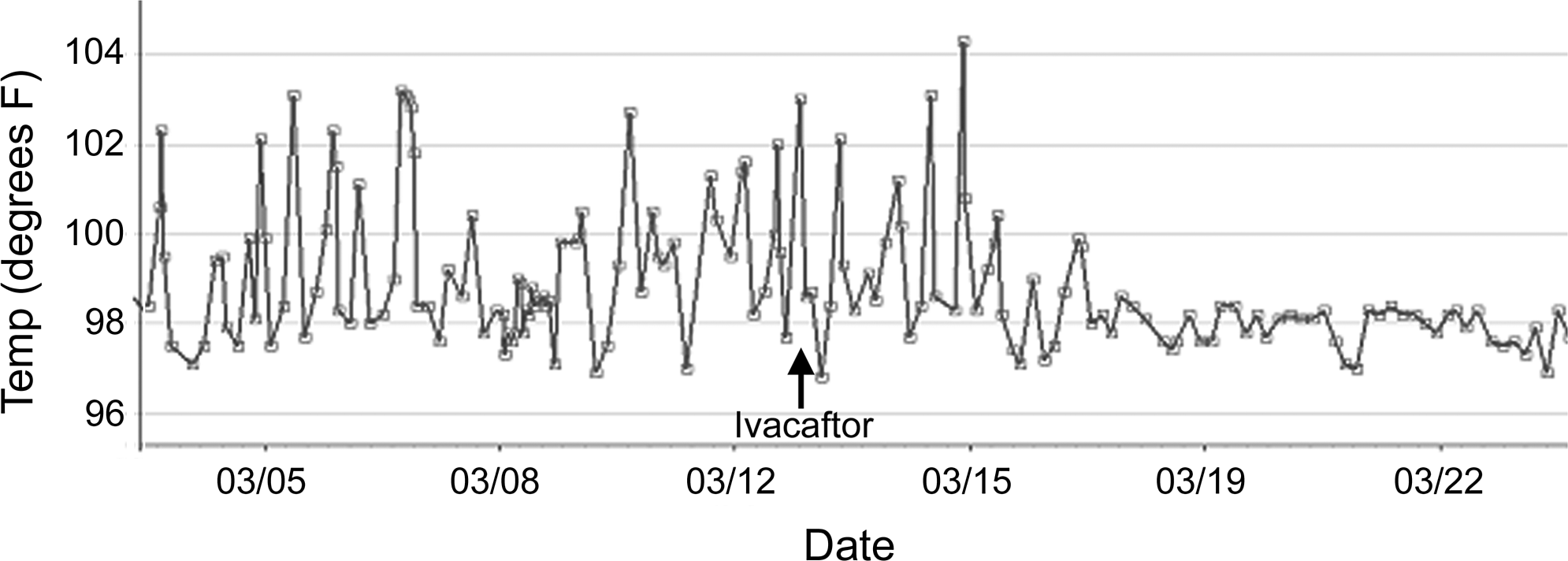
Fever curve for the 10 days before and after starting ivacaftor. The arrow indicates the start of ivacaftor.

Percent-predicted FVC (▪) and percent-predicted FEV1 (▴). The asterisks denote the first spirometry during this admission, and the arrow indicates when ivacaftor was started. FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second.
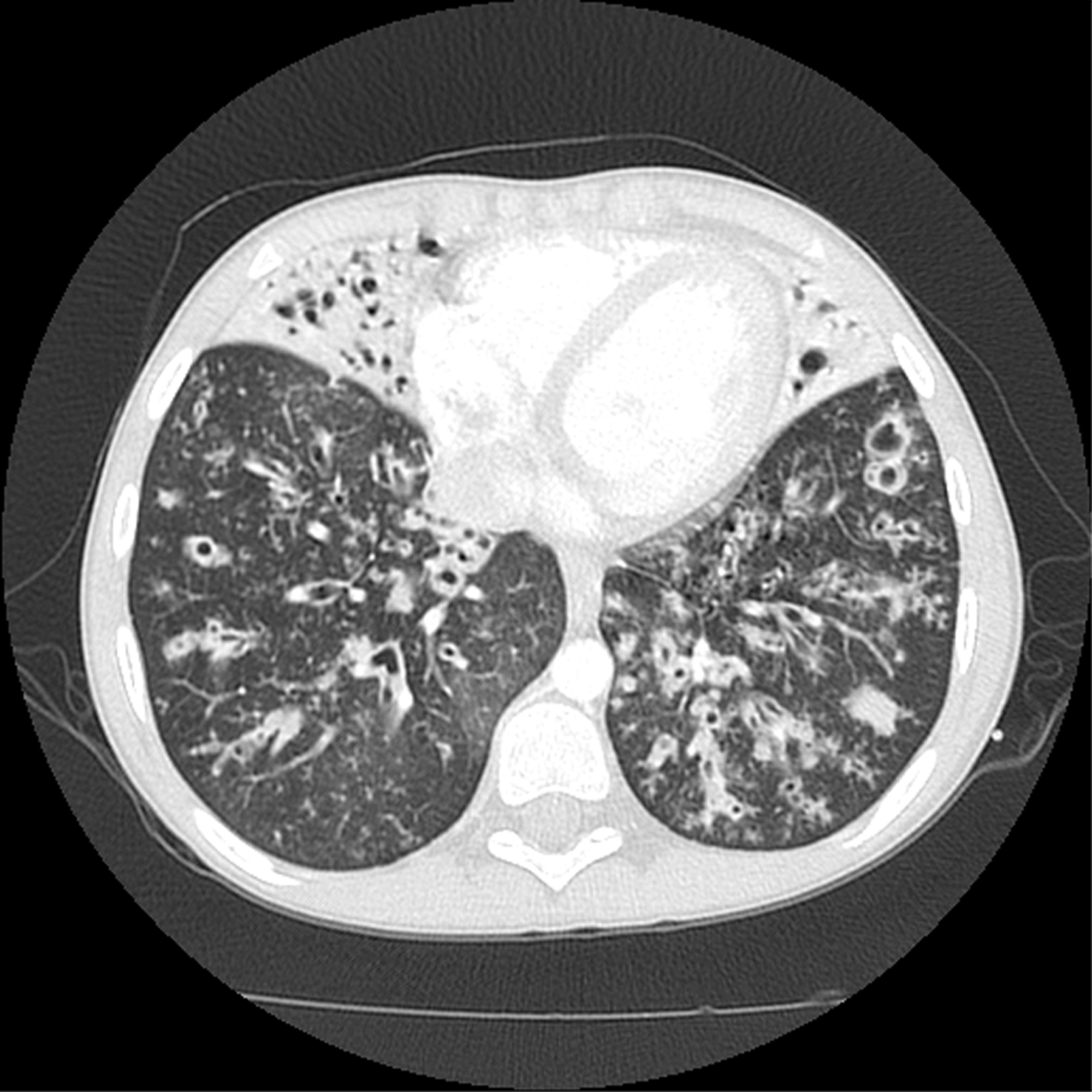
Chest CT scan taken before initiation of ivacaftor showing diffuse bronchiectasis with intraluminal mucus, bronchial wall thickening, and volume loss with consolidation in the right middle lobe and lingual. There also are small centrilobular nodules (tree-in-bud and rosettes) representing mucus plugging. CT, computed tomography.
On day 50 of his hospitalization, his respiratory status further deteriorated with severe hypoxemia and elevated pCO2 to 64 mmHg. Supplemental oxygen therapy via high-flow nasal cannula (HFNC) at 25 L/min with FiO2 of 0.65–1.0 was commenced. Due to his persistent fevers, he was not considered a candidate for lung transplantation, and end-of-life discussions were held with the family. At this time, however, the drug ivacaftor (previously known as VX-770) was approved by the Food and Drug Administration and became available through commercial pharmacies. After discussion with his family, ivacaftor was initiated at a dose of 150 mg twice daily on day 55 of hospitalization. His antibiotic regimen at the time consisted of IV minocycline and trimethoprim-sulfamethoxazole, and inhaled tobramycin. Within 48 h of initiating therapy with ivacaftor, his appetite began to improve, and the volume of expectorated sputum increased. After a transitory worsening in his oxygen requirement, his oxygenation improved allowing progressive weaning of the HFNC flow rate and FiO2. By 72 h, his fever had resolved. Leukocytosis and neutrophilia resolved by day 6 of ivacaftor, and C-reactive protein decreased from 4.4 to 0.5 mg/L. His steatorrhea resolved on day 7, and by day 9, his weight had increased from 26 to 26.9 kg. On day 17, he was transitioned from HFNC to oxygen via simple face mask. Spirometry performed on day 22 showed improvement of forced vital capacity (FVC) to 45.8% predicted and FEV1 to 26.5% predicted having declined to as low as 21% predicted during this hospitalization. On day 26, a 6-min walk test at a moderate pace demonstrated oxygen saturation between 90%–95% while on oxygen via nasal cannula at 2 liters per minute (LPM). On day 29, spirometric measurements had improved to an FVC of 48.6% predicted and an FEV1 of 31% predicted. On day 34 of ivacaftor, he was discharged from the hospital on supplemental oxygen by nasal cannula at 1.5 LPM, and oral trimethoprim-sulfamethoxazole and minocycline.
Within 2 weeks of discharge, his parents reported that he was back to his usual, baseline physical activities, including swimming, with only intermittent episodes of hypoxemia. After 10 weeks of ivacaftor therapy, he was weaned completely off oxygen. His FVC had improved to 58% predicted and FEV1 to 38% predicted. The absolute value of FEV1 had improved from 320 mL before starting ivacaftor to 590 mL. Although he continued to have some cough, sputum production was markedly reduced, and his weight had increased by 3.1 Kg. His sputum continued to grow 2 strains of B. vietnamiensis with the previously identified antibiotic susceptibilities.
Discussion
Ivacaftor is a small-molecule potentiator of the CFTR anion channel and is the first drug that specifically targets defective CFTR protein that underlies CF disease. 5 It has been approved for the treatment of patients with CF who are 6 years of age and above, and have at least one copy of the G551D mutation.3,4 The G551D mutation, which is present in about 4% of patients with CF in the United States, is a Class III CFTR mutation that leads to impaired gating of cell membrane-localized CFTR protein.1,5 Ivacaftor enhances stimulated chloride transport by increasing the open probability of G551D-CFTR and reduces sodium and water absorption across cell membranes and the dehydration of the luminal surface liquid. 5
In 2 clinical trials of CF patients with mild-to-moderate lung disease (FEV1 of 40%–90% predicted) and at least one copy of the G551D mutation, ivacaftor was shown to induce a rapid, sustained improvement in FEV1, improve nutritional status, reduce CF-related symptoms, and pulmonary exacerbations.3,4 Preclinical data suggest that ivacaftor also may be effective in the treatment of other CFTR-gating mutations, which currently is being investigated in a phase 3 trial. 6 However, ivacaftor alone has no effect in patients with the F508del mutation, 7 which is present in 90% of CF patients in the United States, and which results in CFTR protein misfolding and degradation before reaching the cell membrane. However, phase 2 and dose–escalation data (unpublished data, Vertex Pharmaceuticals, Cambridge, MA) of ivacaftor in combination with the drug lumacaftor (VX-809) that helps F508del-CFTR move to the cell suggest that this combination may be efficacious in patients with 2 copies of the F508del mutation. Enrollment for a phase 3 trial of this combination in F508del homozygotes will begin soon in the United States.
Our case demonstrates the efficacy of ivacaftor in a CF patient with one copy of the G551D mutation with much greater impairment of lung function than those previously described in clinical trials, radiologic evidence of severe structural lung damage, and with clinical features consistent with cepacia syndrome. Cepacia syndrome was first described in 1984 in CF patients colonized with B. cepacia complex and is associated with a rapid, and usually fatal, deterioration in lung function. 8 Cepacia syndrome has been most commonly described with B. cenocepacia (genomovar III) and B. multivorans (genomovar II) infections,9–11 and to our knowledge, previously has not been reported in a CF patient infected with B. vietnamiensis. Our patient clearly had features consistent with this diagnosis given his rapid deterioration of lung function, persistent fevers, elevated inflammatory markers, and progressive weight loss. Further, he had no response to multiple antibiotic combinations, aggressive airway clearance, and nutritional support. At the time of starting ivacaftor, the patient was not a candidate for lung transplantation due to his persistent fevers, and the medical team believed that his condition was end stage. It is clear that his rapid clinical improvement was directly related to the initiation of treatment with ivacaftor. Of note, his condition transiently worsened shortly after beginning ivacaftor, triggered by the expectoration of copious amounts of thinned mucus. Thus, it may be reasonable to observe patients with very severe lung disease more closely when initiating ivacaftor.
In summary, this case demonstrates the effectiveness of ivacaftor in a 12-year-old patient with severe lung disease and clinical findings consistent with cepacia syndrome. While this patient continues to have significant impairment of lung function and severe irreversible structural lung damage, his nutritional status and overall quality of life are much improved since starting ivacaftor. This therapy may be beneficial and should be considered even in CF patients with end-stage lung disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.