
Abstract
Delivery of inhaled medications to children with asthma by a small-volume nebulizer is an antiquated method. Delivery by metered dose inhaler through a valved holding chamber with mask is at least equally effective, but more convenient, safer, faster, and less expensive. In addition, antistatic chambers increase the amount of drug delivered to the airways. This is an advantage for albuterol, but could increase the risk of long-term systemic adverse effects of inhaled corticosteroids at higher doses.
Comparison with Nebulizer Delivery
The MDI+VHC is more efficient, faster, more convenient, and less expensive than the SVN.5,6 Furthermore, in the emergency department treatment of asthma in children 5–17 years, when albuterol was given by MDI+VHC with mouthpiece (6–10 puffs per dose repeated at 20-min intervals), there was less tachycardia than when given by nebulizer. 2 Finally, in children under five years of age with moderate-to-severe asthma exacerbations treated in the emergency department, albuterol given by MDI+VHC was more effective than by a nebulizer in decreasing hospitalization and improving clinical score. 1 However, prescribers and parents of young children often believe that a nebulizer is more effective than an MDI+VHC. On the contrary, it has been shown that 4–10 puffs of albuterol sulfate delivered by MDI+VHC per dose is as effective as 2.5 mg of albuterol delivered by SVN when both are administered at 15–30-min intervals to infants and preschool children.4,5,7,8 The results of these studies apply to home treatment of exacerbations. However, another disadvantage of home nebulizer administration is that pathogenic organisms can be transmitted when nebulizers are not disinfected. 9
Budesonide inhalation suspension (Pulmicort Respules® and generics) is the only ICS available in the United States for nebulization. There are no studies comparing the delivery of budesonide by nebulizer to delivery by MDI+VHC in young children. However, a randomized, double-blind, placebo-controlled study has shown that fluticasone delivered through an MDI+VHC improves pulmonary function and controls symptoms in infants with recurrent wheeze. 10 Other studies have substantiated improved asthma control when an MDI+VHC was used to deliver fluticasone in children <2 years as well as older preschool children.11–15
Thus, the MDI+VHC is an efficient and effective way to deliver both albuterol and ICS to young children. However, as children get older, there is less rationale for using a VHC. For older children who can breath-hold, a dry powder inhaler for ICS and a breath-actuated MDI for a short-acting beta-agonist are more practical. These devices are cheaper and less cumbersome than a MDI+VHC for a child who is able to correctly use them (e.g., can breath-hold).
Valved Holding Chamber Characteristics
Delivery of inhaled drugs to young children by MDI+VHC with mask eliminates the need for coordination between actuation of the MDI and inhalation and the need to breath-hold. 16 However, the type of VHC is important because the amount of drug delivered to the airways varies depending on the VHC used.17,18 The FDA requires only in vitro studies of VHC for approval. Thus, these products are approved without a proof of safety, efficacy, or pulmonary deposition. In vitro aerosol deposition from a cascade impactor, such as the Anderson Cascade Impactor, is commonly used to compare the performance of various inhaled drug delivery systems.19,20 It provides information about the aerodynamic size of the droplets or particles that suggest where in the respiratory tract the drug might be deposited. 21 Despite the common use of this method, the clinical relevance of in vitro differences between devices and how much drug is actually delivered to the airways is inconsistent. For example, in vitro InspirEase® delivered a 50% greater fine-particle dose of fluticasone propionate than E-Z Spacer®, a generic equivalent, but in a randomized crossover pharmacokinetic study in children, there was no significant difference in the amount of fluticasone propionate delivered, assessed by the area under the curve, although the peak concentration was 25% greater after InspirEase®. 22
Delivery of a drug from a VHC to the airways may be increased or decreased depending upon the specific VHC used (size, shape, and chambers with electrostatic charge compared to those with no electrostatic charge), drug formulation (drug, propellant, and excipient), and patient characteristics (tidal volume, calm versus crying, and facemask seal). 23 Electrostatic charge on the inner wall of plastic spacers has been shown to reduce drug delivery by several fold in vivo.24–26 Both chambers with electrostatic charge (static chambers) and those without an electrostatic charge (antistatic chambers) are available in the United States (Table 1). The dose delivered to the airways from static chambers may vary considerably by up to 72% depending on day-to-day handling, especially when inhalation is delayed. 27 On the other hand, antistatic chambers consistently deliver a higher amount of medication to the airways.17,24,25,27,28
Relative cost when patient pays out of pocket.
New entry into the market. Cost not yet available.
However, the clinical relevance of increased drug delivery has been minimally studied. One example of such a study examined the bronchodilator response during nocturnal bronchospasm in adults. 29 Albuterol delivered through an antistatic chamber significantly improved FEV1 compared to delivery through a chamber with a static charge (Fig. 1). Similarly, decreasing the static charge increased the amount of fluticasone reaching the airways on average 17 ; however, this is unlikely to improve efficacy, since the dose–response curve for ICS in children is flat. 30 Specifically for fluticasone, the dose–response curve appears to plateau between 100 and 200 μg/day. 30 On the other hand, an antistatic chamber increases systemic exposure to ICS when compared to delivery by actuator alone 28 (Fig. 2). This raises long-term safety concerns in fully adherent patients (e.g., growth suppression 31 ) if higher doses are administered. 31

Bronchodilator response to albuterol delivered by an antistatic or static chamber. This was a randomized, double-blind, double-dummy, single-center, crossover study comparing the bronchodilator response to hydrofluoro-alkane (HFA) albuterol-metered dose inhaler, after 1, 2, and 4 cumulative puffs at 15-min intervals, delivered through an antistatic and a static chamber during nocturnal bronchospasm. Subjects were ≥18 years and slept in the Clinical Research Center of Shands Hospital at the University of Florida. FEV1 was measured before and 15 min after each dose upon awakening with asthma symptoms or at 4 am. Of 11 randomized subjects, 7 completed the study. There was a significant difference between treatments at each dose. The error bars represent standard deviations. 29 Reproduced with permission from Respiratory Care.
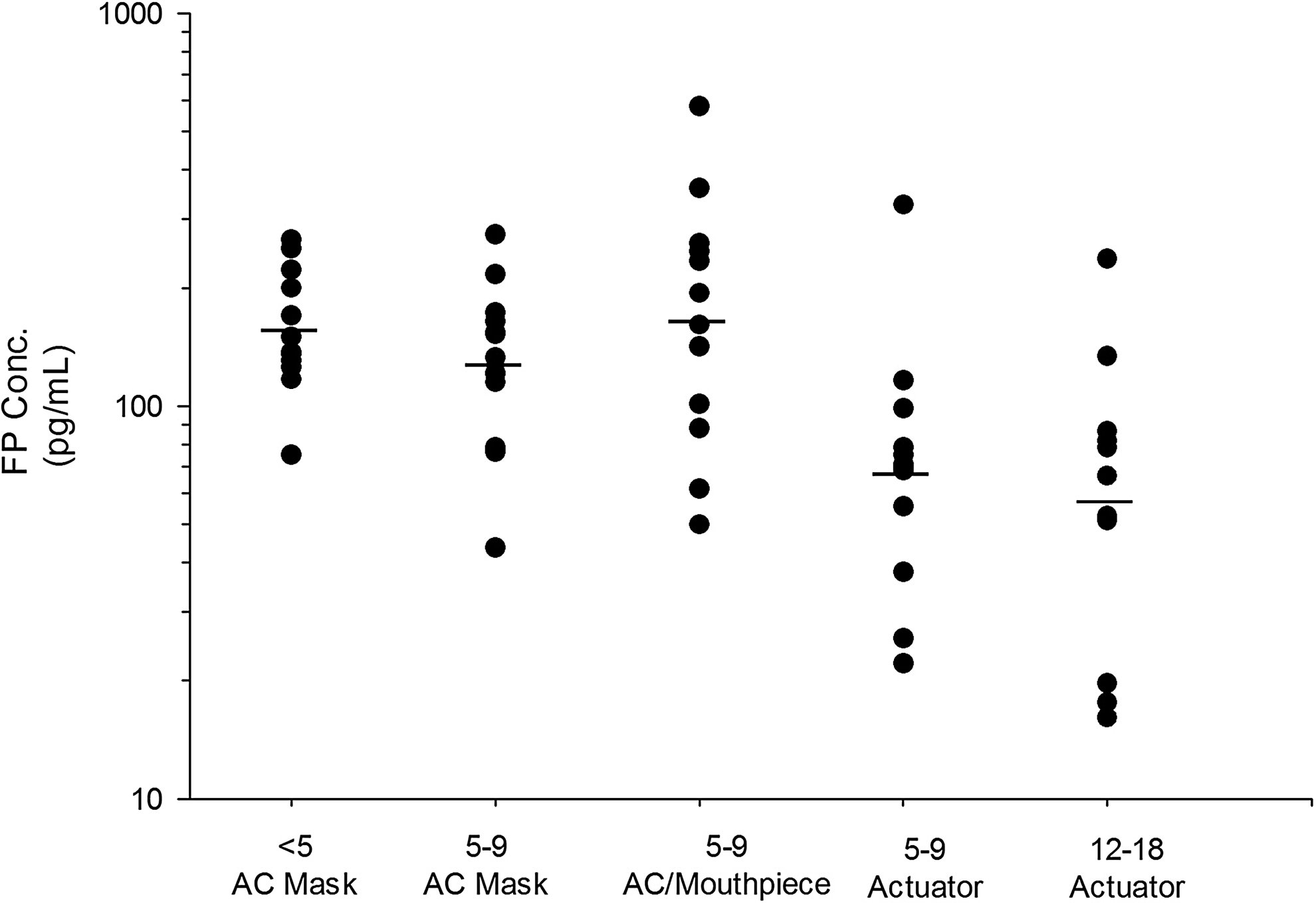
Systemic exposure to fluticasone delivered by actuator and antistatic valved holding chamber. This was a single-center nonrandomized, unblinded, cross-sectional study of steady-state fluticasone propionate (FP) plasma concentrations, a surrogate for the amount of drug delivered to the airways. All subjects received 220 μg of fluticasone propionate twice a day for at least three days. FP plasma concentrations were measured 1 h after the final dose. FP concentrations in the two age groups receiving the drug by actuator alone were significantly lower than all groups receiving the drug through an antistatic chamber, indicating less drug delivered. 28 Reproduced with permission from Elsevier, the publisher of the Journal of Allergy and Clinical Immunology.
Obstacles
So, why is every asthmatic child under five years not prescribed an antistatic chamber with mask? Unfortunately, a number of obstacles exist that prevent this.
First, lack of insurance coverage is a common problem. In many states, insurance carriers, including Medicaid, do not cover chambers, but pay for nebulizers. In primary care offices, respiratory companies have made it very easy to prescribe nebulizers. They provide the primary care office with numerous types of nebulizers (in the shape of loveable animals (penguins, panda bears, etc.), on consignment, so that when a patient presents with an initial asthma exacerbation, the nebulizers are readily available for the providers to hand out to their patients (requiring the filling out of paperwork for the respiratory care company). A few primary care providers have overcome this obstacle by buying antistatic chambers in bulk and selling them to their patients.
The second obstacle is the misinformed parent. A parent given a nebulizer at the first asthma exacerbation, which provided relief for their child, is reluctant to try the MDI+VHC. Despite the fact that delivery by nebulizer is more cumbersome, not mobile, and is loud, they prefer to use it because it worked for the initial exacerbation. Additionally, providers who are unaware of the literature on MDI+VHC may misinform the parents that the nebulizer is more effective.
The final obstacle is a problem with pharmacy substitution of inequivalent products. We have found that some chain pharmacy technicians substitute the OptiChamber® when we prescribe AeroChamber plus with FlowVu®. The OptiChamber accumulates a static charge and delivers less drug in vitro 32 (Fig. 3). Additionally, it lacks an inspiratory flow indicator, which gives the parents feedback that the child is inhaling the drug. There is a lack of information about chambers among pharmacists, and often we have encountered a Florida Medicaid patient who was told that chambers are not covered and asked to pay out of pocket $60–70 when the AeroChamber®, but not the OptiChamber, is 100% covered by Florida Medicaid for children.

In vitro fine-particle dose of fluticasone propionate delivered by different chambers. The study involved the OptiHaler Advantage, a plastic valved holding chamber (VHC) that accumulates an electrostatic charge, and two antistatic devices, the Pari-Vortex, an aluminum chamber that conducts electricity, and the AeroChamber Max®, which has a coating on the inner wall that dissipates a static charge. Three units of each VHC were studied new out of the package, primed with 14 puffs of fluticasone propionate, and washed (in mild detergent, rinsed, and air-dried). The fine-particle dose of fluticasone was measured by an Andersen Cascade Impactor after discharge of fluticasone into an in vitro infant nose–throat model (SAINT). The OptiChamber® delivered a significantly lower lung dose than the two antistatic chambers under all three test conditions. 32 Reproduced by permission of Dr. Geller.
Cleaning Instructions
Cleaning instructions for VHCs are simple and can be easily taught to parents and providers. We give parents the following simple cleaning instructions: disassemble the chamber and soak the parts for 15 min in a mild solution of liquid dish detergent with lukewarm clean water; then, rinse the parts with clean water and allow the chamber to air-dry in a vertical position. However, in clinics that reuse devices for demonstration to many patients, the chamber is cleaned with warm soapy water, rinsed, and then submerged in Cidex ortho-phthalaldehyde for 12 min (Appendix). Use of this protocol has been approved by our hospital Infection Control Committee.
Footnotes
Acknowledgments
Dr. ElMallah is funded by the College of Medicine, and the Parker B Francis Foundation. Dr. Hendeles is funded by the College of Pharmacy.
Author Disclosure Statement
Dr. ElMallah has no conflicts of interest to disclose. Dr. Hendeles has received reimbursement of travel expenses from Monaghan Medical to make presentations at scientific meetings in 2009, 2011, and 2012.