
Abstract
An investigation of immunopathogenetic mechanisms of obesity-associated asthma may demonstrate novel therapeutic targets. The aim of this study was to compare levels of T-helper lymphocyte (Th)1, Th2, regulatory T lymphocyte (Treg), and Th17 cytokines secreted by peripheral blood mononuclear cell culture (PBMC) in response to nonspecific stimulation in obese and nonobese children with asthma. Obese and nonobese children with asthma aged 5–16 were enrolled into this case-control study consecutively. Age at asthma diagnosis and clinical severity were recorded. A skin prick test was performed. Serum adipokine levels and PBMC supernatant interleukin (IL)-4, IL-10, IL-17, IL-23, interferon (IFN)γ, and transforming growth factor (TGF)-β levels were measured. Mean (±standard deviation) ages of obese (n=28) and nonobese (n=39) children with asthma were 8.7±2.9 and 10.5±3.2, respectively. Asthma symptom score was higher, and age at asthma diagnosis was lower in obese compared with nonobese children with asthma (P=0.03 and P=0.004, respectively). Leptin levels were significantly higher in obese than in nonobese asthma group (P<0.001). IL-10 and IL-17 levels in obese group were significantly lower than in nonobese group (P=0.005 and P=0.017, respectively). On the other hand, TGF-β levels were significantly higher in obese compared with nonobese children with asthma (P=0.015). IL-4, IL-23, and IFNγ levels were not significantly different between the groups (P<0.05 for all). Low IL-10 and high TGF-β levels in obese compared with nonobese children with asthma might indicate lower anti-inflammatory cytokine secretion and Treg function as well as a higher remodeling process in obesity-associated asthma in children.
Introduction
C
Despite the fact that adipokines are thought to play an important role in the increase in systemic inflammatory status, it has been documented that obesity is not associated with increased airway inflammation, and asthma in obese children is less commonly associated with bronchial hyperreactivity compared with nonobese children.1,11,12 Therefore, asthma that develops in obese children is more likely to be associated with systemic inflammatory immune response. The clarification of the exact cell and mediator components of this inflammation is essential in delineation of the exact pathogenesis and in development of novel therapeutic regimens for this specific asthma phenotype.
The aim of this study was to compare the levels of Th1, Th2, regulatory T lymphocyte (Treg), and Th17 cytokines secreted by peripheral mononuclear cells in response to nonspecific stimulation in obese and nonobese children with asthma.
Materials and Methods
Study population
This study was carried out in a university hospital Pediatric Allergy Clinic. Obese and nonobese children with mild persistent asthma aged 5–16 years who presented to the Pediatric Allergy and Pulmonology outpatient clinic were enrolled consecutively.
Asthma was diagnosed based on history of recurrent cough and wheezing with prolonged expiration time that demonstrated reversibility (clinical improvement or 12% or more improvement in forced expiratory volume in one second) with salbutamol inhalation. 13 Mild persistent asthma was defined as the presence of symptoms more than once a week but less than once a day, exacerbations affecting activity, or nocturnal symptoms more than twice a month. 13 Obesity was defined as body mass index (BMI) above 90th percentile for age and gender.14,15 BMI was calculated according to the formula: weight (kg)/height2 (m2).
Children who had an acute asthma exacerbation or acute illness during the previous month and the ones who received inhaled or systemic steroid treatment or any other anti-inflammatory treatment within the previous 3 month period were excluded from the study. Moreover, children who have any other inflammatory disease were excluded from the study group.
Study design and ethical procedures
This was a prospective case control study. The two study groups were obese children with asthma and nonobese children with asthma.
This study was approved by the Institutional Ethics Board of Celal Bayar University, Manisa, Turkey, and written informed consent was obtained from the parents of all the children who enrolled in the study.
Data collection
Age and gender of all the children who enrolled in the study were recorded as well as the age at diagnosis of asthma and the clinical severity of asthma. A skin prick test was performed for all children according to the European Academy of Allergy and Clinical Immunology (EAACI) guidelines using commercial allergen extracts for common inhalant allergens, including dermatophagoides, grass pollens, olea, molds, cat, dog, and cockroach allergens (Allergopharma Ltd, Reinbek, Germany). 16 Skin prick test positivity was used to define allergy to inhalant antigens.
Blood was drawn from all obese and nonobese subjects for measurement of serum adipokine levels and for peripheral blood mononuclear cell cultures (PBMCs). Cells in the PBMC were stimulated with the addition of phytohemagglutinin (20 μL) to PBMC plates. Interleukin (IL)-4, IL-10, IL-17, IL-23, interferon (IFN)γ, and transforming growth factor (TGF)-β levels were measured in the supernatants obtained from PBMC by enzyme-linked immunosorbent assay (ELISA) method.
Patient reported asthma symptom score
Asthma symptom score that was used in this study included five items reflecting chronic asthma symptoms such as dyspnea, tightness in chest, day-time wheeze, nocturnal wheeze, and daily performance during the previous 3-month period. 17 The score was filled in by one investigator by questioning the parent. Scoring of the items increased from 0 to 3 as the severity increased. Total score is expressed as the sum of all the scores of the items.
Peripheral blood mononuclear cell culture method
PBMC were prepared by standard Ficoll-paque density gradient centrifugation. 18 Blood samples for PBMC were poured into tubes of 50 mL and phosphate-buffer solution (PBS) at the same volume as the blood samples were added onto it. Then, Biocoll solution at the same volume of the initial blood sample volume was added on this mixture. The tubes were centrifuged for 20 min at 2,300 rpm. Gray–white colored cells that appear at the junction of PBS and Biocoll at the end of centrifugation were taken into a new tube of 15 mL.
PBS at the same volume of the collected cells was added onto the tube and mixed. Then, the mixture was centrifuged for 10 min at 2,000 rpm. The supernatant at the top of the centrifuged mixture was removed. To lyze the remaining erythrocytes, 1 mL of water and 1 mL of PBS were added one after the other. The total mixture was centrifuged at 1,300 rpm for 5 min, and the supernatant was removed. Four milliliters of RPMI-1640 medium containing 1%
For cell count, 40 μL of the sample was obtained, and cell number in a milliliter was counted on a thoma slide after mixing with 40 tryptan blue. No other procedure was performed on control group samples. Mean number of cells per well used for the cultures was 3×106 cells/mL. Onto the other Petri dish, 20 μL phytohemaglutinin was added and control versus disease groups were incubated for 48 h at 37°C. Culture media were collected afterward, and the supernatant was collected. Supernatants obtained were stored under −20°C until cytokine measurements were taken.
Measurement of serum adipokine levels
Serum levels of adipokines were measured using the ELISA method. All ELISA measurements were performed according to the manufacturer's instructions. Visfatin levels were measured with the immunodiagnostic ELISA kit (Adipogen, Liestal, Switzerland), while adionectin was measured with the immunodiagnostic (Stubenwald, Bensheim, Germany) kit. Leptin concentrations were assayed using an ELISA kit (DRG Diagnostics, Marburg, Germany).
Measurement of cytokine levels in supernatants
Cell culture cytokine concentrations were assayed using ELISA method. All ELISA measurements were performed according to the manufacturer's instructions. All measurements were carried out in duplicate, and the mean of the two measurements gave the final result. IL-4, IL-10, IFNγ, and TGF-β levels were measured using the kit from Diaclone (Besançon, France). Cell culture IL-17A concentrations were assayed using an ELISA kit from Bender MedSystems (Vienna, Austria), while those of IL-23 levels were measured using eBioscience (Vienna, Austria) ELISA kit.
Statistical analysis
Statistical analysis of this study was performed using SPSS 15.0 computer software (Chicago, IL). Demographic characteristics were analyzed using descriptive statistics. Gender was reported as frequencies. Age was described as mean±standard deviation (SD), while cytokine and adipokine levels were expressed as median (interquartile range). Nonparametric Mann–Whitney U test was used to compare cytokine and adipokine levels between the groups. Nonparametric Spearman analysis was performed to analyze for correlation between adipokine and cytokine levels. IFNγ levels were above the higher limit detection of the ELISA kit in 24 samples; therefore, these values were accepted as 2,000 mg/dL, which is the highest limit of detection. Similarly, IL-10 levels were above the highest limit of detection in 36 samples, and these values were accepted as 600 mg/dL, which is the highest limit of detection. Lastly, IL-23 levels were less than the lower limit of detection in 17 samples; so, these were accepted as 1 mg/dL, which is the lowest limit of detection for statistical purposes. Statistical significance was defined as a P-value<0.05.
Results
Sociodemographic characteristics of the study population
Obese asthma group was composed of 28 children (20 male, 8 female) with a mean±SD age of 8.7±2.9 years, and the nonobese asthma group was composed of 39 children (24 male, 15 female) with a mean±SD age of 10.5±3.2 years (P=0.02). Among the obese group, 32.1% was allergic; while among the nonobese group, 48.7% was allergic to an inhalant allergen.
In obese children, age at initiation of asthma findings was significantly lower compared with the nonobese children [median (interquartile range) of 5 (1.5–8.3) versus 6 (4–12), respectively, P=0.03]. On the hand, asthma symptom score was significantly higher in obese children [6 (4–8) versus 4 (2–6), respectively, P=0.004].
Serum adipokine levels of the study groups
Leptin levels were significantly higher in the obese asthma group when compared with the nonobese asthma group (P<0.001). However, adiponectin and visfatin were similar between the two groups (P=0.79 and P=0.21, respectively) (Table 1).
Mann–Whitney U test.
Median (interquartile range).
Cytokine levels of the peripheral mononuclear cell culture supernatants
In obese children with asthma, IL-10 and IL-17 levels were significantly lower than those in nonobese children (P=0.005 and P=0.017, respectively) (Figs. 1 and 2). On the other hand, TGF-β levels were significantly higher in the obese asthma group compared with that in the nonobese asthma group (P=0.015) (Fig. 3). IL-4, IL-23, and IFNγ levels were not significantly different between the two study groups (P<0.05 for all) (Table 2).
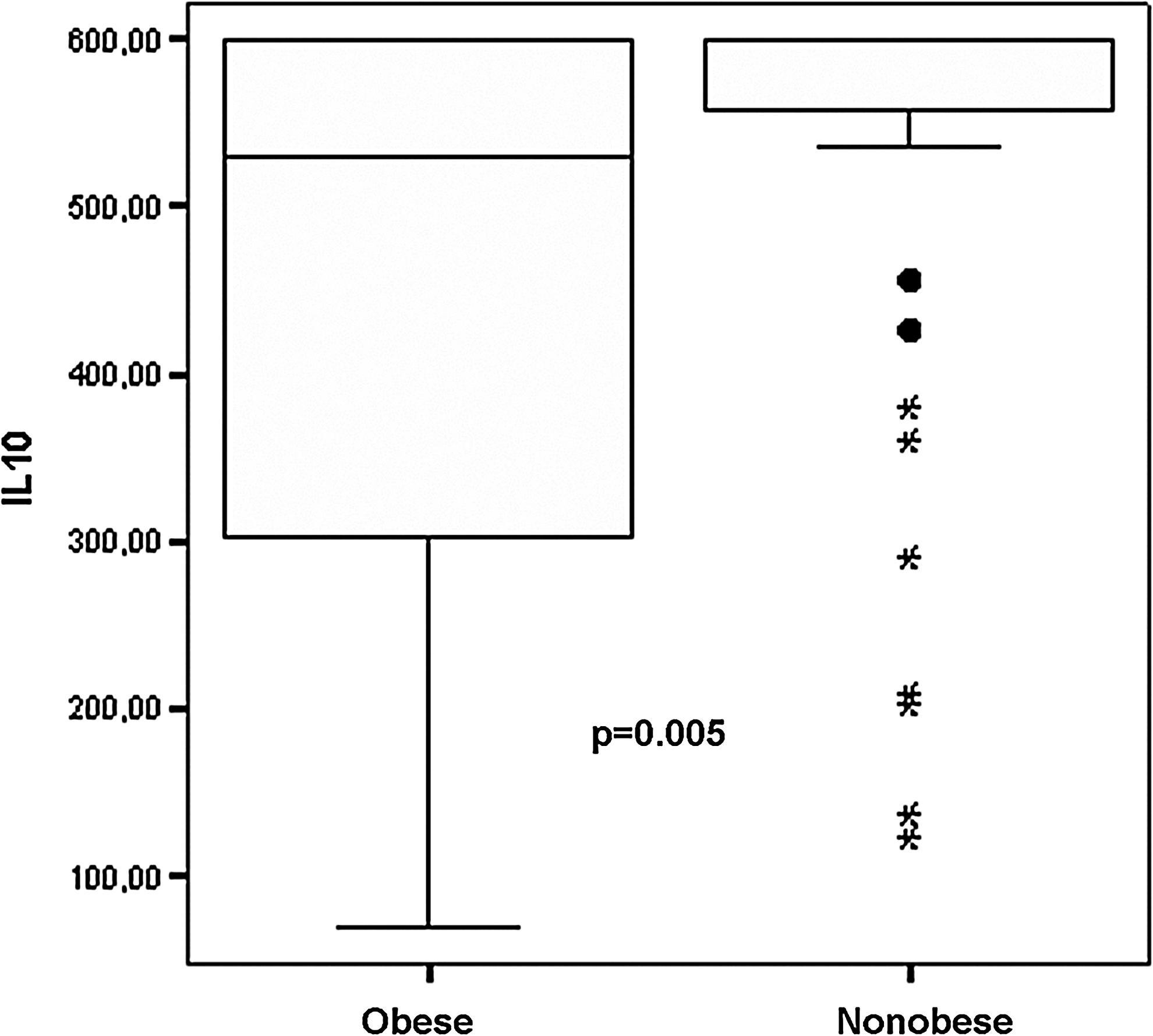
Interleukin (IL)-10 levels in obese and nonobese asthma groups. Black circles indicate outliers, and asterisks indicate extreme outliers.
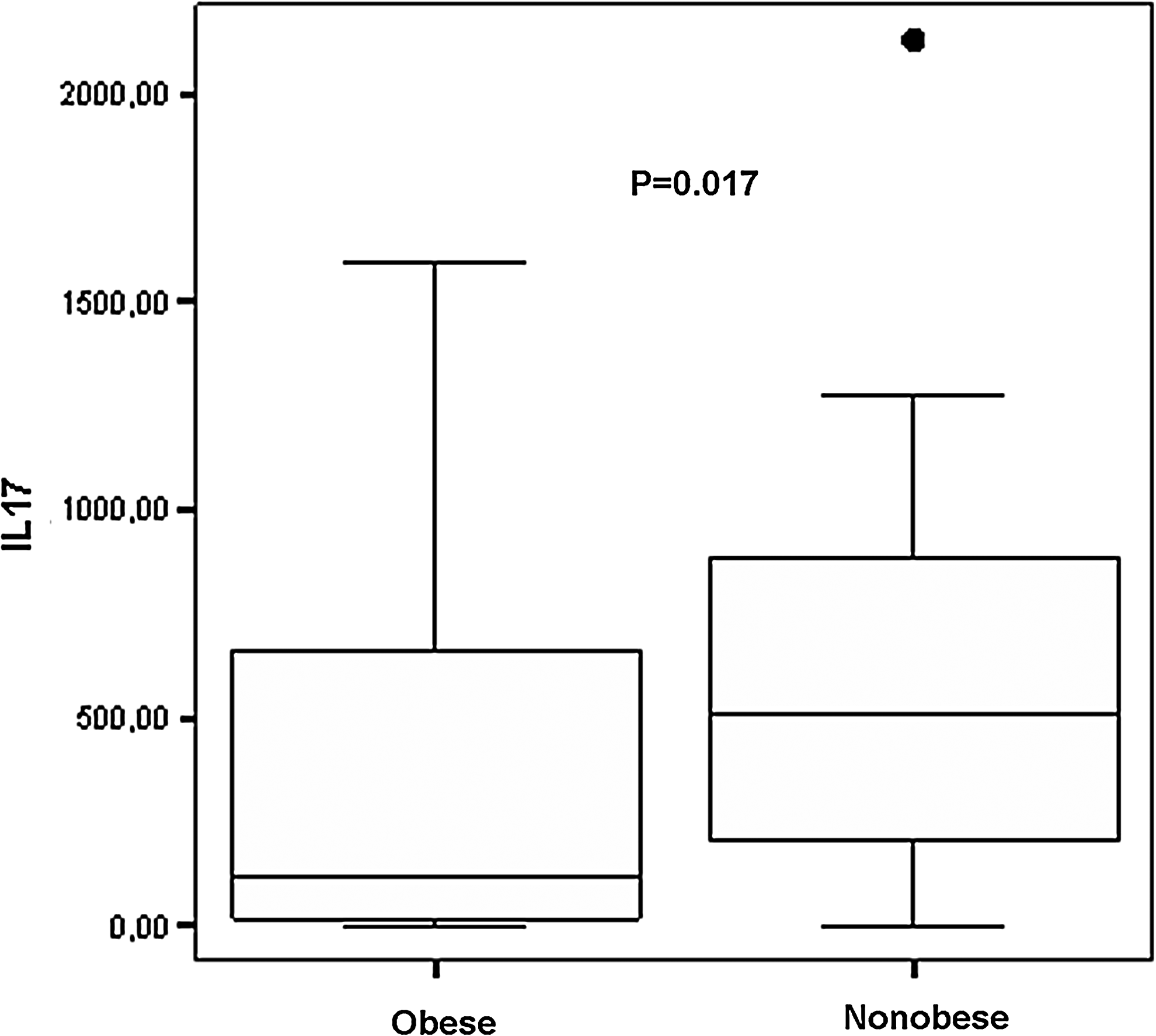
IL-17 levels in obese and nonobese asthma groups. Black circles indicate outliers.
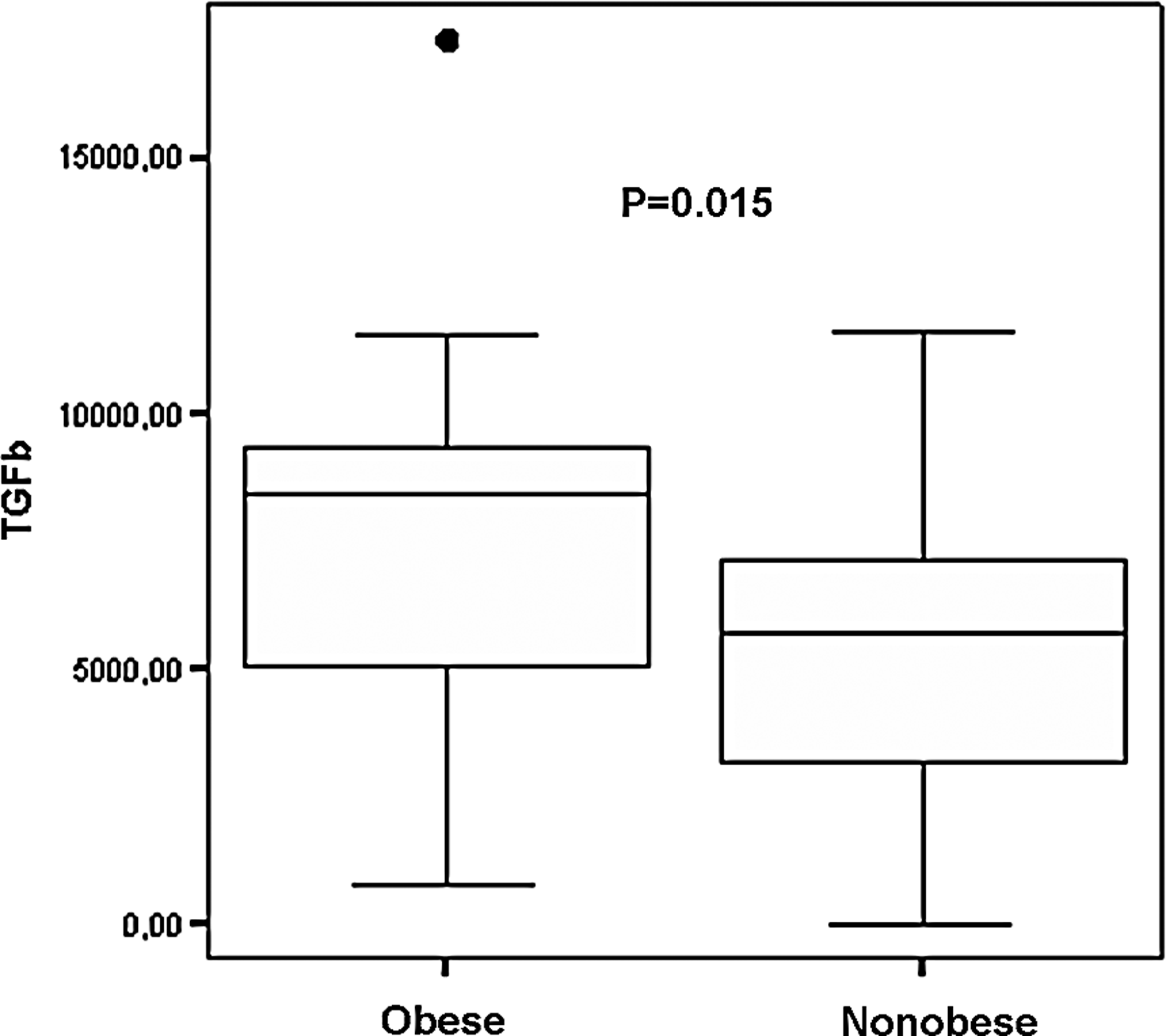
Transforming growth factor (TGF)-β levels in obese and nonobese asthma groups. Black circles indicate outliers.
Median (interquartile range).
Mann–Whitney U test.
PBMC, peripheral blood mononuclear cell culture; IL, interleukin; IFN, interferon; TGF, transforming growth factor.
Correlation of adipokine and cytokine levels
Adipokine levels of the study population were not correlated with any of the cytokine levels when analyzed as a whole group, but correlation analysis of the obese and nonobese groups separately revealed that leptin and visfation were negatively correlated with IL-23 levels in the obese group (ρ=−0.42 and ρ=−0.41, P=0.03 for both). There was no correlation between adipokine and cytokine levels in the nonobese group.
Discussion
The results of this study indicated that among the adipokines leptin, adiponectin, and visfatin, only leptin was significantly different between obese and nonobese children with asthma. Evaluation of the cytokine response of PBMCs to nonspecific antigenic stimulation revealed that inhibitory cytokine IL-10 response is significantly lower in obese children compared with the nonobese children with asthma. Similarly, IL-17, which is a mediator of neutrophilic inflammation, is lower in obese compared with nonobese children with asthma. On the other hand, TGF-β that mediates fibrosis and remodeling is significantly higher in obese than nonobese children with asthma. Moreover, the results indicated that asthma severity was higher and asthma started at an earlier age in obese children when compared with the nonobese children with asthma.
Obesity-associated asthma is a distinct phenotype of asthma syndromes that is associated with different endotypes. 4 The etiopathogenetic backgrounds of this phenotype depend on different factors such as the influence of obesity on lung function tests, symptom score, bronchial hyper-reactivity, and, most prominently, on systemic inflammatory state, especially via adipokines such as leptin, adiponectin, and visfatin. 19 Leptin stimulates proinflammatory cytokine secretion from monocytes and macrophages, inhibits regulatory T cells but does not influence Th2 response. 3 Therefore, it is proposed to play a major role in the inflammation in obesity-associated asthma. This study indicated that leptin levels were significantly higher in obese children with asthma compared with nonobese children with asthma. However, the results of this study failed to detect a significant difference in adiponectin levels between obese and nonobese children with asthma. Enrollment of both atopic and nonatopic asthmatic children in the study groups might have precluded detection of the difference in adiponectin levels, as the decrease in adiponectin is proposed to be associated with nonatopic asthma but not with atopic asthma. 5 Visfatin is an adipokine that has a debatable role in obesity; however, it is known to have regulatory activity in inflammation.20,21 The results of our study did not support a role of visfatin in obesity-associated asthma.
Similar to previous research, obese children with asthma in our study reported worse asthma symptom scores.22,23 Higher clinical severity of asthma in obese children may be attributed to many factors, one of which is the higher level of inflammation that decreases steroid responsiveness. Similarly, age at diagnosis of asthma in obese children with asthma in our study was younger than in nonobese children with asthma.
Despite the fact that low-grade systemic inflammation has been clearly reported in obesity, the detailed aspects of this inflammatory response have not been clarified. 3 The cytokine response of the PBMCs from obese and nonobese children with asthma enrolled in our study showed that there was a significant difference between levels of inhibitory and fibrotic cytokines and Th17 response but not in Th1 or Th2 response estimated by IFNγ and IL-4 levels, respectively. Serum levels of IL-10 levels in obese children have been reported to be lower than nonobese children, and low levels of IL-10 have been reported to be associated with worse lung function test results in asthmatic patients.24,25 These results from previous studies point out a protective role of this cytokine, and the results of our study showed that levels of IL-10 are lower in obese children with asthma compared with the nonobese children, indicating a role for low levels in the development of obesity-associated asthma in children. Moreover, considering that Tregs form an important source of IL-10, obesity-associated asthma may also be associated with a decrease in T regulatory function. 7
IL-17 has been suggested to play a role in severe asthma, which is predominantly associated with neutrophilic inflammation.7,8,26 In our study, we measured IL-17, because obesity-associated asthma has more severe clinical characteristics and has been proposed to be a phenotype that is associated with steroid-resistant asthma endotype. 4 However, the results of our study indicated that IL-17 levels secreted from PBMCs of nonobese children with asthma were significantly higher than those from obese children with asthma. This finding suggests that IL17 and neutrophilic inflammation driven by this cytokine does not play a role in the increased severity of obesity-associated asthma. On the other hand, despite correlation of IL-23 with leptin and visfatin levels in the obese asthma group, we could not detect a difference in IL-23, which is an inducer of Th17 cells and IL-17 secretion between the study groups. 8 This might indicate the influence of another cytokine on IL-17 secretion from Th17 cells, and it is known that IL-17 secretion is influenced by many other cytokines such as IL-10 and TGF-β. 7 Therefore, the difference in IL-17 between the two groups may be due to the difference in IL-10 and TGF-β levels between the two groups. The correlation of IL-23 and leptin might be attributed to this.
Another cytokine that was found to be significantly different between obese and nonobese children with asthma in our study was TGF-β. This cytokine induces development of regulatory T cells in mice. 27 Moreover, it has been reported to play a major role in airway remodeling in asthma due to its influence on fibroblasts and extracellular matrix enzymes, leading to fibrosis.27,28 Considering these data, higher TGF-β levels in the obese asthma group in this study compared with the nonobese asthma group indicate a higher potential for remodeling in obesity-associated asthma. Further research needs to assess whether Treg population is increased in this population owing to this increase in TGF-β. This higher potential for remodeling may also contribute to the more severe clinical outcome in this population and necessitates investigation of the potential therapeutic potential of TGF-β inhibition in obesity-associated asthma.
Our research has not shown a difference in IL-4 and IFNγ secretion of PBMC between obese and nonobese children with asthma. INFγ is the prototypical Th1 cytokine, whereas IL-4 is one of the Th2 cytokines.9,10 Absence of a difference in these cytokines between the two groups of our study might indicate that obesity-associated asthma has a pathogenetic basis that does not include an imbalance of Th1 and Th2 lymphocytes or there are more important factors in pathogenesis which override this imbalance.
The major limitation of this study was the wide distribution of cytokine levels in the samples, which decreased the power of our study. In addition, lack of an obese nonasthma group prevented any interpretation on the influence of obesity on these cytokine levels apart from asthma, but this was not a primary aim of the study. Moreover, inclusion of a flow cytometric analysis of the cell subgroups might have provided additional information about the cellular component of the inflammation in obesity-associated asthma. Moreover, assessment of systemic inflammation with a serum marker might have added more value to our interpretation of obesity on systemic inflammation but this has been clearly stated in previous research, so we did not perform a reassessment.
In conclusion, the low levels of anti-inflammatory cytokine, IL-10 secretion by PBMCs indicative of decreased Treg function, might play a role in the pathogenesis of obesity-associated asthma. The higher levels of TGF-β might have a role in the more severe clinical findings in obesity-associated asthma due to the increase in the remodeling process. Considering that remodeling is an important component of future asthma morbidity, TGF-β blockage may be investigated further for its therapeutic potential. However, IL-17, which is associated with neutrophilic inflammation in severe asthma, does not seem to play a significant role in obesity-associated asthma phenotype.
Footnotes
Acknowledgments
The authors thank Dr. Cecilia M. Patino, who is a MECOR (Methods in Epidemiologic, Clinical and Operations Research) course faculty responsible for the critical editing of this article.The project was funded by the Scientific Research Fund of Celal Bayar University. The project was performed in the Celal Bayar University Medical Faculty Department of Pediatric Allergy and Pulmonology, Manisa, Turkey.
Author Disclosure Statement
None of the authors declare competing financial interests.