
Abstract
A mannose-binding lectin (MBL) deficiency, due to MBL2 gene polymorphisms, is suggested to increase susceptibility to respiratory tract infections, particularly in young children. This study aimed to determine whether a MBL deficiency might be associated with pulmonary morbidity in children with recurrent pulmonary infections of unknown pathogenesis. We performed a retrospective, cross-sectional study on children referred to a tertiary pediatric pulmonary center between 2006 and 2011. We included children with a conclusive MBL2 genotype that exhibited recurrent pulmonary infections without any obvious explanatory findings. Pulmonary morbidity was estimated by lung function, body mass index, antibiotic prescriptions, and the odds ratio of radiological structural lung changes, assessed with chest X-rays or high-resolution computed tomography. One hundred thirteen children were included. No significant differences in lung function (z-scores), body mass index, or the number of annual courses of antibiotics per year could be demonstrated between high- and low-expression MBL2 genotypes. The odds ratio of structural lung changes was not related to the MBL2 genotypes. Pulmonary morbidity was not associated with low-expression MBL2 genotypes in a highly selected, although heterogeneous, group of children with recurrent pulmonary infections of unknown pathogenesis. Thus, most likely, a MBL genotyping cannot be used as a single, explanatory, causative factor for detecting differences in pulmonary morbidity in children.
Background
A MBL deficiency arises from polymorphisms in the MBL2 gene located on chromosome 10 and results in low serum levels of MBL. 2 The normal, wild-type allele, A, has 3 variant alleles, B, C, and D, which are collectively referred to as O. The MBL serum concentration is further influenced by promoter polymorphisms, particularly in X/Y promoters. The Y promoter is correlated with high expression and the X promoter with the lower expression.3,4
It is estimated that, among the general Caucasian population, 5% are homozygous and 30% are heterozygous for the MBL O allele, 5 but frequencies vary according to ethnicity and worldwide geographic variations.4,6 Among the Danish Caucasian population, the frequency of the MBL2 O/O alleles is estimated to be 5%, the frequency of A/O is 37%, and the frequency of A/A is 58%. 7
MBL deficiency is used to classify some states of immunodeficiency, but the definition of MBL deficiency is unclear. There is significant overlap in MBL serum levels among the different MBL2 genotypes. Cutoff levels vary widely among studies for defining a MBL-deficient state. 8 However, a cutoff level less than 500 ng/mL has been proposed, 9 and this is currently used in Denmark.
MBL deficiency is believed to contribute to an increased susceptibility to various infectious diseases in children, 10 including respiratory tract infections11,12 and otitis media. 13 It is also associated with the development of asthma in school-aged children who had bronchiolitis in infancy. 14 MBL is considered particularly important during the vulnerable period of infancy, between the disappearance of maternal antibodies and maturation of the infant's adaptive immune responses. 11
In some children, the pathogenesis of recurrent respiratory infections remains unresolved, despite intensive investigation. Preliminary investigations can at least exclude cystic fibrosis (CF), primary ciliary dyskinesia (PCD), obvious anatomic airway abnormalities, and cellular or humoral immunodeficiencies. A MBL measurement has been proposed as a first line test to investigate unexplained recurrent respiratory infections, 15 but its role is not entirely clear. We aimed to explore whether MBL deficiency could serve as a single, explanatory, causative factor for differences in pulmonary morbidity that are reflected in antibiotic use, lung function, or radiological evidence [chest X-ray or high-resolution computed tomography (HRCT)] of chronic, structural lung damage in a heterogeneous group of children. We also aimed to assess the MBL genotype distribution among the children specifically referred to our department and compare that distribution to that of the Danish background population.
Methods
This retrospective, cross-sectional, cohort study was based on a review of medical records. The study was conducted at a tertiary, pediatric pulmonary center, Rigshospitalet, in Copenhagen, Denmark.
Patients
Children, 0–16 years of age, with an available, previous assessment of the MBL2 genotype were eligible when they had no anatomical airway/esophageal abnormalities, malignancies, or neurological diseases. They were referred by their general practitioner or secondary pediatric centers for further diagnostic work-up investigations between January 2006 and January 2011. The reason for the referral was a composite history of recurrent pulmonary infections treated with antibiotics and/or pneumonic infiltration on chest X-ray and/or referral to a pediatric department due to recurrent airway infections. The exact number of previous infections was not established.
Patients were excluded when they had a diagnosis of CF, PCD, any other chronic lung disease, or other established immunodeficiencies (e.g., agammaglobinaemia, IgA and IgG subclass deficiencies, complement deficiency, B-cell or T-cell disorders) that might inherently increase the risk of pulmonary morbidity.
Endpoints
Our primary outcomes were pulmonary morbidity and structural lung changes. Morbidity was assessed as the number of antibiotic treatments received per year, body mass index (BMI), and measures of lung function (spirometry and whole body plethysmography). Structural lung changes were assessed by the latest available chest X-ray and HRCT obtained at our center.
The number of antibiotic treatments received per year after referral was calculated based on the hospital electronic patient medicine registration system. Only antibiotic treatments prescribed from the Pediatric Pulmonary Service were included, because monitoring and treatment were predominantly provided from that center.
The lung function (Jaeger Master Screen Pro, Hochberg, Germany) was assessed, depending on the level of cooperation, by either spirometry (children older than 5–6 years) according to European Respiratory Society guidelines, 16 or whole body plethysmography (for younger children) according to Bisgaard and Nielsen. 17 Abnormal spirometry defined as a z-score is less than −1.96, according to reference values provided in the Excel add-in program: least mean squares of growth all ages. 18 Abnormal specific airway resistance (sRaw) was defined as the z-score >1.96 based on references from Kirkby et al. 19
Chest X-rays and HRCTs were described by pediatric radiologists and assigned to groups of children without or with chronic structural lung changes; the latter group included chronic atelectasis, bronchiectasis, and airtrapping. Abnormality assessments based on HRCTs were considered superior to those based on chest X-rays and the choice of modality was on discretion of the clinician, dependent on clinical severity.
MBL2 genotypes were determined by sequence-specific priming, polymerase chain reaction, as described elsewhere. 20 Different MBL2 genotypes have been associated with different serum levels of MBL. 11 Genotype A/A was associated with sufficient MBL levels. Three genotype subgroups were associated with low MBL levels: the YA/O genotype was associated with intermediate low levels of MBL; the XA/O genotype was associated with severely low levels of MBL; and the O/O genotype was associated with no functional MBL. 11 To facilitate the detection of a difference between the groups, our primary analysis consisted of a comparison between A/A and A/O (YA/O and XA/O) versus O/O, secondly between A/A and YA/O versus XA/O and O/O, and finally, comparisons between each subgroup alone (A/A versus XA/O versus YA/O versus O/O).
Statistics
Statistical analyses were conducted with MedCalc® (Version 12.3.0.0; MedCalc Software, Mariakerke, Belgium). Data were presented as the mean and 95% confidence interval (95% CI) or the median and range, according to the normality distribution of the data. Continuous data were analyzed with the unpaired t-test or nonparametric tests; either the Mann–Whitney or the one-way ANOVA (Kruskal–Wallis test), as appropriate. Categorical data were analyzed with the Fisher's exact test or the chi-square test, as appropriate. The odds ratio was used to describe structural lung damage, according to the retrospective study design. A 2-tailed P value <0.05 was considered significant.
Results
The MBL2 genotype was assessed in 270 children, who had been referred to our pulmonary department during the study period. In 141 children, an existing diagnosis of chronic lung disease or an established immune deficiency was known; therefore, those children were excluded. In 16 children, the result was not available. Hence, for further analyses, we included 113 children (males 67%) who had a median age (range) of 3 (0–16) years at the time of the MBL2 genotype assessment. The patient inclusion flow chart is presented in Fig. 1.

Patient inclusion/exclusion flow chart. During the period of 2006 to 2011, a total of 270 children with pulmonary diseases underwent measurements of MBL serum levels. Patients were excluded from the current study, when they had a history of various specific diseases and other immunodeficiency conditions (apart from MBL deficiency), when some records were missing, and when the MBL genotype was not determined. A total of 113 children were included in the final analyses. MBL, mannose-binding lectin; CBP, ciliary beat pattern (observed in the ciliary lining of nasal mucosa biopsies); TEM, transmission electron microscopy (of cilia ultrastructure).
The distribution of MBL2 genotypes is presented in Table 1. The frequency of the O/O genotype was significantly higher than predicted from the Danish background population (Hardy–Weinberg equilibrium), but the distributions of the other genotypes were similar to those of the background population. The distribution of the actual MBL serum level in 86% of the study cohort (serum level missing in n=16) according to MBL2 genotypes is presented in Fig. 2 and demonstrates a significantly higher median MBL level in the A/A group (2609 ng/mL) compared to both YA/O (387 ng/mL); XA/O (110 ng/mL) and O/O (40 ng/mL).
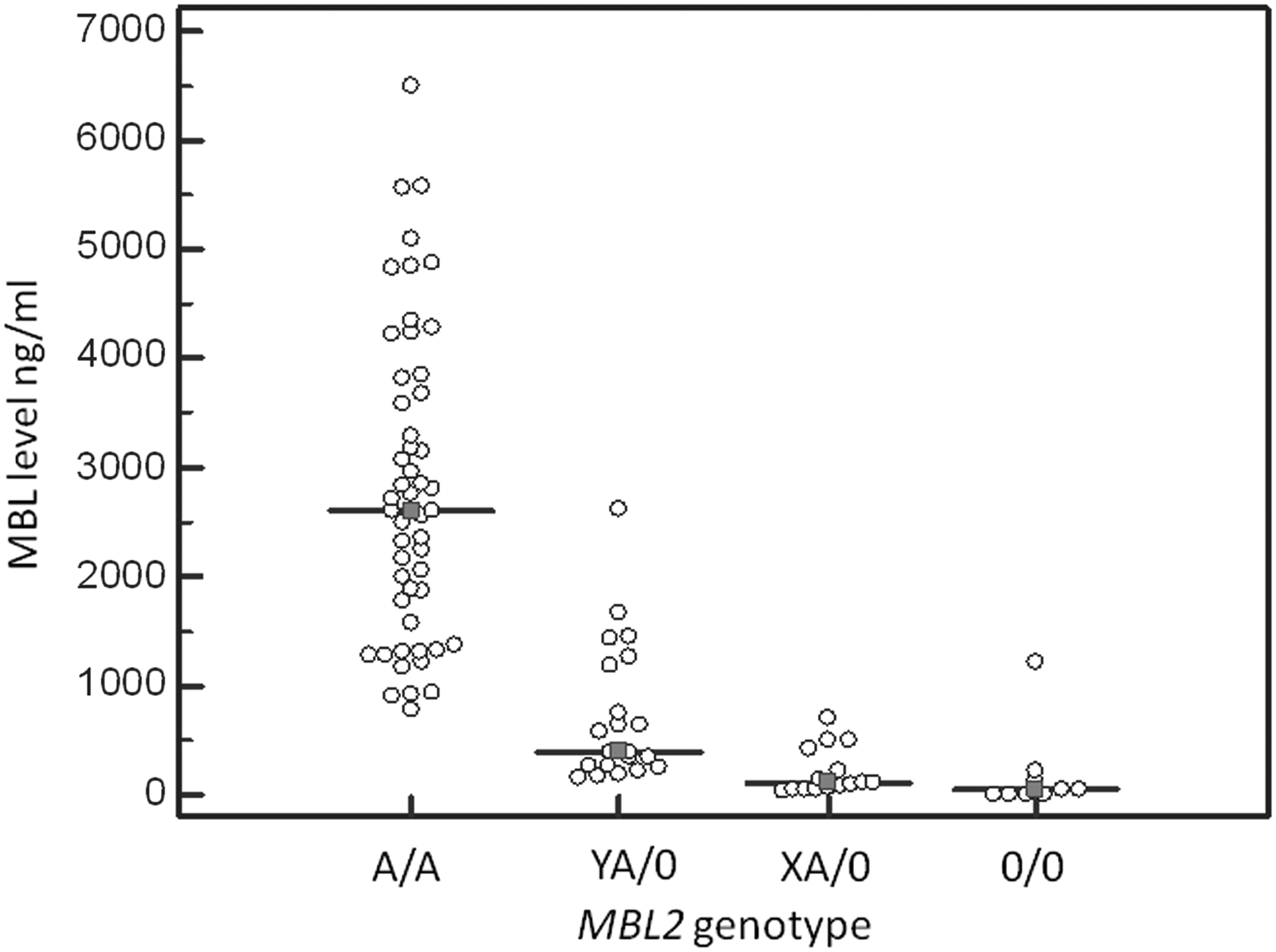
Distribution of MBL serum levels in the study cohort according to MBL2 genotypes.
MBL, mannose-binding lectin; A, wild-type allele; O, group of variant alleles; X/Y, promoter polymorphisms with low/high MBL expression, respectively.
The MBL-deficient O/O group and the MBL-sufficient groups (A/A and A/O) received similar annual courses of antibiotics, with means (range) of 2.1 (0–12) versus 3.9 (0–48) courses/year, respectively (P>0.05). They also had similar lung function measures (z-score), with mean (95% CI) forced expiratory flow in 1 second (FEV1) values of −0.38 (−2.32 to 1.6) versus −1.17 (−1.7 to −0.62); mean forced vital capacity (FVC) values of 0.35 (−1.66 to 2.4) versus −0.49 (−1.05 to 0.06); and mean sRaw values of 0.64 (−4.0 to 5.3) versus 1.3 (0.4 to 2.2) (P>0.05), respectively. The proportion of children with abnormal lung function (z-score <−1.96) in the MBL-deficient group was higher than the MBL-sufficient groups, but not significantly different (33% versus 21%, respectively; P=0.8). Finally, the mean BMIs at referral to our center were similar between the deficient and sufficient MBL groups (16.9 versus 16.7, respectively). However, the BMIs increased nonsignificantly to 18.5 and 16.9, respectively, according to the latest available measurement.
Chest X-rays and/or HRCT images were available for all children. The proportion of children studied with HRCT (33%) compared to children studied exclusively with chest X-ray was similar across the 4 MBL2 genotypes and number of received antibiotic courses. However, the HRCT group had a significantly more impaired mean (95% CI) lung function, z-score—FEV1 of 2.04 (−2.80 to 1.31) versus −0.27 (−0.83 to −0.30), FVC of −1.26 (−1.94 to −0.59) versus 0.31 (−0.40 to 1.04), and sRaw of 4.2 (2.3 to 6.5) versus 1.9 (0.7 to 3.1). No radiological structural lung changes were described in 69% of the entire study cohort, but not surprising, significantly more frequently reported from HRCT (63%) than chest X-ray modality (17%) (P<0.0001). However, radiological images of the O/O group showed no elevation in the odds ratio of 0.76 (95% CI: 0.21–2.8) for structural lung changes.
We then divided the MBL-deficient genotype group into 3 subgroups (intermediate MBL, YA/O; severely reduced MBL, XA/O; and no functional MBL, O/O). Mean (range) annual courses of antibiotics were similar: A/A=4.3 (0–48), YA/O=3.5 (0–12), XA/O=3.3 (0–16), and O/O=2.1 (0–12). However, a nonsignificant trend of increased proportion of children having radiological structural changes was seen. In both the O/O and XA/O group, ∼60% had radiological changes compared to only 33% and 26% in the A/A and YA/O group, respectively. The most severe group (O/O and XA/O) showed again no elevated odds ratio of 0.70 (95% CI: 0.28–1.7), Otherwise, we found no significant differences among the different groups for any other variables studied.
Discussion
This retrospective study assessed whether MBL deficiency could serve as a single factor to explain the differences in pulmonary morbidity in a large, heterogeneous group of children with recurrent pulmonary infections of unknown pathogenesis. We found no differences between the MBL-deficient O/O genotype and the other MBL2 genotypes. The 2 groups showed similar use of antibiotics, BMI, lung function, and radiological structural changes. We also found no differences among the other MBL2 subtypes with less severe deficiencies. To our knowledge, this specific issue has not been previously addressed in a pediatric cohort.
In 2001, Koch et al. 11 performed a prospective study and found a significant, 2-fold increase in the relative risk for acute respiratory tract infection in a group of MBL-insufficient children compared to MBL-sufficient children. The risk was restricted to young children, aged 6 to 17 months; this suggested that children were particularly vulnerable to infections when depleted of maternal antibodies. However, results from other studies indicated that MBL might act like an innate immune response at any age before the production of specific antibodies. 13 Some studies suggested that the risk conferred by MBL deficiency persisted throughout childhood.21,22 In contrast, Ruskamp et al. 23 did not find that MBL2 polymorphisms contributed to the risk of respiratory tract infections. They conducted a study based on questionnaires that prospectively collected data on 987 Dutch children, during the first 4 years of life. Our study differs from the previous few studies in children, since the age span is significantly wider and since we focused on the overall pulmonary morbidity and not solely on the frequency of pulmonary infections as endpoints.
In the present study, we excluded children with an established diagnosis of chronic lung disease, humoral or cellular immune deficiency. Several studies, mainly in adults, have indicated that MBL deficiency might predispose to increased pulmonary morbidity in the presence of other existing chronic lung diseases, like CF 24 or well-established humoral or cellular immunodeficiency. 25 We chose to exclude children with those conditions, because they could hamper the primary aim of the study, which focused on children without clear causes or predispositions to recurrent pulmonary infections. Instead, we targeted children with unexplained recurrent pulmonary infections, which is a frequent, difficult diagnostic entity in pediatric pulmonary outpatient clinics.
No previous pediatric studies have documented antibiotic use, BMI, lung function, or radiological structural changes. However, we found that MBL status had no significant impact on these measures. Similarly, in adults with non-CF bronchiectasis, Macfarlane et al. 26 could not demonstrate any impact of MBL deficiency on lung function, exacerbation rates, symptoms of breathlessness, or microbiology.
Currently, there is no consensus on the definition of MBL deficiency. Up to 10% of the normal population may be considered MBL deficient. It is beyond the scope of this report to review this complex issue. In addition, also, nongenetic factors like age, hormone status (thyroid and growth hormones), and immune activation (MBL is also an acute-phase protein) can affect the MBL level. 8 Koch et al. 11 suggested that MBL2 genotypes (O/O and XA/O) should be considered MBL deficient when the MBL concentration is <600 ng/mL. However, as illustrated in Fig. 2, an overlap in the MBL level is revealed between the MBL2 genotypes, including obvious outliers. Hence, we mainly divided the cohort based on their MBL2 genotype and not the actual MBL level. In the primary analysis of this study, we then only considered the O/O genotype to be fully MBL deficient, to facilitate the detection of a difference between the groups. Nevertheless, we found no significant differences. In a post hoc analysis of the other MBL subgroups with milder deficiencies, the overall results did not change.
Limitations
The main limitations of our study were the retrospective design, and the highly heterogeneous group of children that spanned a broad age range. Also, the threshold for referral to a tertiary pulmonary center may have varied. Moreover, because the causes of recurrent airway infections were unknown, a wide variety of conditions could have obscured differences between the subgroups. For example, ficolins 27 and pentraxins 28 have recently been shown to be an important part of the innate immune system and might be involved concerning recurrent pulmonary infections. Another limitation was that our data on antibiotic use were restricted to electronic prescriptions from the hospital; thus, we may have underestimated antibiotic use, because we did not include the data from general practitioners. However, the patients in this study were primarily monitored and treated at the discretion of physicians at our single center; therefore, we assumed that underestimations would be limited, and any bias on this issue would be equally distributed throughout the cohort.
This study may have been improved by including an unselected control group, due to the relatively high frequency of MBL deficiency in the general population. Furthermore, when a patient is referred to the hospital, the increased attention and treatment they receive could change the natural history of MBL deficiency; however, we assumed that a no alternate clinical approaches were taken based on the MBL status.
The MBL O/O subgroup was overrepresented in our cohort. However, any significant impact from this would have favored the opposite results. We assumed that, despite the statistical uncertainty due to the small sample size, the most severe cases were referred to the hospital, but this should have enhanced any statistically significant differences in lung function or lung damage between groups. It could be argued that HRCT was used in cases considered more severe as the lung function was more impaired in children examined with this modality. However, use of HRCT was similar across the different MBL2 genotypes and use of antibiotics in this HRCT subgroup was similar.
Because MBL deficiency is a congenital genetic entity, the risk of structural lung changes due to infections might increase with the increasing age of the child. Therefore, it was possible that we could have missed future radiological structural changes in this cross-sectional study. However, the most vulnerable period is restricted to the first years of life. Because the median age of our cohort at the time of referral was 3 years (judged by the age of the MBL measurement), we assumed that age would not have hampered our results.
Despite these limitations, we considered the results of this study reliable and important. The reliability rests on the fact that we studied a relatively large group of children, and included their antibiotic use. All variables regarding lung function and radiology were retrieved without the knowledge of the MBL status. The results of this study are relevant because pediatric patients with recurrent respiratory infections are frequent in pulmonary outpatient clinics, and MBL is among the first line tests, despite scanty research to support this test in children. Further prospective studies are needed with birth cohorts, a large random control group, and other immunological measures.
In summary, our data showed that pulmonary morbidity or radiological pulmonary damage was not associated with low-expression MBL2 genotypes in a heterogeneous group of children with recurrent pulmonary infections of unknown cause.
Footnotes
Author's Contributions
K.D. was involved in the conduct of the study, the interpretation of the results as well as the statistical analysis, and writing of the manuscript.
F.B. was involved in the concept and design of the study, the statistical analysis, the interpretation of the results, as well as writing and critical review of the manuscript.
A.T. was involved in the conduct of the study, the interpretation of the results, and writing of the manuscript.
P.G. was involved in the design of the study, the interpretation of the results, as well as critical review of the manuscript.
K.G.N. was involved in the concept and design of the study, interpretation of the results, as well as writing and critical review of the manuscript.
Author Disclosure Statement
None of the authors have any actual or potential conflicts of interest, either personal or financial.