
Abstract
It is unknown whether gastroesophageal reflux disease (GERD) during infancy affects infant bronchiolitis severity or childhood asthma inception. Four hundred thirty-two infants presenting with acute respiratory illness due to bronchiolitis or upper respiratory infection were studied. The primary exposure was the parental report of a previous GERD diagnosis. Outcomes included bronchiolitis severity at initial presentation and childhood asthma diagnosis at age 4. Infants with parentally reported GERD had a higher bronchiolitis severity score (range=0–12, clinically significant difference=0.5), indicating more severe disease, than infants without reported GERD (median 5.5 [interquartile range 3.5–9.0] among those with reported GERD versus 4.0 [1.0–7.0] among those without, P=0.005). This association persisted after adjusting for infant age, race, gender, and secondhand smoke exposure by a propensity score (adjusted odds ratio [OR] 1.99, 95% confidence interval [CI] 1.14–3.46, P=0.02). The parental report of GERD during infancy was not associated with the parental report of asthma diagnosis at age 4. GERD during infancy may contribute to acute respiratory illness severity, but is not associated with asthma diagnosis at age 4. Future prospective studies are needed to confirm these findings.
Introduction
A
Materials and Methods
We studied 432 term, healthy infants (0–12 months) enrolled in the Tennessee Children's Respiratory Initiative presenting with acute respiratory illness (ARI) due to bronchiolitis or upper respiratory infection (URI). The exposure of interest was infant GERD, defined by the parental report of previous diagnosis (answering yes to the question, “Does your child have a history of GERD?”), at study enrollment during acute respiratory illness. The primary outcomes were the infant bronchiolitis severity score (BSS) at clinical presentation and subsequent wheezing and reported asthma at age 4 (“Has your child ever had asthma?”). BSS measures respiratory illness severity and is a 0–12-point validated scale based on retractions, wheezing, respiratory rate, and room air oxygen saturation. 5 A higher score indicates more severe disease, and a difference of 0.5 points is clinically meaningful. BSS was determined based on the most severe values obtained during the initial 24 h of care. Because BSS is a continuous measure describing the spectrum of respiratory disease severity, it was applied to all infants, not just the group (72% of the cohort) diagnosed with bronchiolitis. We compared, by the presence or absence of GERD, BSS at admission and wheezing and reported asthma at age 4; we also examined the independent association of GERD with these outcomes, adjusting for a priori selected covariates of infant age, race, gender, and secondhand smoke (SHS) exposure, using the multivariable proportional odds model for BSS or logistic regression for binary outcomes. To preserve regression power, we applied the propensity adjustment method that combines confounders into one summary score. 6 Written informed consent was obtained from the caregiver of enrolled infants, and the research protocol was approved by the Institutional Review Board of Vanderbilt University.
Results
Among 432 infants with acute respiratory illness, 45 (10.4%) had parentally reported GERD. Infants with reported GERD were more likely to be white, have a parent with allergic rhinitis, and have a history of previous treatment for wheezing. Infants with reported GERD had a slightly lower median gestational age (38 versus 39 weeks, P=0.046) compared with infants without reported GERD. The groups did not differ by age at illness, SHS exposure, or history of parental asthma (Table 1). At study enrollment, a higher percentage of infants with reported GERD had bronchiolitis compared with URI, although this difference was not statistically significant (among infants with reported GERD, 84% had bronchiolitis and 16% had URI; among infants without reported GERD, 71% had bronchiolitis and 29% had URI, P=0.061). Median BSS was 5.5 (interquartile range [IQR] 3.5–9.0), indicating more severe respiratory disease, in infants with reported GERD versus 4.0 (IQR 1.0–7.0) in infants without reported GERD (P=0.005) (Fig. 1A). Increased BSS among infants with reported GERD persisted after adjustment for infant age, race, gender, and SHS using the propensity score (adjusted odds ratio [OR] 1.99, 95% confidence interval [CI] 1.14–3.46, P=0.02). Although not significant in this small sample, 11% (N=5) of infants with reported GERD versus 5% (N=20) without reported GERD needed ICU care (P=0.11).
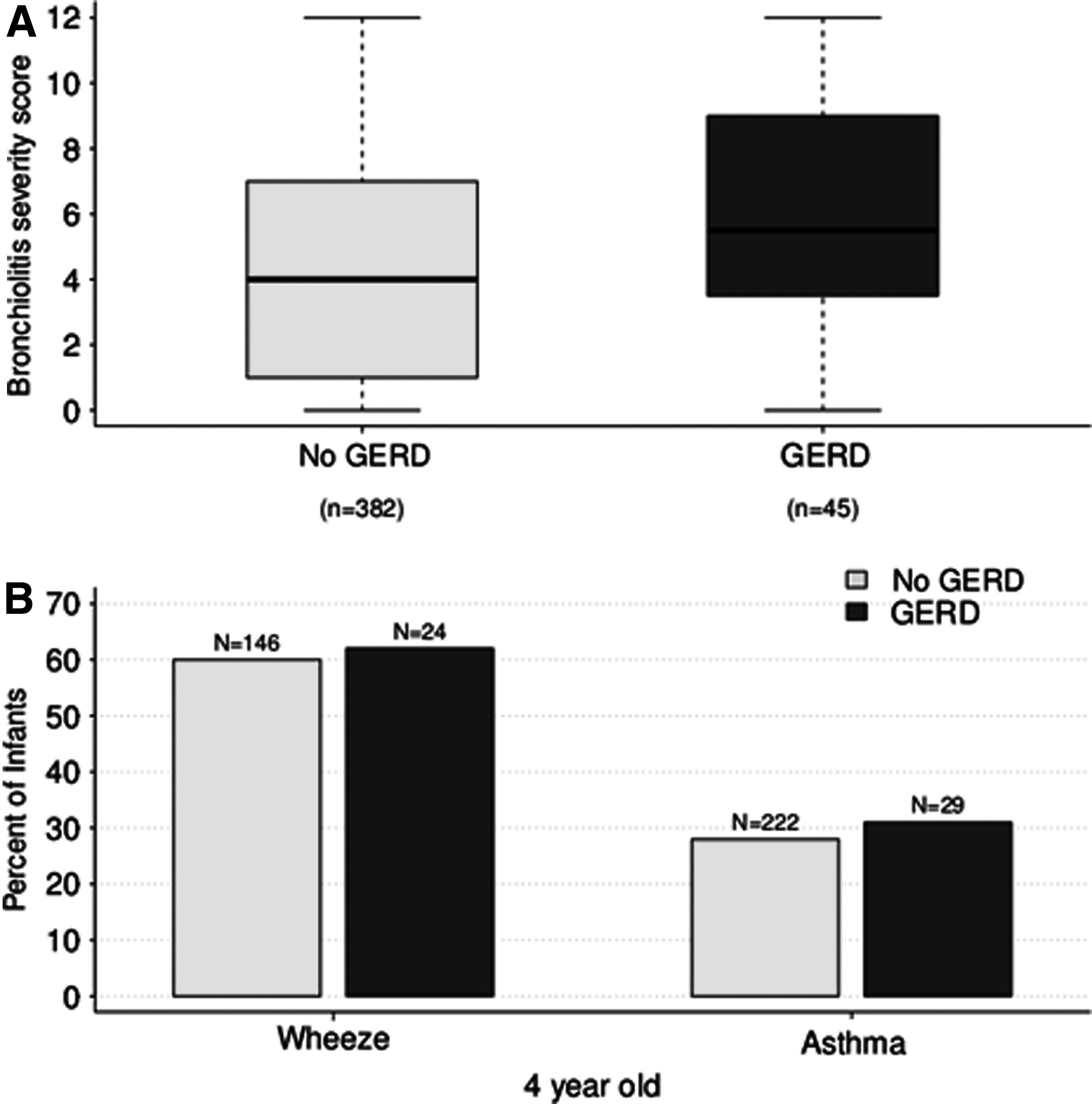
Severity of infant acute respiratory illness and prevalence of wheezing and asthma at age 4.
Unless otherwise stated, all data are presented as N (%).
The chi square test was used for proportions, and the Wilcoxon test for continuous variables.
IQR, interquartile range;
At the 4-year-old study follow-up (completed by 58% of subjects), there was no difference by reported history of infant GERD in parentally reported wheezing in the previous 12 months (among infants whose caregiver reported previous wheezing at any time, 62% of children with reported infant GERD and 60% of those without reported GERD had wheezing in the previous 12 months, P=0.84). There was also no difference in reported asthma diagnosis (31% of those with reported infant GERD versus 28% of those without, P=0.8) (Fig. 1B).
Discussion
Although transient gastroesophageal reflux during admission for bronchiolitis is a risk factor for more severe bronchiolitis among infants without preexisting GERD,1,2 this is the first study to suggest that preexisting GERD is associated with more severe bronchiolitis. However, infants with a history of parentally reported GERD at the time of their acute respiratory illness presentation were not more likely than those without reported GERD to develop asthma by age 4.
Although the presence of GERD and asthma in children is associated, 4 it is unknown whether GERD contributes to asthma development. This study does not support a role for GERD in infancy as a risk factor for subsequent development of asthma in early childhood. It is notable that the association of reported infant GERD with increased bronchiolitis severity does not translate into increased asthma at age 4, since increasingly severe bronchiolitis exerts a dose–response effect on the risk for developing asthma and asthma severity, 7 although this study is underpowered to detect small differences in asthma outcomes.
There are several limitations of this study. First, the cohort was not principally designed to study infant GERD, and the determination of the history of GERD diagnosis was based on the one question asked of caregivers. However, the percentage of infants with reported GERD (10.4%) is quite similar to the prevalence of infant GERD (12.3%) found in a large study that used claims data. 8 Additionally, GERD was only assessed during infancy, and so it is unclear if GERD persisted throughout early childhood. Finally, since the history of treatment for wheezing before study enrollment was higher in the group with reported GERD, it is possible that wheezing might have led to increased GERD recognition (ie, respiratory symptoms may have influenced a provider to diagnose GERD) or that wheezing might have directly contributed to GERD etiology. However, we decided that adjusting for previous wheezing did not make biological sense, because GERD likely impacted respiratory symptoms in affected infants during previous respiratory illnesses, and not just at the time of study enrollment. A related issue is that it is possible that parents of sicker children (ie, those with higher BSS at study presentation) may be more likely to recall a past GERD diagnosis, but illness severity at presentation was based on an objective severity score that was not made available to parents. Despite these limitations, this study, asking a novel question, is the first to suggest a link between early life GERD and bronchiolitis severity, and is of interest as a hypothesis-generating study to encourage further investigation into potential strategies to lessen the morbidity of acute infant bronchiolitis.
One intriguing implication of this study is that, since infants with a report of pre-existing GERD had more severe bronchiolitis, treating GERD during bronchiolitis admissions might result in improved bronchiolitis outcomes. A previous investigation using barium swallow studies showed that thickening feedings eliminated aspiration among a group of infants with R.S.V. bronchiolitis. 9 Future studies, utilizing a more rigorous diagnosis of GERD, could examine whether infants with a history of pre-existing GERD might benefit from treatments for GERD during bronchiolitis admission, since there are currently no effective treatment strategies for bronchiolitis other than supportive care.
Footnotes
Acknowledgment
T.V.H. received support from the Thrasher Research Fund; NIH K24 AI 077930; NIH UL1 RR024975; NIH U19 AI 095227. KNC received support from NIH K01 AI070808.
Author's Contributions
Robert S. Valet MD: study design, data interpretation, and drafting/editing of the manuscript.
Kecia N. Carroll MD, MPH: study design, data interpretation, and editing of the manuscript.
Tebeb Gebretsadik MPH: study design, data analysis/interpretation, and editing/drafting of the manuscript.
Patricia A. Minton RN: study design, acquisition of data, and editing of the manuscript.
Kimberly B. Woodward RN, BSN: study design, acquisition of data, and editing of the manuscript.
Zhouwen Liu MS: data management, data analysis, and editing of the manuscript.
Tina V. Hartert MD, MPH: study design, data analysis/interpretation, editing/drafting of the manuscript, and study funding.
Author Disclosure Statement
No conflicts of interest to disclose.