
Abstract
Chronic eosinophilic pneumonia (CEP) is a rare lung disease and is especially uncommon in children. It presents with subacute respiratory symptoms of hypoxemia and dyspnea, peripheral infiltrates on imaging, and eosinophilia. However, it can be difficult to diagnose, as there is no strict diagnosis criteria and the clinical findings may be very nonspecific. In this case report, we describe a 14-year-old female with an unusual presentation of asymptomatic bronchiectasis, and the role of surgical lung biopsy in the diagnosis of CEP when no peripheral or alveolar eosinophilia is seen. It suggests that perhaps bronchiectasis can also be an unusual presenting sign of CEP and that there may be more asymptomatic cases of CEP with the true incidence being underreported, especially in the pediatric population.
Introduction
C
In CEP, there is no strict diagnostic criterion, with a diagnosis being based solely on clinical findings. These include respiratory symptoms of more than 2 weeks' duration, alveolar and/or blood eosinophilia, pulmonary infiltrates with bilateral peripheral predominance, and exclusion of other known causes of eosinophilic lung disease.4,5,6 The histology of CEP shows eosinophilic and lymphocytic infiltration into the alveolar septa and intra-alveolar lumina, and occasionally can show giant cells, increased macrophages, interstitial edema, and fibrin deposition. 2 Treatment consists of oral corticosteroids, but there is no standard treatment of dose or duration. General recommendations are to start initial prednisone therapy 0.5–1 mg/kg/day with a gradual taper for 6–12 months, but relapses in the long term have been seen in up to 50% of cases. 4
Case Report
A 14-year-old previously healthy female presented to an emergency department with history of intermittent left-sided abdominal pain for 4 months. She had an abdominal computed tomography (CT) scan done that showed a left ovarian cyst. Incidental lung findings were seen on the CT of a right lower lung pulmonary nodule, scarring, and bronchiectasis in the lower lobes. She had a normal complete blood count and comprehensive metabolic panel. She was admitted to the hospital for pain management and upon discharge was referred to pulmonology for further outpatient evaluation of the lung findings. She was evaluated for common causes of bronchiectasis. Her medical history was negative for any past condition, and she had no respiratory symptoms. She denied history of frequent infections, asthma, foreign travel, smoking, or positive purified protein derivative (PPD) test. Her family history was also negative for lung disease. Physical exam was unremarkable, with a body mass index in the 52nd percentile, a normal symmetric lung exam, and no signs of digital clubbing or edema.
Her sweat chloride tests were normal (13/13 mmol/L), and CFTR gene sequencing failed to identify any known pathogenic mutations. Ciliary biopsy was insufficient for ultrastructural evaluation of cilia morphology. Alpha-1 antitrysin level was normal. A high-resolution CT chest scan was done, and a cystic fibrosis score of 10 out of 27 7 was given for a significant component of diffuse bronchiectasis, predominantly in bilateral posterior basilar peripheral lungs and the posterior right upper lobe. No bronchial wall thickening, sacculations, abscesses, bullae, or emphysema were seen (Figs. 1 and 2). A CT scan of the sinuses revealed a normal study. Further testing was done for rheumatologic and autoimmune diseases, as well as immunodeficiency disorders. All lab tests returned normal, except for elevated IgE (360 IU/mL). Quantitative immunoglobulins and quantitative T-cell subsets panel were normal. HIV antibody was nonreactive. Her erythrocyte sedimentation rate, C-reactive protein, antinuclear antibody (ANA), antineutrophil cytoplasmic antibodies (ANCA), double-stranded DNA, antiglomerular basement membrane (GBM) antibodies, complement, and rheumatoid factors were all in normal range.
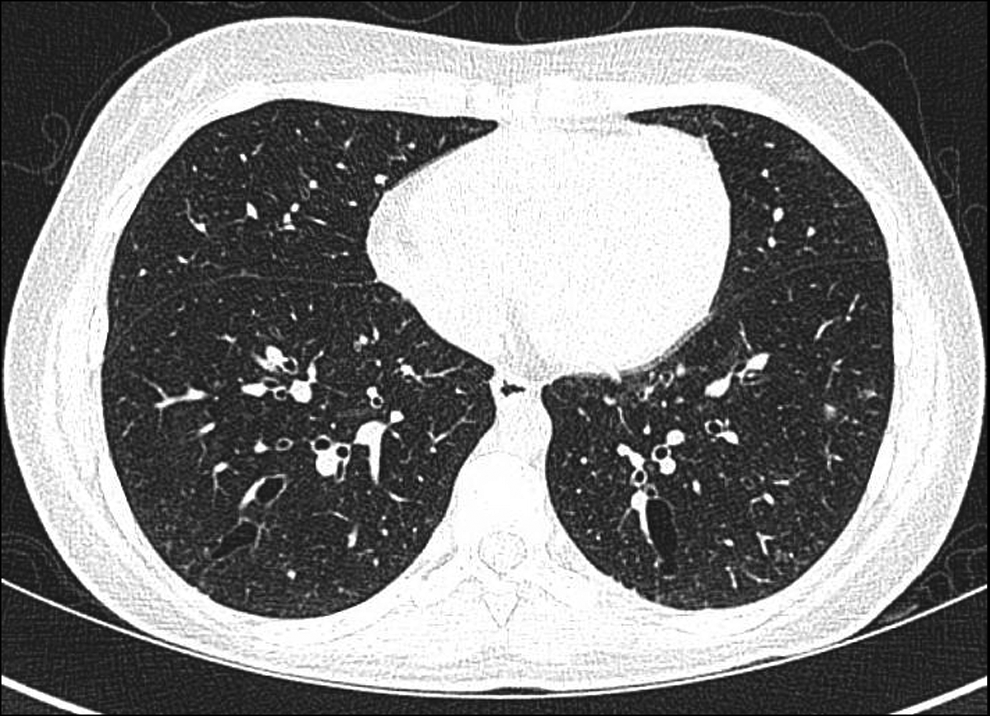
Axial view of the bronchiectasis in the lower lobes seen on high resolution computed tomography (HRCT) scan.
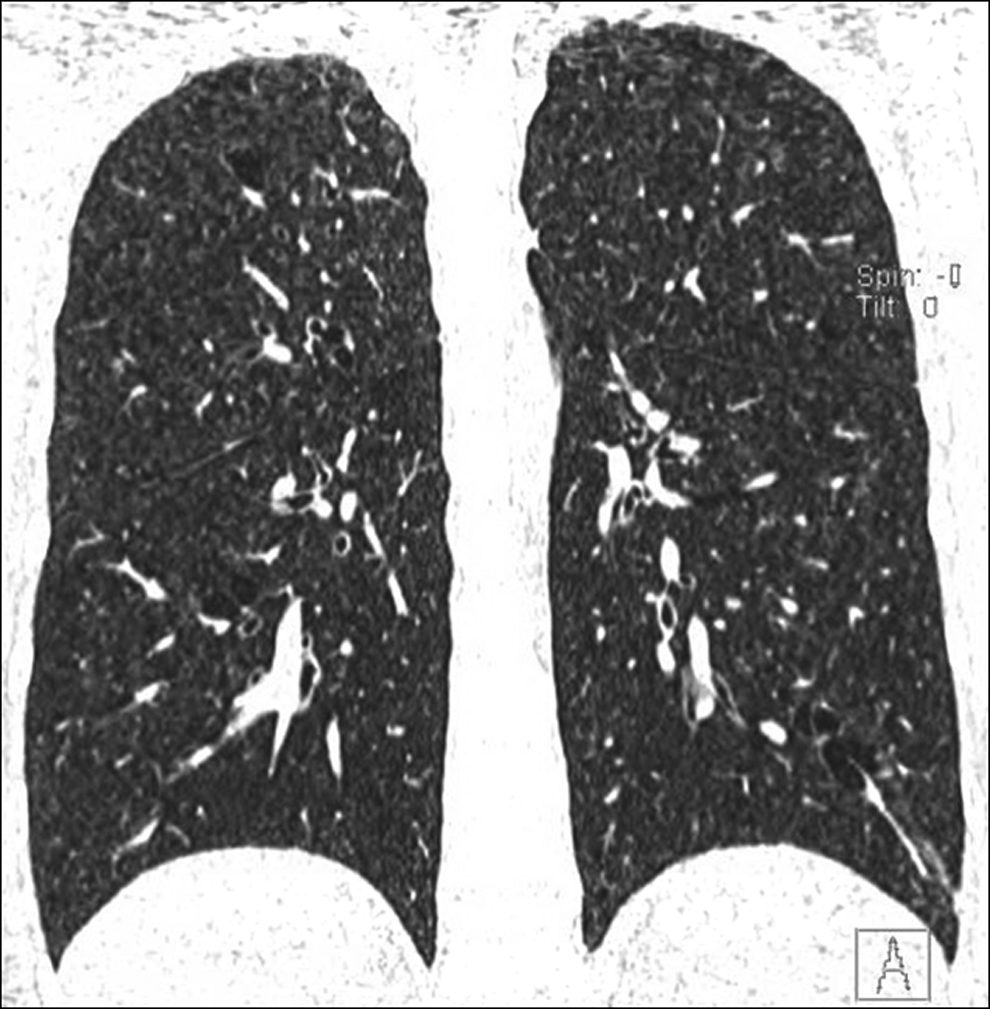
Coronal view of bronchiectasis and scattered small foci of airspace consolidation on HRCT.
Radioallergosorbent allergy testing (RAST) was positive for dust mites and cat dander but negative for A. fumigatus. Aspergillus precipitins was also negative. She had a negative Aspergillus skin prick test. The patient's stool was examined and was negative for ova and parasites. Full pulmonary function testing including lung volumes and diffusing capacity for carbon monoxide (DLCO) was performed initially, and then serial spirometries were monitored at each pulmonology visit, and they were all within normal limits. She had also been asymptomatic and afebrile with normal lung exams during each visit as well. She was started on empiric albuterol with high-frequency chest-wall oscillation vest therapy and azithromycin 500 mg daily three times a week for anti-inflammatory effects. Four months after her initial presentation, a bronchoscopy with bronchoalveolar lavage (BAL) was done. Findings showed normal anatomy, and BAL fluid showed RBC 629 cells/μL, WBC 71 cells/μL; differential showed neutrophils 48%, lymphocytes 34%, monocytes 10%, and eosinophils 8%. BAL culture grew A. versicolor and was negative for acid fast bacilli/bacterial/viral pathogens and mycoplasma. Aspergillus growth was believed to be contaminant.
Due to negative testing thus far, a right thoracoscopic lung biopsy was performed. The posterior aspect of the right upper lobe, which appeared to be the most consistent with the bronchiectatic portion of the lung, was biopsied and sent for pathologic evaluation at our institution and to Mayo Clinic in Arizona. Histology revealed bronchiolectasis and mucus stasis associated with focal, acute, and organizing pneumonia with prominent eosinophils consistent with chronic eosinophilic pneumonia (Fig. 3). There were also patchy areas of increased airspace macrophages associated with rare multinucleated giant cells (Fig. 4). Histochemical stains and cultures for fungi, acid-fast organisms, and bacteria showed no pathologic organisms.
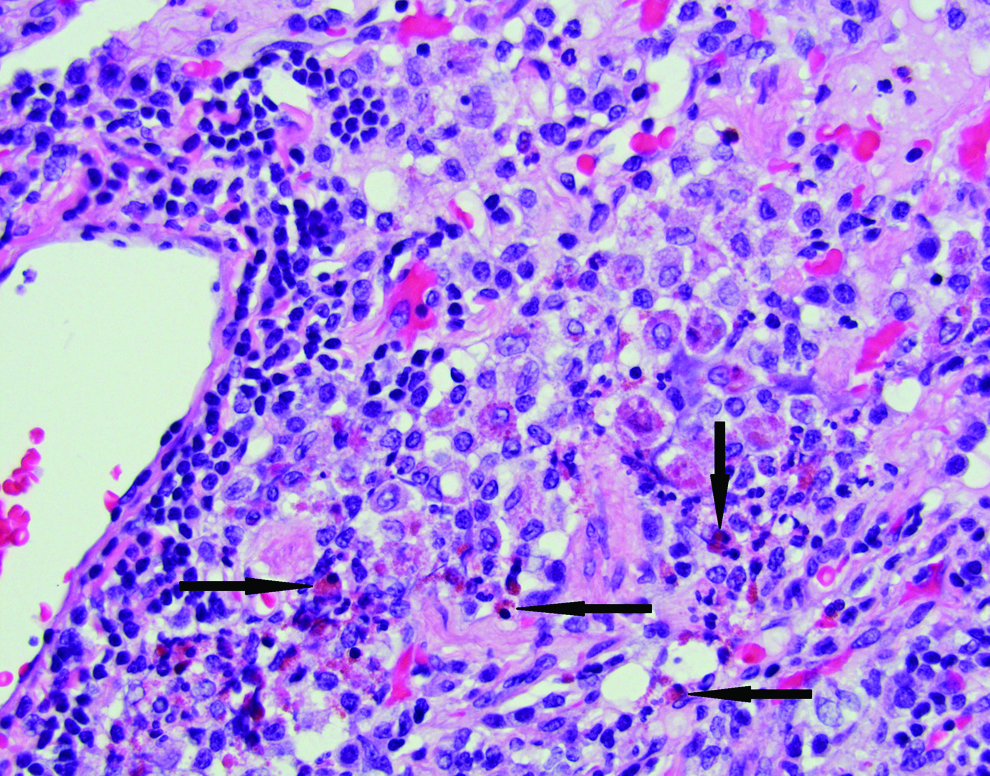
Chronic bronchiolitis with bronchiolectasis and mucus stasis associated with focal, acute, and organizing pneumonia with prominent eosinophils (arrows) consistent with chronic eosinophilic pneumonia. Color images available online at www.liebertpub.com/ped
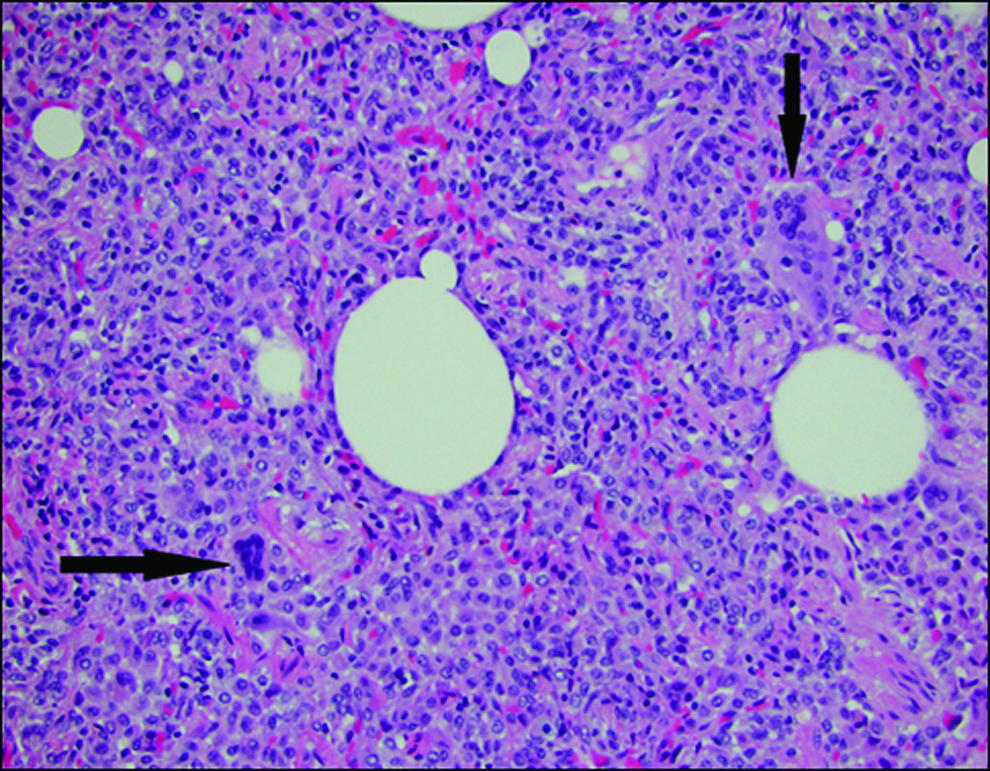
Patchy areas of increased airspace macrophages associated with rare multinucleated giant cells (arrows), which can be seen with chronic eosinophilic pneumonia. Color images available online at www.liebertpub.com/ped
After the lung biopsy, the patient was started on inhaled beclometasone dipropionate and prednisone while continuing on albuterol and vest therapy. Azithromycin treatment was discontinued at that time, and she was treated with prednisone for 6 months. A repeat high-resolution CT scan showed improvement in the severity of her bronchiectasis.
Discussion
CEP can be difficult to diagnose and can present in various ways. In this case, our patient was asymptomatic and was found to have incidental bronchiectasis discovered on CT abdomen for abdominal pain. Due to a negative evaluation for the common causes of both focal and generalized bronchiectasis, she underwent a surgical biopsy. Only through histological evaluation of her bronchiectasis was the unexpected diagnosis of CEP.
CEP is one of the eosinophilic lung diseases that feature increased number of eosinophils in the pulmonary parenchyma, and the cause of CEP is idiopathic. Differential diagnosis of eosinophilic pulmonary infiltrates includes Churg–Strauss syndrome (CSS), allergic bronchopulmonary aspergillosis (ABPA), acute eosinophilic pneumonia (AEP), parasitic, bacterial, viral and fungal infections, toxin exposure, and drug reactions. CSS can present with pulmonary symptoms similar to CEP with dyspnea, cough, and pulmonary infiltrates with eosinophilia. CSS also has many more extrathoracic findings such as asthma, sinus abnormalities, eosinophilia >10% of total white blood cell (WBC) count, migratory or transient pulmonary opacities, neuropathy, and extravascular eosinophils on biopsy.4,6,8 On CT imaging CSS has features of bilateral nonsegmental consolidation or reticulonodular opacities, subpleural ground-glass opacities, interlobular septal thickenings, and bronchial wall thickening. Hyperinflation, pleural effusions, or mediastinal lympadenopathy are less commonly seen. 6 Our patient did not have any of the above lung findings on imaging, and she had a thorough rheumatologic workup that returned negative. ABPA can be diagnosed by positive immediate skin test for Aspergillus antigens, increased serum IgE (>417 IU/mL or >1,000 ng/mL), elevated serum IgE/IgG to A. fumigatus, positive Aspergillus precipitins, presence of asthma or cystic fibrosis, and peripheral blood eosinophilia with pulmonary infiltrates. 9 Radiographic findings can range from transient pulmonary opacities to plugging of airways with distal mucoid impaction in the early stages of disease to central bronchiectasis and pulmonary fibrosis in the later stages. 6 Our patient had IgE only slightly elevated at 360 IU/mL with negative Aspergillus skin test and negative Aspergillus IgG/IgE antibodies.
She was never febrile or had any exposure history to indicate infection. Lung biopsy also did not reveal infection. The A. versicolor that grew from the bronchoalveolar lavage was believed to be contaminant because the biopsy did not grow A. versicolor. The lung biopsy specimen was a good sample, as it was taken from the area that grossly appeared the most bronchiectatic. A. vesicolor is also much more common to be the cause of cutaneous not pulmonary infection. In addition, negative history and normal immunity (normal quantitative immunoglobulins and quantitative T-cell panel) make invasive Aspergillus infection very unlikely. She did not take any medications to cause a drug-induced pulmonary infiltrates with eosinophilia or present with acute respiratory symptoms to suggest idiopathic AEP.
Common causes of bronchiectasis were also considered in this case, including cystic fibrosis, alpha-1 antitrypsin deficiency, hypersensitivity pneumonitis, immunodeficiency disorders, and rheumatologic and autoimmune diseases. All the tests were negative for these diseases. Primary ciliary dyskinesia (PCD) was excluded in our patient, as her symptoms and signs were not consistent with PCD. Specifically, she did not have chronic otitis media, chronic or recurrent sinusitis, or early respiratory infections. 10
Eighty-six percent of patients with CEP demonstrate peripheral blood eosinophilia. Our patient did not have peripheral eosinophilia with the typical CEP presentation of >1,000/mm3 in the blood. 4 If there is no significant peripheral eosinophilia, then BAL eosinophilia of >25% 8 can aid in confirming the diagnosis. Elevated eosinophil counts are found in BAL fluid 100% of the time, and transbronchial lung biopsies reveal eosinophilic infiltrates in 64% of cases. 11 However, in our unusual patient, she had BAL eosinophilia of only 8%, which was still elevated. 12
Bronchiectasis is not a common finding in patients with CEP, which typically has a radiographic presentation of nonsegmental peripheral airspace consolidation and the “photographic negative shadow of pulmonary edema”4,6 involving mainly the upper lobes on chest X-ray and CT chest scan. Pleural effusion can be seen in <10% of cases, and in later stages of CEP, one can have less common findings of ground-glass opacities, nodules, and reticulation. 6 However, in a study by Furuiye et al., 13 comparing CT chest images of adult patients with CSS versus CEP, their findings described 25 cases of traction bronchiectasis (reflecting organization or fibrosis) as being associated with CEP. In our patient, the bronchiectasis may have formed more due to inflammation of her airways rather than traction bronchiectasis, as there was no fibrosis or sign of lung volume loss seen on CT chest scan or biopsy. Open or thoracoscopic lung biopsy is typically not necessary to diagnose CEP. However, it may be performed to exclude other lung diseases, particularly infections. It was through biopsy that our patient received the unexpected diagnosis of CEP and was started on systemic steroids. The importance of treating her CEP, even if asymptomatic, was to prevent irreversible pulmonary fibrosis.
In conclusion, not all cases of CEP have peripheral eosinophilia in blood or bronchoalveolar lavage as identified in our patient, so there is a role for surgical lung biopsy to assist in diagnosis. Also, bronchiectasis was the most prominent radiological lung finding in our patient, so we suggest adding bronchiectasis as an atypical sign of CEP in children. We raise the question that perhaps there are more cases of asymptomatic CEP presenting as isolated bronchiectasis and that the incidence of CEP in the pediatric population is underreported.
Footnotes
Acknowledgments
Special thanks to Dr. Aaron Sassoon for his contribution to the pathology pictures, and Dr. Henry Tazelaar for his contribution to the pathology report.
Author Disclosure statement
No competing financial interests exist.