
Abstract
Background:
Pneumonitis, pleuritis, and pulmonary interstitial infiltration have been described in patients with juvenile idiopathic arthritis (JIA). However, the pulmonary involvement of JIA is not often clinically apparent. There are few studies based on pulmonary function in children having only a diagnosis of JIA. The aim of the present study is to determine whether children with JIA have airway resistance and flow impairments measured by easily applied interrupter technique.
Method:
We performed interrupter resistance (Rint) measurements in children with JIA and in healthy control subjects who had no respiratory symptoms or diseases.
Results:
Fifty-eight children with the diagnosis of JIA (Mean age=12.5±2.75 years; range 7–17 years) and 33 healthy subjects (Mean age=11.8±2.62 years; range 6–16 years) were included in the study. The mean value of tidal peak flow during expiration measured by the interrupter technique was significantly lower in the JIA study group (0.73±0.11 L/s) compared to the healthy control group (0.79±0.08 L/s; p=0.01). Rint values measured during inspiration (Rintinsp) and during expiration (Rintexp) were higher in the JIA study group (Rintinsp=0.28±0.16 Kpa/L/s; Rintexp=0.30±0.50 Kpa/L/s) compared to the healthy control group (Rintinsp=0.26±0.11 Kpa/L/s; Rintexp=0.23±0.08 Kpa/L/s; p>0.05). There was also a positive correlation between C-reactive protein level and median expiratory interrupter resistance (Rintexp; r=0.50, p=0.005).
Conclusion:
The interrupter technique is a noninvasive and feasible technique and can be used to assess airway abnormalities in children with JIA who cannot successfully complete spirometry.
Introduction
J
Methods
Study population
Fifty-eight children with JIA were recruited consecutively into the study. Information on respiratory symptoms, allergy, eczema, and doctor's diagnosis of any pulmonary diseases, paricularly asthma, were recorded using questionnaires modified from the International Study of Asthma and Allergies in Childhood. Patients and control group subjects with a history of asthma and other pulmonary diseases were excluded 13 because they may confound results. The children in the study group were classified according to International League of Associations for Rheumatology criteria.2,14 Age at onset, history of treatment, disease activity, and disability scores were recorded.
The investigation conforms to the principles outlined in the Declaration of Helsinki. The study was approved by the local ethics committee. Parental permission and child assent were obtained for all study participants.
Disease activity
On the day of evaluation, joint swelling was graded using a validated 4-point scoring system. Swelling is scored as 0=normal, 1=minimal swelling, 2=swelling within joint limits, and 3=swelling exceeds joint limits. 15 Inflammatory disease was described as having active arthritis (swelling, dysfunction, pain) with leukocytosis and/or thrombocytosis and/or elevated C-reactive protein levels and/or elevated erythrocyte sedimentation rates.
Rint measurement procedure
We utilized the protocol published by Merkus et al. for measurement of interrupter resistance in preschool children. 16 All measurements were completed by using identical commercial devices (Micro Lab 4000; Micro Medical Ltd, Gillingham, United Kingdom) by the single and same operator. Flow calibration was achieved before each measurement. Studies were done in a child-friendly environment by a single member of our research team to encourage cooperation to achieve reproducible results. Children were given the opportunity to practice before the actual measurements were recorded. They were instructed to breathe gently through a mouthpiece (2.7 cm diameter) with the nose clipped and the neck extended. The children's anxiety, which could possibly cause abnormal breathing, was reduced with entertainment and talking with them to divert their mind and attention from the procedure. After a period of slow and quiet breathing, the shutter locked at the peak of tidal flow for a period of 100 ms. At least two practical challenges were performed before recording the data. Participants of the procedure were unable to predict the trigger, but they were able to hear the valve shutting. Measurements disrupted by a respiratory pause, crying, or coughing were not recorded during the breathing cycles. Tracings that did not show the timing of the interruption of the flow on the screen, or tracings with a horizontal or declining pressure signal indicating leakage at the mouth, or with an altered ventilation pattern were excluded as well. 17 At least five validated Rint measurements with a coefficient of variation of ≤20% were taken into account for the calculation of the median Rint value of a subject. Rint values were measured in children with the diagnosis of JIA first during expiration (Rintexp) and then during inspiration (Rintinsp). Rint values were also measured in healthy control subjects first during expiration followed by inspiration.
Control group
Thirty-three healthy children were randomly selected from a group of 300 healthy children whose parents were working in our hospital. There was no significant difference between these children (control group) and patients with JIA regarding sex, age, and body mass index, demonstrating that these two groups could be directly compared (Levene test >0.05).
Statistical analysis
The Kolmogorov–Smirnov test was used to test for normal distribution of continuous variables. Data characterized by a normal distribution were expressed as mean values followed by standard deviation. Student's t-test (normal distribution) was used to compare the two groups. Multivariate regression analysis was used in a stepwise descending method from prognostic factors with significance <0.1 at univariable analysis. Results are given as odds ratios (95% confidence interval [CI]), and p<0.05 was considered statistically significant.
Results
Fifty-eight consecutive children with a diagnosis of JIA were included in the study. The mean age of the patients was 12.5±2.75 years, and 37 of them were female. Twenty-seven patients were treated with weekly oral methotrexate (weekly dose 10–15 mg/m2). The study population and the control group had normal respiratory rates and oxygen saturation on room air. Clinical features, characteristics, and Rint measurements of the study population and controls are listed in Table 1.
Bold p value indicates statistical significance.
Tidal peak flow measured by interrupter technique.
Data are presented as mean±standard deviation. Significance was calculated by using Student's t-test: p<0.05.
JIA, juvenile idiopathic arthritis, Rint, interrupter resistance; Rintinsp, inspiratory interrupter resistance; Rintexp, expiratory interrupter resistance.
All of the children with JIA and all of the control subjects were able to provide Rint measurements. The mean value of tidal peak flow during expiration measured by interrupter technique was significantly lower in the JIA group (0.73±0.11 L/s) than in the healthy control subjects (0.79±0.08 L/s; p=0.01). Rint values measured during inspiration (Rintinsp) and during expiration (Rintexp) were higher in JIA study group (Rintinsp=0.28±0.16 Kpa/L/s; Rintexp=0.30±0.50 Kpa/L/s) compared to the healthy control group (Rintinsp=0.26±0.11 Kpa/L/s; Rintexp=0.23±0.08 Kpa/L/s; p>0.05). There was also a positive correlation between C-reactive protein level and median expiratory interrupter resistance (Rintexp; r=0.50, p=0.005; Fig. 1). In multivariate analysis, a significant association was found between JIA disease activity and median expiratory interrupter resistance (Table 2).
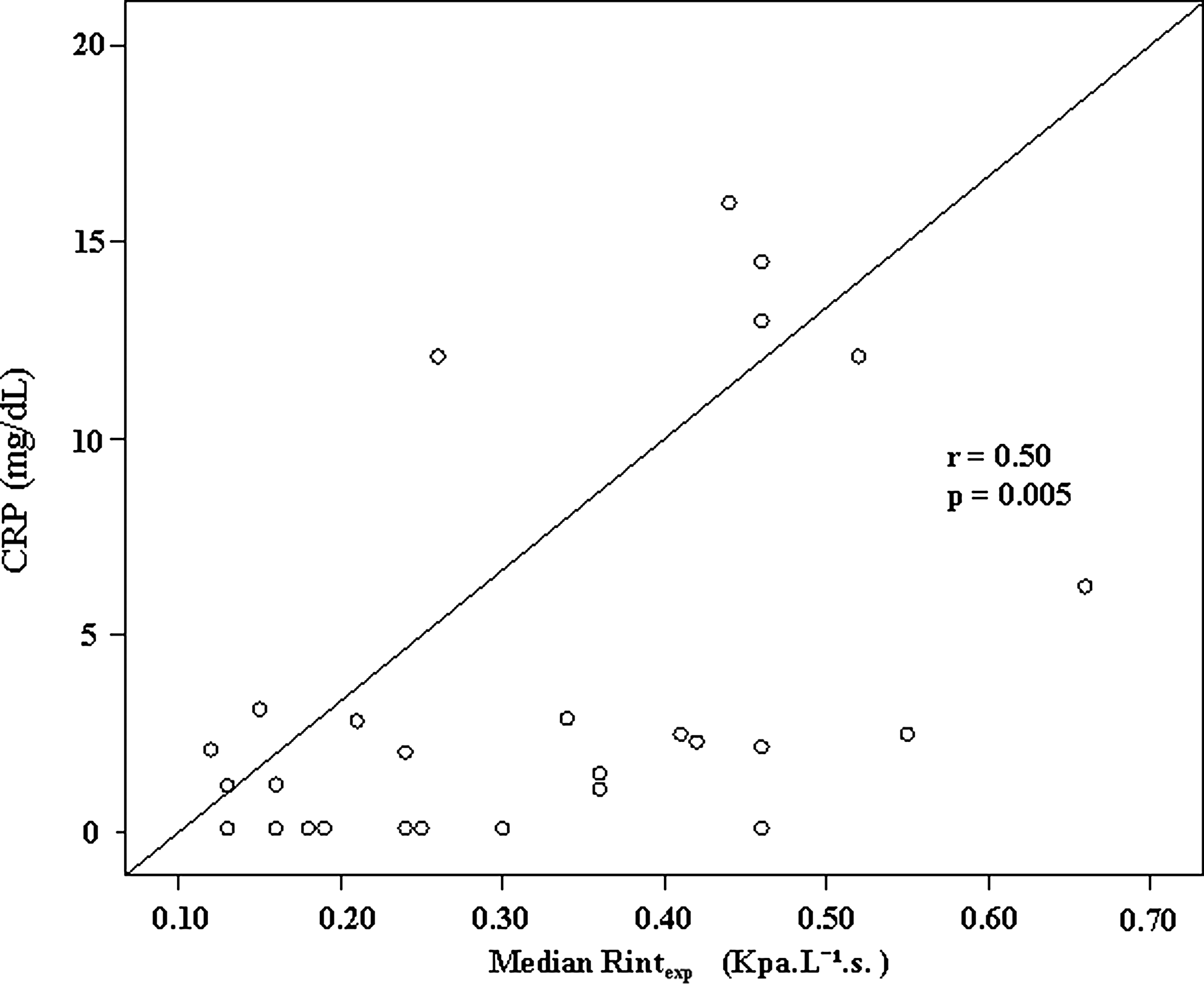
Correlation between median expiratory interrupter resistance (Rintexp) and C-reactive protein (CRP) levels (n=27).
Bold p value indicates statistical significance.
HR, hazard ratio; CRP, C-reactive protein; ESR, erytrocytes sedimentation rate; CI, confidence interval.
Discussion
In this study, we demonstrated significant impairment in tidal peak flow measurements during expiration in children with JIA as measured by the interrupter technique. Recording tidal breathing without interference is important because it necessitates minimal cooperation, and may reflect “real life” with the help of frequent measurements, even during acute respiratory conditions. 18 Tidal breathing includes significant physiologic information pertaining to a number of processes related to both respiratory control and pulmonary mechanical function. It is also associated with natural physiologic state of undisturbed regular breathing.19,20 Early respiratory involvement in children with JIA is often not clinically apparent. Techniques to identify respiratory dysfunction in children before they are developmentally able to perform spirometry successfully are important. Correlation between C-reactive protein level and median expiratory interrupter resistance (Rintexp) also has particular importance. CRP as a disease activity marker has an association with the airway resistance at expiratory phase of Rint measurements. The upper airways contribute to most airflow resistance of the respiratory system. Younger children could have higher Rint values physiologically, even with a low CRP. Therefore, the wide age range may be an important issue when comparing Rint values in this group of patients. This problem can be solved by using Z-scores. International references values are now available for the 3–13 years age range. 21 Temporomandibular joint involvement in JIA may be asymptomatic. 22 This may account in part for the higher Rintexp measurements and lower tidal peak flow measurements during expiration. Significant impairment has been reported in respiratory muscle strength in children with JIA, severe enough to cause mild lung function abnormalities and an increase in disability. 10 The preclinical muscle strength impairment may be a cause of respiratory muscle fatigue with a reduced ability to exhale to residual volume, and may account for the decreased tidal peak flow measurements during expiration in children with JIA. Although tidal peak inspiratory flow is also decreased in children with JIA compared to the controls, it is not statistically significant, since no muscle activity is normally expected during expiration. It is the opinion of these authors that the most likely explanation for this finding might be that children with JIA have a stiffer lung with lower compliance than controls. Generally, in childhood connective tissue disorders, clinically apparent lung involvement is rare, particularly in JIA. 7 Functional lung impairment has been shown, even in the absence of radiographic abnormalities in childhood connective tissue disorders. 7 Rint measurements may have prognostic significance for the detection of early involvement of the respiratory system in patients with JIA. There are few studies, all of small size, of pulmonary involvement in patients with JIA.8,10 One of the most important limitations to investigations of pulmonary involvement and pulmonary functions in children with JIA are the difficulties with the effort-dependent spirometric measurements in children. However, the ability to assess pulmonary function is important for evaluation of a child with respiratory diseases and helpful in establishing a diagnosis. 23 It is also important for assessing the severity of impairment and for providing effective care during the follow-up period. Rint measurement may provide insight into the early changes in the airways and respiratory function in children with JIA.
The interrupter technique is a noninvasive and easily applied technique for estimating airflow resistance. This technique requires only quiet breathing, and is based on measurements of tidal airflow and mouth pressure during the interruption.24,25 Koopman et al. studied interrupter resistance in methacholine challenge testing in children, and concluded that the use of Rint to diagnose bronchial hyperresponsiveness in individual patients seems limited with low sensitivity and specificity. 26 On the other hand, the accuracy of the Rint method was reported as reasonable, with a sensitivity of 66% and a specificity of 82% cystic fibrosis patients. 27 Rint measurements correlate closely with spirometric values.28,29 In the present study, it was possible to achieve reliable Rint measurements in all of the children, both in the JIA study group and in the healthy control group.
Previous studies of lung function in children with JIA have produced conflicting results.7–11,30 Some studies reported a decrease in pulmonary function tests including maximum midexpiratory flow, peak expiratory flow, forced vital capacity, and carbon monoxide diffusing capacity, which they attributed to inflammatory changes of the peripheral bronchial airways due to the disease process.7–10 Evidence from these studies supports the presence of an early onset of flow limitation, particularly at low lung volumes without any significant large airway obstruction in children with JIA. 9 Others found no impairment in lung function in children with JIA.11,30 However, there was consensus that there was no relationship between methotrexate therapy and lung function parameters in children with JIA.9–11,30 Our study agreed with these results. No relationship was identified between airway resistance measurements by Rint technique and methotrexate therapy in children with JIA. Notably, up to 25% of affected children in these studies were unable to perform pulmonary function testing reliably.7,9 This is an important external validity problem in terms of pulmonary function test studies in young children. The variable results of pulmonary function tests in children with JIA may potentially be due to children's inabilty to carry out these effort-dependent routine pulmonary function tests, particularly the forced expiratory maneuvers. On the other hand, Rint measurement is an easily applied technique requiring slow and quiet breathing with relatively good compliance by children. The present study showed that we were able to complete all the Rint measurements in both the JIA and the healthy control groups. The completion of all the Rint measurements in both the JIA and the healthy control groups may provide better external validity for future JIA studies without any dropped out measurements.
In addition, from the measurements of maximal expiratory flows at low lung volumes in routine pulmonary function tests, it was shown that sex may influence the growth and dynamics of airways. Girls have been shown to have higher flows than boys during both early and late childhood periods. 31 Because maximal expiratory flows at low lung volumes are expected to reflect geometry of small airways, girls may have larger peripheral airways than boys. The central airways supply most of the resistance to airflow.31,32 There are also conflicting reports about the effect of sex on resistance to airflow in routine measurements of pulmonary function tests. For example, in one study, there were higher values in boys than in girls. 33 We considered that our findings of decreased maximal expiratory flows at low lung volumes in children with JIA might also have been influenced by gender. However, previous studies do not support a gender difference in Rint measurements.12,34,35 Rint values correlated well with other small airway parameters. 36 Therefore, studying pulmonary function impairment with Rint measurements in children with JIA may provide an advantage over routine pulmonary function tests in which children have difficulties with these effort-dependent procedures.
There are several limitations to this study. First, we did not measure respiratory muscle strength of the children with JIA for the possible explanation of the lower Rint values. Second, we did not investigate further whether these patients with JIA had temporomandibular joint involvement, although they were clinically asymptomatic. Third, small sample size may limit generalizability.
In conclusion, the mean value of tidal peak flow during expiration measured by interrupter read was significantly decreased in patients with JIA compared to healthy controls. Median expiratory interrupter resistance (Rintexp) significantly correlates with CRP level of patients with JIA. Rint measurements have an important potential for use over a wide age range. Rint testing may provide a suitable alternate method for assessing respiratory dysfunction in children who are unable to perform acceptable spirometry and lung volume maneuvers successfully.
Footnotes
Acknowledgments
The authors thank Prof. R.W. Guillery from Oxford University for the English correction of the manuscript.
Author Disclosure Statement
No competing financial interests exist.