
Abstract
Allergic rhinitis (AR) is a risk factor for the development of asthma, and if poorly controlled, it may exacerbate asthma. We sought to describe AR symptoms and treatment in a larger study about asthma, sleep, and school performance. We examined the proportion (1) who met criteria for AR in an urban sample of school children with persistent asthma symptoms, (2) whose caregivers stated that they were not told of their child's allergies, (3) who had AR but were not treated or were undertreated for the disease, as well as (4) caregivers and healthcare providers' perceptions of the child's allergy status compared with study assessment, and (5) associations between self-report of asthma and AR control over a 4-week monitoring period. One hundred sixty-six children with persistent asthma participated in a clinical evaluation of asthma and rhinitis, including allergy testing. Self-report of asthma control and rhinitis control using the Childhood Asthma Control Test (C-ACT) and Rhinitis Control Assessment Test (RCAT) were measured 1 month after the study clinic session. Persistent rhinitis symptoms were reported by 72% of participants; 54% of rhinitis symptoms were moderate in severity, though only 33% of the sample received adequate treatment. AR was newly diagnosed for 53% during the clinic evaluation. Only 15% reported using intranasal steroids. Participants with poorly controlled AR had poorer asthma control compared with those with well-controlled AR. This sample of urban school-aged children with persistent asthma had underdiagnosed and undertreated AR. Healthcare providers and caregivers in urban settings need additional education about the role of allergies in asthma, recognition of AR symptoms, and AR's essential function in the comanagement of asthma. Barriers to linkages with allergy specialists need to be identified.
Introduction
A
Most patients with asthma also have rhinitis, while 10–40% of patients with rhinitis have comorbid asthma. 4 Several mechanisms have been postulated for this close association between upper and lower airway morbidity, including (1) aspiration of inflamed or infected secretions to the lower airway, (2) nasal blockage that leads to mouth breathing cold, dry air increasing allergen entry into the lower airway, (3) systemic absorption of inflammatory mediators in the nasal mucosa, or (4) a nasobronchial reflex.5–8
AR practice guidelines highlight the need for allergy evaluation when rhinitis symptoms are persistent, moderate or severe, or impact quality of life.1,9 Guidelines also recommend the integration of AR treatment in the management of asthma1,4,9–11 and highlight intranasal steroids as the optimal medication class for controlling AR symptoms.1,4
Data presented here are part of a larger study, Project NAPS (Nocturnal Asthma and Performance in School), a multimethod longitudinal study of urban children with asthma investigating links between asthma, rhinitis, sleep, and school performance during one academic year in children at high risk for frequent emergency department (ED) visits and hospitalizations for asthma. During study participation, child participants underwent an asthma and AR clinical evaluation. Herein we report the extent to which AR was diagnosed and treated by urban healthcare providers in this sample of urban school-aged children with persistent asthma symptoms, specifically (1) proportion of children who met criteria for AR, (2) proportion whose caregivers reported no previous diagnosis of their child's allergies, (3) caregivers' and healthcare providers' perceptions of child's allergic status, compared with the study assessment of allergic status, and (4) proportion of children with AR who were undertreated or lacked treatment for the condition. Finally, we compared self-report of asthma control in participants with well-controlled versus poorly controlled AR over a 4-week period following the study clinic session.
We hypothesized that given participants had persistent asthma for study inclusion, there also would be a high percentage of AR diagnosed by their healthcare provider, especially in those with moderate/severe persistent rhinitis symptoms. Furthermore, we hypothesized that participants with comorbid AR would be taking some AR medication for upper airway symptoms, and that poorly controlled AR would be associated with poorly controlled asthma.
Materials and Methods
Patients
Participants were recruited from four ethnically diverse urban public school districts in Rhode Island. Data presented here include those of 166 children with persistent asthma who completed the Project NAPS study clinical evaluation during the first 3 years of data collection.
Inclusion criteria specified that children (1) were between the ages of 7 and 9 (the narrow age range allows for an in-depth understanding of the larger study's hypothesized associations during the school-age years, when this age group begins to be more independent with self-management behaviors), (2) resided and went to school in one of the four targeted districts, (3) had a primary caregiver fluent in English or Spanish, (4) had a physician diagnosis of asthma according to caregiver and healthcare provider report, or (5) met criteria for persistent asthma. Specifically, participants had to have an asthma controller medication prescribed and/or have daytime asthma symptoms greater than 2 days a week, nocturnal asthma symptoms greater than 2 times a month, short-acting beta-agonist use greater than 2 days a week, at least minor limitation in normal activity, and/or 2 or more oral steroid bursts per year. Those excluded had additional pulmonary disease, significant developmental delay, or a severe psychiatric condition.
Study design
Participant recruitment occurred through school nurses within the four targeted urban school districts and from primary and specialty clinics at Rhode Island Hospital (RIH). Participants were recruited by convenience sampling. During an initial study visit, families underwent the informed consent process and completed demographic and other self-report assessments. All participants completed an asthma and allergy evaluation by a pediatric asthma specialist, one component of the larger NAPS protocol to ensure that study criteria were met before participation continued. The clinic study visit consisted of a medical history and physical examination, allergy skin prick testing, and pulmonary function testing. A “physician query” was faxed to the regular healthcare provider to obtain background medical information about the child. Asthma control and rhinitis control were measured by participant report at the end of a 4-week period after the study clinic session. The Institutional Review Board at RIH approved the study protocol.
The research protocol was administered to the child and caregiver in English or Spanish, according to respondents' preferences. Race/ethnicity was based on caregiver self-report.
Study measures
Physician query
The physician query was a brief chart abstraction form querying date of last visit, diagnosis of asthma and/or rhinitis, surgical history (e.g., tonsillectomy and/or adenoidectomy), significant medical history, and current asthma and rhinitis medications. Physician queries were sent to the primary care providers and an asthma specialist if identified. Two key questions were asked of healthcare providers about rhinitis: (1) Does this patient have intermittent or persistent rhinitis symptoms (not associated with acute infections)? (2) Do you suspect environmental allergies? There was a high return rate (96%) of queries.
Poverty threshold and healthcare access
Poverty status was determined by family per-capita income in relation to U.S. federal poverty thresholds.12,13 Healthcare access was assessed by a dichotomous variable—the child participant having at least one physician visit in the past year, which is a broad measure of access to the healthcare system for both acute and chronic conditions.14,15
Asthma severity and asthma control
Persistent asthma status was assessed by an asthma specialist during the clinic session. Both asthma severity and control were classified according to NHLBI EPR-3 criteria. 16 Baseline lung function (FEV1) was measured via the Koko Incentive Spirometer (nSpireHealth, Longmont, CO) before and after administration of a short-acting beta-agonist following American Thoracic Society standards. 17 Emergency room visits and oral steroid bursts for asthma in the past 12 months before study entry were assessed by self-report at baseline. Adherence to asthma medication at study entry was also queried using a 5-point Likert scale: 1=never to almost never missed, 2=occasionally missed, 3=missed about half the time, 4=missed more than half the time, to 5=missed almost all the time.18,19
Caregiver perception of allergy status
Before allergy skin prick testing, caregivers were asked questions about their child's nasal symptoms: (1) Do you think your child has allergies, and (2) has your doctor ever told you or diagnosed your child with allergies? Caregivers were asked whether their child ever had allergy testing before the research clinic visit.
Rhinitis symptom summary
At baseline, to assess descriptive information of rhinitis symptoms, a 21-item scale was administered to the child and caregiver, including a severity scale for each symptom (from 0=absent to 4=prevents daily activity or sleep), 20 and frequency of nasal symptoms (intermittent vs. persistent). 9 The question regarding persistence of symptoms, “Did this symptom last for more than 4 days a week for EVERY SINGLE week of the past month?” was added to the scale based on Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines. 9
AR diagnosis and severity
Rhinitis symptoms were evaluated by the study clinician by (1) evidence on physical examination,9,21 (2) caregiver-reported child rhinitis symptoms, 20 and (3) allergy skin prick testing to perennial and seasonal allergens common to the area (Dermatophagoides farinae, Dermatophagoides pteronyssinus, cat, dog, cockroach, mold mix, tree, grass, ragweed, plantain pollen, and mouse; Greer Laboratories, Lenoir, NC). Skin testing was performed (Multi Test II device; Alk Abello, Round Rock, TX) after appropriate medication washout. If participants were found to have rhinitis, severity was classified as intermittent or persistent and mild or moderate/severe based on ARIA guidelines. 9 If diagnosed, AR was also separately categorized by allergic triggers using U.S. Practice Parameter recommendations (perennial AR; seasonal AR; perennial AR with seasonal exacerbation; or episodic AR). 1
Asthma control and rhinitis control during the monitoring period
The Childhood Asthma Control Test (C-ACT) administered at the end of the monitoring period measured level of asthma control by caregiver and child participant report. 22 The scores of test items are summed for a total score (0–27), with lower scores indicating poorer asthma control.
The rhinitis control assessment test (RCAT) administered at the end of the monitoring period measured rhinitis disease control by caregiver report. 23 The rating scales of 6 items (frequency of nasal congestion, sneezing, and watery eyes; sleep interference; activity avoidance; and self-assessed control) are added for a total score (6–30), with lower scores indicating poorer control. A score of 21 and below denotes “poorly controlled rhinitis.” 23
Statistical analysis
A new diagnosis of AR was calculated as the proportion of children who received a diagnosis of AR at the study clinic session and whose caregivers reported that they were not told previously by their regular healthcare provider that their child had allergies. Concordance between caregiver perception (Do you think your child has allergies?) and the research study assessment of AR status was measured by Cohen's kappa. Similarly, concordance between healthcare provider perception (Do you suspect environmental allergies?) and the research study assessment of AR status was measured by Cohen's kappa. During the monitoring period, scores on the C-ACT and RCAT were analyzed using Pearson's correlation. Differences in C-ACT scores between participants with well-controlled AR and poorly controlled AR were analyzed by one-way analysis of variance. Significance levels were set to p<0.05.
Results
Demographics
Two hundred fourteen participants with asthma enrolled in Project NAPS during the first 3 years of data collection. Twenty-nine deemed ineligible after enrollment were excluded. Ineligible participants had intermittent asthma (12), no asthma (7), or confounding medical or sleep conditions (10). Nineteen enrollees did not complete the study clinic visit, leaving a total of 166 participants with persistent asthma who completed the clinic study session. The excluded participants were similar in demographic profile (sex, age, ethnicity, poverty status) to included participants except for not meeting inclusion criteria. Of the 166 participants, children were, on average, 8.4 years old (SD=0.87). Forty-six percent were female. The race/ethnicity distribution was majority Latino (52%), followed by African American (31%), and non-Latino white (17%). Sixty-eight percent were at or below the poverty threshold. Ninety-six percent had a medical visit within the 12 months before study entry. Seventeen percent reported ever having seen an asthma/allergy specialist. Twenty-seven percent reported ever having an allergy test in their lifetime.
Characteristics of asthma and rhinitis are shown in Table 1. Asthma was not well-controlled in 77% of the children. Fifty-six percent had moderate-to-severe asthma based on NHLBI EPR-3 criteria. 16 Forty-five percent of participants reported using the ED for asthma and taking oral steroid bursts for asthma in the year before study entry. Seventy-two percent had persistent rhinitis symptoms (nasal symptoms more than half the week every week of the month), assessed by caregiver and child report. Of the patients with rhinitis, 24% had mild rhinitis symptoms (not troublesome), 54% had moderate symptoms (nasal symptoms disrupted either daytime activity or nighttime sleep), and 22% had severe symptoms (nasal symptoms disrupted both daytime activity and nighttime sleep). Seventy percent of caregivers reported that their child had nasal congestion in the past 4 weeks. The majority of participants were confirmed to have AR (86%), based on allergy testing and symptom report.
Five-point Likert scale: 1=never to almost never missed, 2=occasionally missed, 3=missed about half the time, 4=missed more than half the time, 5=missed almost all the time.
6% of participants reported taking ICS as needed.
Those with rhinitis were N=163 from N=166.
Three participants were not able to undergo allergy testing.
Those with AR were N=137 from N=160.
ARIA, Allergic Rhinitis and its Impact on Asthma; ICS, Inhaled Corticosteroid; ED, Emergency Department.
AR classification by triggers appears in Table 1. Most allergen exposure was because of perennial triggers (93% had positive testing and exposure to perennial allergens). The majority of study clinic visits and monitoring period that followed occurred between August and January. Of the 26% participants who had ragweed allergy (whether mixed with perennials or exclusively seasonal), 42% were in ragweed season during that time. Six percent of participants were exclusively tree/grass/ragweed allergic and were out of season (n=8/137), which did not change the primary study results.
Underdiagnosed AR
Of the 86% child participants with AR, 53% were newly diagnosed at the clinic visit. The proportion of caregivers who correctly perceived allergic status was 0.79. Concordance between caregiver perception and research study assessment was significant (κ=0.19, p=0.02). The proportion of healthcare providers who correctly perceived allergic status was 0.5. Concordance between healthcare provider assessment and research study assessment of AR status was not significant. Some caregivers (9%) and healthcare providers (20%) endorsed don't know. For those reporting moderate/severe persistent AR symptoms at the research clinic visit, 60% of healthcare providers correctly suspected allergic triggers on the physician query.
Undertreated AR
The remainder of analyses below focuses on participants with positive AR status. Only 33% of the child participants diagnosed with AR at the study visit were receiving appropriate treatment using ARIA recommendations, as reported by their caregiver. The remainder received no treatment (37%), was undertreated (28%), or overtreated (2%). Fifteen percent of caregivers reported that their child was using intranasal steroids.
We also describe treatment for AR and asthma prescribed by the healthcare provider as reported on the physician query (see Fig. 1). Intranasal steroids were endorsed by healthcare providers 16% of the time, while intranasal antihistamines were not endorsed at all. We further split out those participants with uncontrolled asthma who reported moderate/severe persistent AR symptoms, and the rate of intranasal steroids endorsed by the healthcare provider on the physician query was still low at 15%.
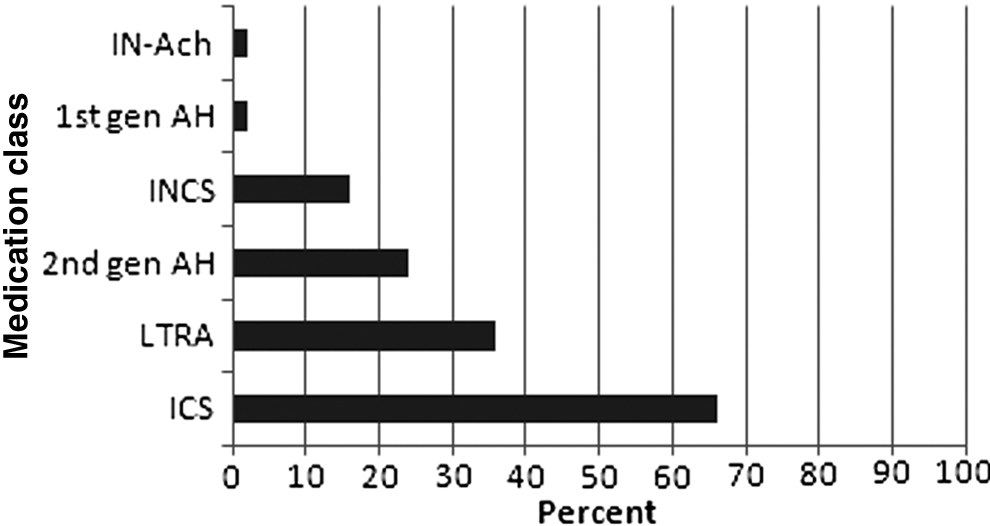
Healthcare-provider reported treatment of allergic rhinitis and asthma on the physician query. 1st gen AH, oral first-generation antihistamine; 2nd gen AH, oral second-generation antihistamine; ICS, inhaled corticosteroid; IN-Ach, intranasal anticholinergic; INCS, intranasal corticosteroid; LTRA, leukotriene antagonist.
Asthma control and rhinitis control during the monitoring period
Asthma control and rhinitis control scores were positively correlated during the monitoring period following the study clinic visit (r=0.3, p<0.05). Moreover, child participants with poorly controlled rhinitis had significantly less control of their asthma compared with those with well-controlled rhinitis (F=6.3, p<0.05).
Discussion
This is a novel study in the U.S. investigating AR control and management in urban school-aged children with persistent asthma. Many children in our sample had underdiagnosed and undertreated AR. Over 80% with asthma had AR, a finding that is consistent with previous studies1,9; however, we found that for half of our sample AR was undiagnosed. Surprisingly, only a third of child participants with AR were using appropriate treatment according to practice guidelines.1,9 Only 60% of participants' healthcare providers recognized the role of allergies in those participants who reported moderate/severe persistent AR symptoms, a group that qualifies for referral to a specialist. Only 15% in our cohort reported using intranasal steroids, whereas over 60% should have received this treatment according to ARIA guidelines. 9 During the monitoring period, children with poorly controlled rhinitis had poorer asthma control than children with well-controlled rhinitis. There is a clear need for intervention in this urban school-aged group with asthma and AR.
Education is needed for both healthcare providers and families
Our results are consistent with other surveys in the United States and Europe, though to our knowledge, previous work has not focused specifically on AR in urban children with persistent asthma. About 27 to 30% of physicians underestimate the impact of AR on their patients' daytime functioning, 24 and 32% of teenagers and adults have undiagnosed rhinitis. 25 Underdiagnosis of childhood allergies has been found even in young, pre-school-aged children. 26 The urban context of our sample and the children's concurrent asthma status are important to highlight. Three-fourths of our childhood sample, who were primarily from ethnic minority backgrounds, had poorly controlled asthma. Though the majority reported having a prescription for inhaled corticosteroids for asthma, the participants' nasal symptoms were largely overlooked.
Underdiagnosis of AR is an area that has been recognized for further guideline-based education. Although an available Pocket Reference for Primary Care Providers4,27 and written Rhinitis Action Plans exist 1 and have been disseminated widely, they still need to be emphasized in urban areas.
AR treatment deserves emphasis in urban areas
Few caregivers in our sample reported the use of intranasal steroids for their children's allergies. This reflects a persistent deficit in meeting guideline-based standard of care28,29 for the majority of our sample who had moderate/severe persistent rhinitis symptoms. Similarly, in other studies, use of intranasal steroid in both children and adults was also low, ranging from 11 to 26%.25,30–33 One large-scale U.S. survey found that 24% of children took no AR medication at all. 32 While patient adherence may play a role in our sample, the impact was likely minimal given that only 33% received appropriate AR treatment. Information from our physician queries indicated that for many, AR medications simply were not prescribed. Our results support findings of other studies and raise awareness of urban needs.
Practice parameters for AR published in the United States1,34,35 highlight the advantages of step-up or combination therapy with intranasal antihistamines. In our urban sample, no participant was prescribed an intranasal antihistamine, perhaps because it is not listed on the approved formulary of the two most common insurance plans available to school-aged patients with low socioeconomic status in Rhode Island. There is clearly a disparity in the delivery of rhinitis care to urban children if step-up therapy is not available.
Our findings of underdiagnosed and undertreated AR among urban children may be because of the prioritization of lower rather than upper airway symptoms, insufficient education surrounding the role of AR in asthma morbidity, and competing urban priorities surrounding poverty and neighborhood safety.
AR control impacts asthma control
Our findings of poorer asthma control in children with poorly controlled rhinitis compared with well-controlled rhinitis support other studies demonstrating the links between AR and asthma control. Incomplete asthma control in children was significantly more likely in children with AR than in those without. 36 Rhinitis was more frequent when control of asthma was worse. 37 Both retrospective and prospective claims data show that treating AR reduces asthma-related hospitalizations and emergency room visits by about half.38–40
Clinical implications
Most patients with asthma have AR, and AR often exacerbates asthma. A model has been proposed to illustrate the concept of “one airway,” 6 which emphasizes the need for healthcare providers who treat patients with asthma also to consider aggressive treatment of coexisting AR.1,9 This is essential for urban children with high asthma morbidity rates at risk for poor school functioning1,41 In these children with high population attributable risk for hospitalization and ED visits, the role of allergies cannot be ignored.
Study limitations
Several study limitations bear mention. This is a descriptive study within a larger protocol. It was not designed to study communication patterns between healthcare providers and caregivers, nor to assess the breadth of knowledge of practitioners in this setting regarding the treatment of AR. There was no control group of nonurban children, nor was there a control group for AR alone (no asthma). Comparisons with these additional control groups will be considered in future studies. We simply raise awareness of gaps in asthma care in urban areas. While we expected low report of intranasal corticosteroids on the part of patients, it was surprising to find that practitioners also prescribed intranasal steroids infrequently even for those participants with uncontrolled asthma who reported moderate to severe persistent AR symptoms. Second, insurance status was not measured; however, Rhode Island is unique in that managed Medicaid insurances have wide coverage in these urban school districts, ensuring some access to a healthcare provider, though not always a regular provider. 42 Notably, 96% of our sample had a documented medical visit within the 12 months before study entry. Although this visit may not have been specifically for asthma, it was important to obtain the most recent documented medication list. The primary purpose of the physician query was to provide additional clinical information to aid in the clinician's diagnosis and assessment of severity of asthma and allergies for the larger study. Third, for participants who were treated in group practices, the physician query may not have been completed by the primary healthcare provider. Prescriptions are charted, however, and undertreatment of rhinitis was readily apparent from our physician query data. Fifth, history of allergy testing was not queried in the physician query. Given that families did not always see the same healthcare provider, we elected to ask the caregiver directly. Finally, this was a descriptive study, so we did not control for seasonal allergen exposure per se. We have described the frequency of exclusive seasonal triggers, which was very low for the timeframe described. The majority of allergen exposure was primarily because of perennial triggers.
In spite of publications of ARIA guidelines and U.S. Joint Practice parameters over the past 15 years, the diagnosis and treatment of AR may be insufficient for specific high-risk groups. Education about the importance of AR in the co-management of asthma is necessary in urban populations with increased asthma morbidity. Future directions include exploring gaps in practitioner knowledge and barriers to allergy testing; exploring communication barriers between practitioners and caregivers about AR symptoms and treatment; examining the effects of asthma and AR on sleep and school performance; and mitigating competing urban factors that preclude the diagnosis and treatment of allergies.
Footnotes
Acknowledgments
The authors thank the children and their families who participated in Project NAPS, and acknowledge the dedicated work of research assistants, school nurse teachers, and clinic staff. We thank Brittney Williams and Kara Ramos for their assistance with article preparation.
The project described was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development (R01 HD057220 to D. Koinis Mitchell, principal investigator).
Author Disclosure Statement
No competing financial interests exist.