
Abstract
Background:
Physicians' assumptions about patients' socioeconomic status (SES) have been shown to influence clinical decision making in adult patients. The goal of this study is to assess the factors associated with pediatric pulmonologists' (PPs') subjective ratings of their patients' SES, and whether these factors differ by patient race/ethnicity.
Methods:
Parents of children with asthma (n=171) presenting for pulmonary care reported their SES using the MacArthur Subjective SES 10-rung ladder. The PPs (n=7) also estimated each family's SES. Two-level linear regression models with random intercepts (level 1: PP's SES ratings; level 2: PPs) were used to assess the predictors of PP-estimated family SES. The analyses were then stratified by race/ethnicity.
Results:
Parental educational, insurance type, age, and race/ethnic background were associated with PPs' SES ratings. Black/African American families were rated lower than white families, accounting for other demographic factors (b=−0.60, p<0.01), but families of other races/ethnicities were not (b=−0.10, p=0.29). Even when comparing families with the same level of parental education, black/African American families, but not families of other backgrounds, were judged to have lower SES than white families (from 0.77 rungs lower among parents with some college, to 1.2 rungs lower among parents with high school or less; both p<0.05).
Conclusions:
Racial differences in PPs' ability to estimate families' subjective SES in asthma care may be a function of unconscious societal biases about race and class. Collecting subjective SES from families and PPs during the office visit could facilitate discussions about material and psychosocial needs and resources that influence treatment effectiveness.
Introduction
A
Some of the etiology of socioeconomic and racial/ethnic asthma disparities may be related to what happens during pediatric office visits when providers are evaluating and treating the child's asthma. 5 Physicians bring their own set of assumptions and expectations to clinical encounters.6,7 A considerable body of evidence suggests that patient characteristics influence physician behavior, diagnosis, and treatment.7–9 Studies in adults demonstrate that physicians are more likely to view low-SES and African American patients as noncompliant, less socially supported, and less intelligent than their peers. Further, physicians perceive African American patients as less educated than white patients, a difference that persists even after accounting for sociodemographic characteristics. 9
Although most research has focused on adult patients, studies in children suggest that assumptions about race and class may also shape care in pediatric settings. For example, physicians significantly underestimate asthma severity among African American children,5,10 and are more likely to perceive racial/ethnic minority families as less compliant with clinical recommendations. 11 In addition, physicians indicate that a key reason for not prescribing inhaled corticosteroid therapy for children with asthma is a concern that the family will not be able to afford it. 12 While there is growing evidence that pediatricians' assumptions about families' socioeconomic resources affect care, the validity of these assumptions is largely unknown. The goal of this study is to assess the factors associated with pediatric pulmonologists' (PPs') subjective ratings of their patients' socioeconomic status (SES). We use subjective social status as a measure of SES, an approach that allows PPs and patients to estimate SES using the same measure.
Materials and Methods
Patients/participants
Participants were parents (or legal guardians) of children who presented for outpatient pediatric pulmonary care at the Johns Hopkins Children's Center between July 1, 2010, and October 1, 2010. A study staff member approached every parent who met the eligibility criteria before their visit to invite them to participate. Subjects were eligible if their child: (1) had doctor-diagnosed asthma; (2) was presenting for a scheduled appointment; (3) resided in the United States; and (4) was accompanied by a caregiver who could provide consent to participate in the study. Of the 193 children who met eligibility criteria, 187 (97%) enrolled, and 182 (94%) completed the survey. Of those approached but not enrolled, one patient was not currently residing in the United States, two patients were not accompanied by a primary caregiver, and two caregivers refused participation. Eleven enrolled patients were excluded because their PP did not estimate family SES for any patient (n=7, 3.8%) or for their family specifically (n=4, 2.2%). This yielded a final sample of 171.
Study design
After providing written informed consent, parents completed a paper and pencil survey that assessed subjective SES and other sociodemographic characteristics. After each visit, their PP estimated the family's SES. Participating PPs were pediatric pulmonology faculty and fellows. The university's Institutional Review Board approved this study.
Measures
SES
The MacArthur Scale of Subjective Social Status SES Ladder 13 was used as a summary measure of SES. A picture of a ladder is prefaced by text that directs the respondent to imagine that the ladder represents where people stand in the United States. Those at the top are the best off (in terms of money, education, and respected jobs); those at the bottom are the worst off in these domains. Respondents mark the rung (i.e., 1 to 10) that shows where they see themselves relative to others in the United States, with higher rankings indicating higher status. SES ladder rankings are highly correlated with objective measures of income, education, and occupation 14 and have been found to have adequate test–retest reliability. 15 Subjective social status captures cumulative effects of SES, life events, and social hierarchy, and may therefore be a more sensitive and inclusive indicator of social position than objective SES.16,17 Position on the ladder is a robust predictor of self-rated health, mortality, and a number of other health conditions, such that those with higher SES ladder rankings experience better health.18–21
The primary outcome measure for this study was the physician's estimate of the family's SES ladder ranking. The patient's PP indicated where he/she believed the family stood in relation to others in the United States. This approach allowed the PP to estimate relative SES using a measure that is highly correlated with objective SES, without requiring him or her to estimate parents' income, education, and occupation.
Characteristics of parents/caregivers
Parents/caregivers used the SES ladder to rate their family's SES. They also reported their relationship to the child, age, sex, highest level of education, and insurance type. Education was categorized as high school or less, some college, or 4 year college degree or more. Child's race/ethnicity was collapsed into white, black/African American, and “other” racial/ethnic group (Hispanic/Latino [not black], American Indian/Native Alaskan, Asian, Pacific Islander, and multiracial). Child race/ethnicity was used as a proxy for family race/ethnicity. The family's health insurance was classified as Medicaid or private insurance.
Characteristics of PPs
PPs reported their sociodemographic characteristics (age, sex, and race/ethnicity). They also rated their familiarity with the family on a 5-point Likert scale which ranged from 1=“know the family not at all well” to 5=‘know the family very well.”
Statistical analysis
The primary goal of the analysis was to examine the factors associated with PP-estimated family SES (dependent variable), including characteristics of the parent, the patient (i.e., race/ethnicity), and the PP (independent variables). First, to determine whether parent ratings were related to objective indicators of SES or other factors PPs might be able to perceive in the course of a visit, we used ordinary least squares regression models, with parent rating as the dependent variable and parent characteristics as the independent variables. Next, two-level linear regression models with random intercepts (level 1: PPs' ratings for individual patients; level 2: PPs) were used to assess the predictors of PP-estimated family SES, in order to account for the nonindependence of ratings by the same PP. Unadjusted models were fit first, and then covariates that were significantly related to PPs' SES ratings in unadjusted models were added to adjusted models. Continuous covariates were group mean-centered for interpretability. 22 Models were then stratified by child race, and the relationships were compared across strata. Finally, in post hoc analyses, we explored whether the unadjusted relationship between child race/ethnicity and PP ladder rankings differed by the parent or caregivers' highest level of education by stratifying the multilevel models by education. The limit for statistical significance was set at p<0.05. Statistical analyses were performed using Stata v13 (StataCorp, College Station, TX).
Results
Families who enrolled but were excluded from the analysis were similar in terms of education, race/ethnicity, and insurance type, but they reported higher subjective social status (p<0.05). There was no item-level missing data, with the exception of parent age. Four percent of parents declined to provide their age. Sensitivity analyses comparing a complete case analysis with an analysis using imputed caregiver age were consistent, so we provide the results of the complete case analysis.
Description of the sample
The demographic characteristics of the 171 parents and other caregivers (hereafter referred to simply as parents, since 93% were parents), as well as the characteristics of their seven PPs, are summarized in Table 1. The distribution of parent and PP SES ladder rankings is summarized in Figure 1.
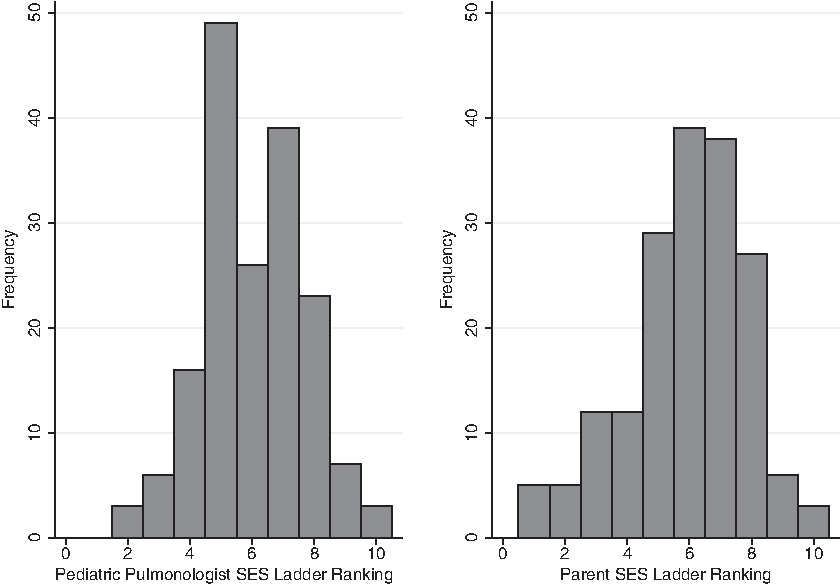
Distribution of pediatric pulmonologist- and parent-rated family socioeconomic status ladder rankings.
Note. Percentages may not add to 100% due to rounding.
5=“knows family very well”; 1=“knows family not at all well.”
Parents' SES ladder ratings
In unadjusted comparisons, parents with a high school education or less rated themselves 1.8 rungs lower than those with a college degree, F(2, 168)=17.9, p<0.001; those with Medicaid rated themselves 1.1 rungs lower than those with private insurance, F(1, 169)=16.6, p<0.001; and African Americans rated themselves 0.9 rungs lower than white parents (p=0.004). There were no significant differences in ranking by race/ethnicity for white parents compared to parents of other races/ethnicities. In an adjusted model including all of the family sociodemographics, the relationship between race/ethnicity and the family's SES rating disappeared. The predictors of family SES ratings were similar for African American and white families in adjusted models.
PP characteristics and their SES ratings
Each PP rated between 11 and 49 patients (M=24; see Fig. 1). The mean rating was 5.97 (SD=1.49), accounting for nonindependence of ratings between PPs. PPs' sociodemographic characteristics (i.e., age, sex, race/ethnic background) were not associated with their family SES rankings, nor was their familiarity with the family. Thus, adjusted models did not include PP characteristics.
Family characteristics and PPs' SES ratings
PPs' ratings were related to each of the family sociodemographic variables except the respondent's relationship to the child. In separate, unadjusted two-level linear regression models, PPs' ratings were significantly positively associated with parents' own SES ratings (b=0.31, p≤0.001) and parents' educational attainment. Parents with at least a college degree were rated 1.7 rungs higher (p<0.001), and those with some college were rated 0.74 rungs higher (p=0.004) than parents with a high school education or less. Patients with Medicaid were ranked one rung lower than those with private insurance (5.1 vs. 6.1, p<0.001). Younger parents were rated lower than older parents (b=0.05, p<0.001). In addition, there were significant differences in PP ratings by the family's race/ethnic background. Compared to white patients, black/African American families were rated 1.3 rungs lower (p<0.001). Ratings for families of other races and ethnicities were not significantly different from ratings for white families.
In an adjusted model that included all of the family sociodemographic variables (see Table 2), parental education, insurance type, parental age, and black/African American race/ethnicity remained significantly associated with PPs' SES ratings.
Parameter estimate standard errors listed in parentheses. Adjusted model includes family characteristics. Parent SES ladder, parent age and physician age are group mean centered.
, p<0.01; ***, p<0.001.
SES, socioeconomic status; ICC, intraclass correlation coefficient.
Table 3 summarizes race/ethnic differences in the factors associated with PPs' SES ratings based on unadjusted and adjusted multilevel linear regression models. While black/African American families were rated significantly lower than white families in adjusted models (p<0.001), families of other races/ethnicities were not (p=0.34). Even after accounting for family sociodemographic characteristics, this disparity persisted. Among white families, PPs' SES ratings were related to parental education level, insurance type, and caregiver age. Among black/African American families, ratings were associated with parental education and insurance type; among families of other races/ethnicities, PPs' ratings were associated with parental SES ratings, education, and parental age.
Parameter estimate standard errors listed in parentheses. Adjusted model includes family characteristics. Parent SES ladder, parent age and pediatric pulmonologist age are group mean centered.
†Black/AA vs. white, p<0.0001; other vs. white, p=ns.
‡Black/AA vs. white, p<0.01; other vs. white, p=ns.
, p<0.05; **, p<0.01; ***, p<0.001.
In post hoc analyses, we evaluated the unadjusted relationship between PPs' SES ratings and family race/ethnicity, comparing families with similar levels of parental education. We found that within each stratum of parental educational attainment, black/African American families, but not families of other races/ethnicities, were judged to have statistically significantly lower SES than white families. Specifically, black/African American families with a high school education had a mean PP-rated SES of 4.74 (SE=31) compared to 5.90 (SE=0.45) for whites and 5.00 (SE=0.64) for other families (black/AA vs. white: p<0.05). Among those with the most education, a 4 year college degree or more, white families were rated on average 6.94 (SE=0.37) compared to 5.92 (SE=0.56) for black/African American families and 6.65 (SE=0.55) for other families (p<0.01). A similar pattern was observed for those with some college.
Discussion
Our results suggest that PPs use several family characteristics to draw conclusions about the SES of their pediatric asthma patients—parental educational level, whether the family is publically insured, and the parents' age. However, they also use the race/ethnicity of the patient as an indicator of SES. After accounting for other family sociodemographic characteristics, black/African American patients were judged to be of significantly lower SES than their white peers. This disparity was only evident for black patients—race was not related to PPs' SES ratings among families of other races/ethnicities. We did not find evidence that the factors that PPs used to estimate SES varied considerably for white and black families, but their ratings did. When we compared families of different race/ethnic backgrounds with the same level of parental education, the disparity persisted. Even among families in which the parent had at least a 4 year college degree, black/African American families, but not those of other races, were rated lower than white families.
Surprisingly, PPs' sociodemographic characteristics, including race/ethnic background of the provider, were not associated with their SES estimates. Further, familiarity with the family was not correlated with SES ratings; this suggests that PPs' SES assessments reflect cues that were discernible in a brief clinical encounter, rather than a nuanced understanding of the family's actual circumstances. This supports findings from van Ryn 7 and others who have found that physicians use race/ethnicity as a heuristic in clinical decision making. Categorizing and generalizing (i.e., stereotyping) are important and adaptive strategies humans use to make sense of the world. 9 The time-pressured, stressful nature of clinical practice may increase the likelihood of using these mental shortcuts to expedite the patient assessment process. 9 Our study is consistent with previous studies in adults suggesting physicians have an implicit preference for white patients compared to black patients.9,23
When we examined the factors that families themselves used to place themselves on the SES ladder, educational level and medical insurance type were significantly associated with this rating. This suggests that families' own perceptions of their SES ratings are consistent with objective indicators of SES that their PP might be able to perceive or observe in the context of a clinical office visit. Whereas some previous studies have found that objective indicators of SES are less strongly related to ladder rankings among African Americans than whites,18,19,24 we found that both groups of parents relied on objective indicators of SES (e.g., parental education).
It is critically important to understand how to optimize healthcare and health systems to decrease socioeconomic and racial/ethnic disparities in asthma. Ideally, asking families to report on their subjective SES would prompt PPs to engage families in conversation about how to overcome socioeconomic barriers in order to facilitate achieving good health (i.e., asthma control and good asthma outcomes).
There are some limitations to this study. This study relied on a small convenience sample of PPs at an academic medical center and should therefore be considered preliminary. It is unclear whether we would see the same results with primary care physicians. However, the fact that PPs' familiarity with the family was unrelated to their ratings suggests PPs' and general pediatricians' ratings might be more similar than we might otherwise have predicted. Future studies using larger, more representative samples of providers and patients drawn from a variety of clinical settings could help clarify and extend our findings. We did not determine whether PPs' assessments of family SES influenced the treatment the child received, although previous research supports this as a possibility.9,25 Future research can help establish whether children whose families have the same objective SES but different subjective SES have different asthma-related health outcomes. Finally, more nuanced measures of family SES and measures of potential contributors or mechanisms (e.g., measures of physician unconscious bias, or patient- provider communication) would address gaps in the current study.
Conclusions
This study is a first step toward understanding physicians' subjective assessments of their patients' socioeconomic risks in the exam room. This study confirms previous research in adults that suggests that physicians underestimate the SES of racial and ethnic minority patients. 9 Research in this area is important to determining how healthcare providers and systems can improve care for low-resource populations as a means of addressing racial/ethnic and SES disparities in pediatric asthma. Rather than relying on PPs' perceptions of families' resources, our results suggest that providers should take a more direct approach. Assessing parent- and PP-rated subjective SES during the social history may allow physicians to begin a conversation about families' psychosocial and socioeconomic resources that could impact treatment adherence.
As advocated by the American Academy of Pediatrics, the family-centered medical home is key to reducing racial/ethnic disparities in child health. 26 Family-centered care includes increased attention to physician–patient communication and cultural competence. Consistent with the family-centered model, open communication about a family's socioeconomic resources may reveal otherwise unexamined barriers and facilitators to achieving asthma control. 26
Footnotes
Acknowledgments
S.J. wrote the first draft of the manuscript, but was not provided financial compensation to do so. S.J. is supported by a Career Development Award sponsored by the National Institute on Drug Abuse (NIDA; K01DA027229). J.J. was supported by KO1 DA022298 from NIDA. S.O. was supported by a Career Development Award sponsored by the National Heart Lung and Blood Institute (K23HL089410).
Author Disclosure Statement
No competing financial interests exist.