
Abstract
Introduction
T
Case Report
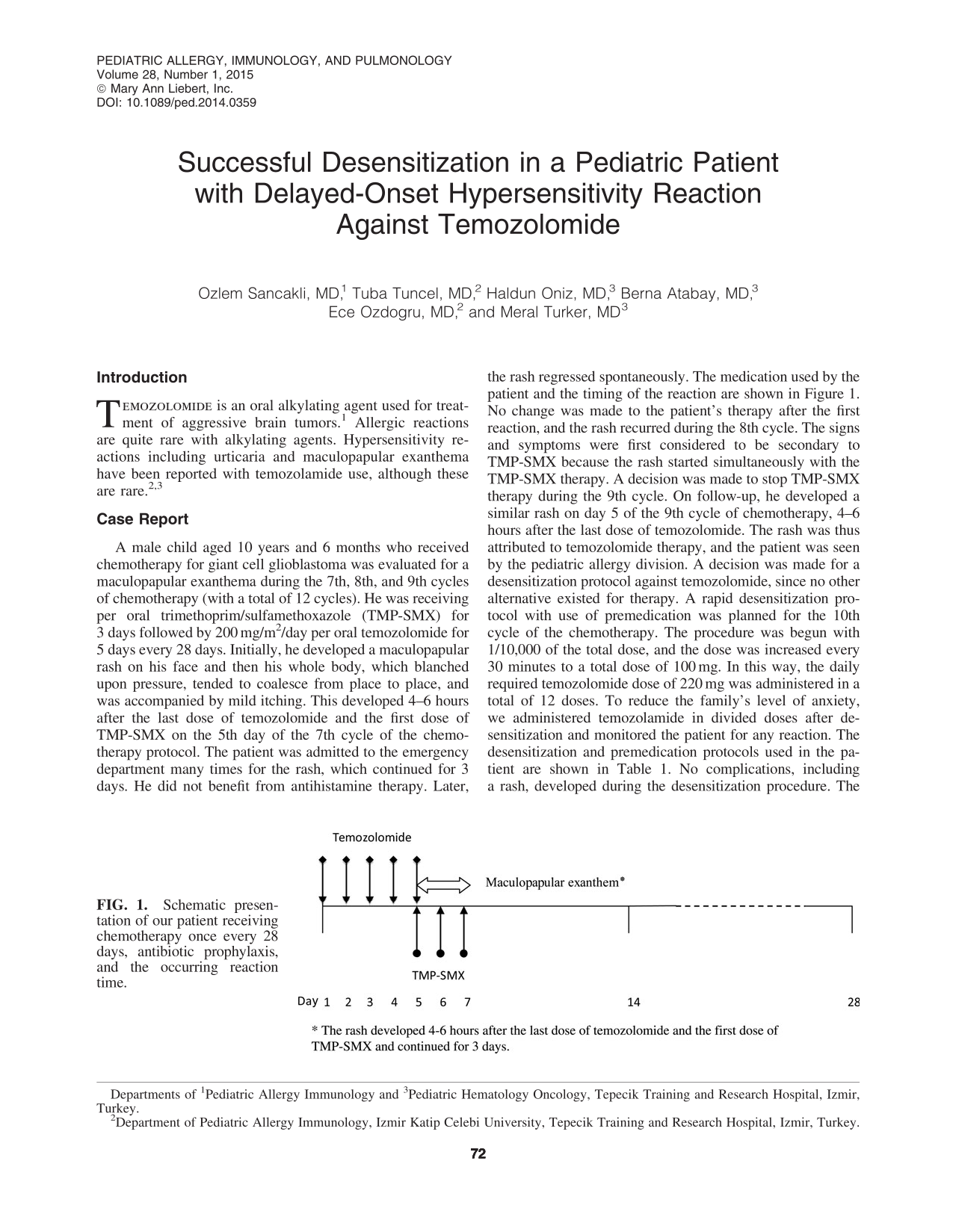
A male child aged 10 years and 6 months who received chemotherapy for giant cell glioblastoma was evaluated for a maculopapular exanthema during the 7th, 8th, and 9th cycles of chemotherapy (with a total of 12 cycles). He was receiving per oral trimethoprim/sulfamethoxazole (TMP-SMX) for 3 days followed by 200 mg/m2/day per oral temozolomide for 5 days every 28 days. Initially, he developed a maculopapular rash on his face and then his whole body, which blanched upon pressure, tended to coalesce from place to place, and was accompanied by mild itching. This developed 4–6 hours after the last dose of temozolomide and the first dose of TMP-SMX on the 5th day of the 7th cycle of the chemotherapy protocol. The patient was admitted to the emergency department many times for the rash, which continued for 3 days. He did not benefit from antihistamine therapy. Later, the rash regressed spontaneously. The medication used by the patient and the timing of the reaction are shown in Figure 1. No change was made to the patient's therapy after the first reaction, and the rash recurred during the 8th cycle. The signs and symptoms were first considered to be secondary to TMP-SMX because the rash started simultaneously with the TMP-SMX therapy. A decision was made to stop TMP-SMX therapy during the 9th cycle. On follow-up, he developed a similar rash on day 5 of the 9th cycle of chemotherapy, 4–6 hours after the last dose of temozolomide. The rash was thus attributed to temozolomide therapy, and the patient was seen by the pediatric allergy division. A decision was made for a desensitization protocol against temozolomide, since no other alternative existed for therapy. A rapid desensitization protocol with use of premedication was planned for the 10th cycle of the chemotherapy. The procedure was begun with 1/10,000 of the total dose, and the dose was increased every 30 minutes to a total dose of 100 mg. In this way, the daily required temozolomide dose of 220 mg was administered in a total of 12 doses. To reduce the family's level of anxiety, we administered temozolamide in divided doses after desensitization and monitored the patient for any reaction. The desensitization and premedication protocols used in the patient are shown in Table 1. No complications, including a rash, developed during the desensitization procedure. The desensitization procedure was successful, and the chemotherapy was completed in 12 cycles without any further complications.
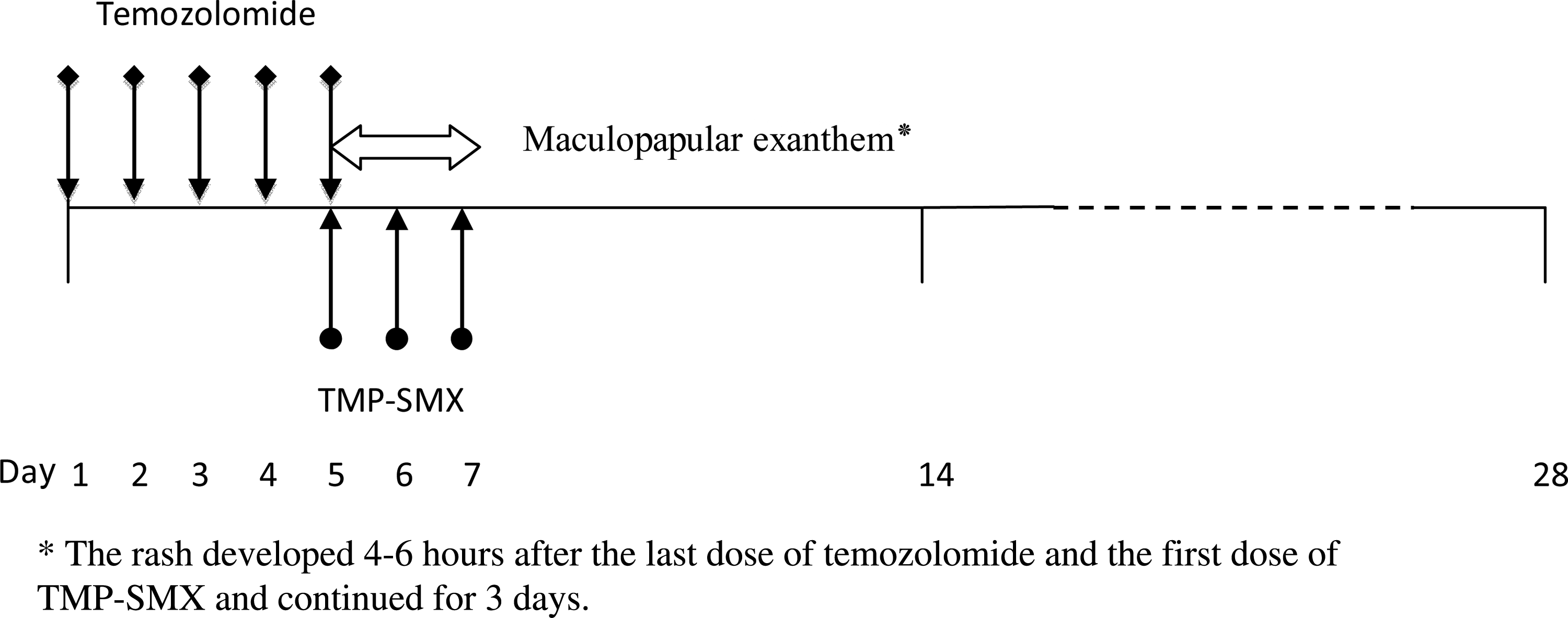
Schematic presentation of our patient receiving chemotherapy once every 28 days, antibiotic prophylaxis, and the occurring reaction time.
Per orally 1 and 13 hours before temozolamide.
Thirty minutes before the temozolamide dose.
Discussion
Drug hypersensitivity reactions are divided into two distinct types based on the onset of symptoms: early and late. Exanthematous drug reactions are the most common delayed drug reactions. In such cases, it is usually recommended to stop the suspected drug. However, desensitization offers an alternative option in cases where an alternative drug therapy is lacking, as in our case. 4 In the literature, successful desensitization applications to temozolamide have been reported in two women, aged 32 and 65 years old, with delayed onset hypersensitivity response, and in a 57-year-old woman with an early onset reaction.3,5
There are no standardized desensitization protocols in delayed-onset drug reactions. Different desensitization applications exist depending on the type of reaction, route of drug application, and pharmacokinetic properties of the drug. The decision regarding the desensitization procedure should be made on a patient-by-patient and drug-by-drug basis. 4 In our case, despite being a more risky application, a rapid desensitization procedure was performed, and the procedure was completed within 6 hours, since reaching a therapeutic level within a short time was desirable. There are reports in the literature of a similar rapid desensitization protocol applied successfully in cases of a delayed-onset allergic reaction to temozolamide. 3
Although premedication is controversial because of its ability to mask mild reactions in delayed-onset drug reactions, we opted to apply it with our desensitization protocol, since our patient was in the pediatric age group and his family was experiencing intense emotional stress. 4
In our case, there was a delayed onset with allergic reaction to temozolomide with high-grade gliablastome multiforme. Because there was no effective alternative therapy and immediate chemotherapy was needed, we applied a rapid desensitization protocol. To the best of our knowledge, our patient is the first pediatric case reporting an allergic reaction associated with the use of temozolamide in which a successful desensitization procedure has been applied. We have reported this case in order to emphasize that a rapid desensitization protocol can also be safely applied in pediatric cases with drug-associated delayed-onset hypersensitivity reactions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.