
Abstract
The presentation, evaluation, and management of chronic esophageal foreign bodies are not well described in pediatric patients. Many patients present with ill-defined respiratory symptoms, making diagnosis challenging. We report on a 2-year-old girl who presented with several months of worsening cough and wheezing unresponsive to medical management. She also had recent onset of feeding difficulty with certain consistencies. She underwent a joint bronchoscopy with the otolaryngology team. Bronchoscopy demonstrated severe tracheal narrowing and esophagoscopy showed severe inflammation. A chest computed tomography scan showed inflammation between the esophagus and trachea. Repeat esophagoscopy revealed an esophageal foreign body embedded into the anterior wall, which was removed via thoracotomy.
Case Report
A
She was referred to pulmonology. At the initial visit, she had a wet-sounding cough, which was worse at night, and daily wheezing worse with exertion. She had nighttime snoring, but had no apnea or cyanotic episodes. Her parents also reported several months of her holding solid food in her mouth and occasionally spitting it out. Her parents denied any recent choking or gagging events. She had no significant medical history, no history of gastroesophageal reflux, negative allergy testing, and no history of chronic sinus or ear infections. Family medical history was significant for asthma, but there was no history of Cystic Fibrosis, immunodeficiency, or other chronic pulmonary conditions. There was no smoke exposure, and she did not attend daycare.
On physical exam, her vital signs were normal for her age, with normal oxygen saturation on room air. Her growth parameters were the 75th percentile for age. In general, she had no respiratory distress, but had audible expiratory rhonchi. She had thick mucus present bilaterally at her nares. Inspection and percussion of the chest were normal bilaterally, with good aeration and no wheezing or crackles on auscultation. She had diffuse coarse expiratory rhonchi bilaterally. She had no clubbing or cyanosis.
After the initial evaluation, tracheomalacia was considered based on history and physical exam and she was prescribed as-needed ipratropium. A clinical diagnosis of laryngopharyngeal reflux was made and she was also started on ranitidine. A modified barium swallow investigation demonstrated a functional pharyngeal swallow with no aspiration or penetration of any consistency.
Joint flexible and rigid bronchoscopy was performed with otolaryngology. Flexible bronchoscopy showed a >95% posterior compression in the mid-trachea (Fig. 1). The remainder of the bronchial tree was normal with no evidence of secretions, cobblestone irregularity, or bleeding. Bronchoalveolar lavage was performed in the right middle lobe; cytology was normal and culture was negative. Rigid bronchoscopy confirmed >95% tracheal compression 2 cm proximal to the carina and moderate edema of the mucosa of the tracheobronchial tree distal to the obstruction. Rigid esophagoscopy revealed moderate-to-severe esophageal edema and very friable mucosa. Given the degree of esophageal inflammation, the bronchoscope was not passed further and was removed.
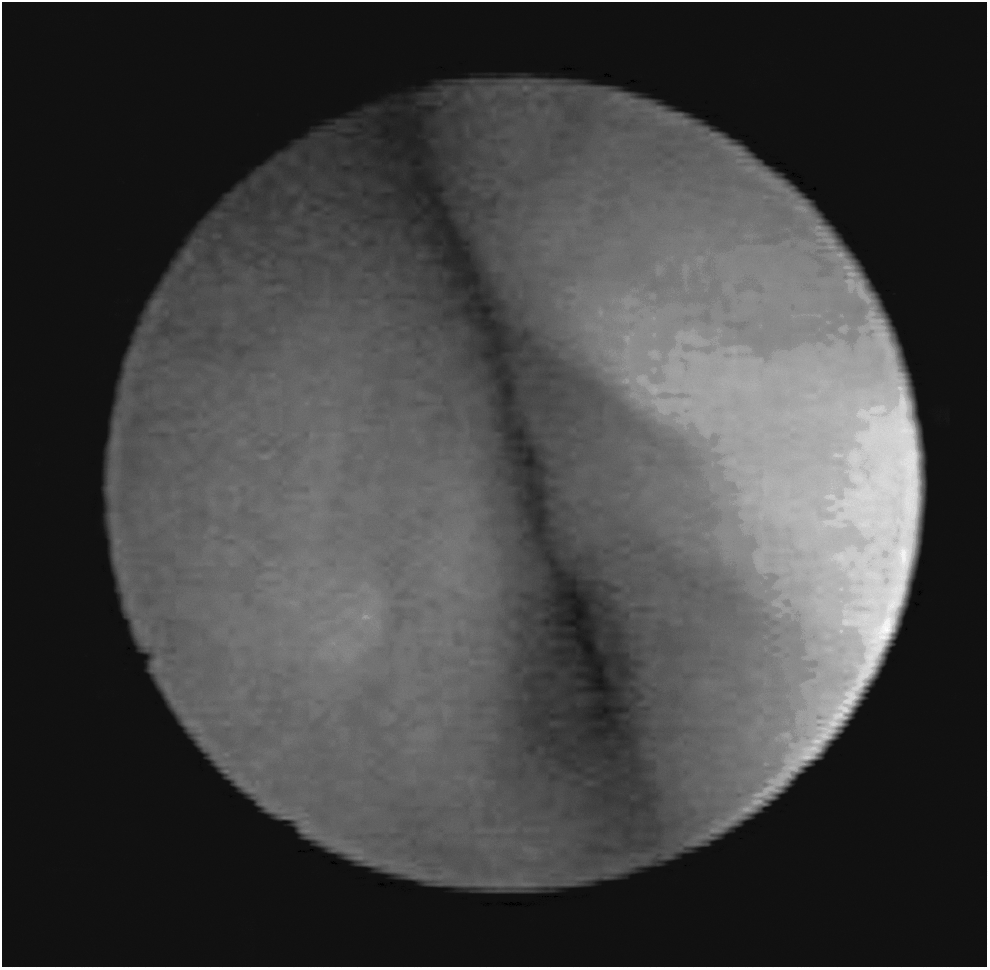
Flexible bronchoscopy demonstrating >95% posterior compression in the mid-trachea.
A chest computed tomography scan revealed diffuse inflammation between the trachea and esophagus and significant tracheal compression (Fig. 2). Mediastinal inflammation due to an esophageal perforation from an esophageal foreign body was suspected. Repeat rigid esophagoscopy showed a purple plastic foreign body embedded into the anterior esophageal wall. It was deeply fixed in the mucosa and unable to be removed endoscopically. She underwent a thoracotomy for removal of the foreign body and repair of the esophagus. She was taken to the operating room for extubation several days postoperatively, and her tracheal compression was resolved.
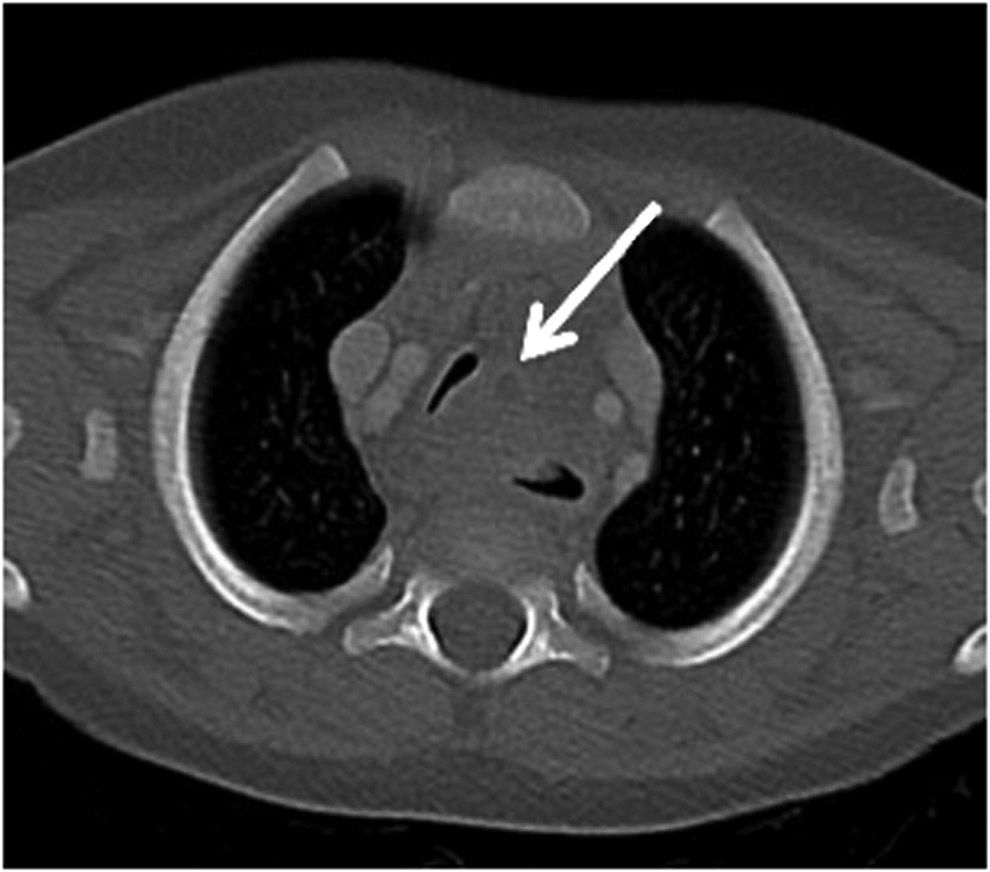
Chest computed tomography scan with severe diffuse esophageal wall thickening with stranding of mediastinal fat between the upper third of the esophagus and compressed trachea with presence of a rim enhancing 4.2 cm×5.2 cm fluid collection between the esophagus and trachea suspicious for phlegmon/abscess formation.
Discussion
Chronic esophageal foreign bodies are not well described in the pediatric population. Studies have shown that approximately 8–15% of all esophageal foreign bodies in children are chronic in nature (estimated impaction time >1 week).1,2 Miller et al. performed a retrospective review of children with chronic esophageal foreign bodies, and found most primarily presented with respiratory rather than gastrointestinal symptoms. Approximately three-quarters of children presented with complaints of respiratory distress and/or asthmatic symptoms. Half of sentinel events were unwitnessed, and the most common age of presentation was 7 months to 2 years. 2 This common presentation is important for pediatricians, pediatric pulmonologists, and pediatric gastroenterologists to remember when assessing children with respiratory symptoms that are poorly defined and/or recalcitrant to medical therapy.
Only 63–85% of all esophageal foreign bodies are visible on chest radiograph. 1 In children with concern for aspiration, a modified barium swallow investigation may elucidate functional abnormalities, but there are limitations in diagnosing esophageal foreign bodies. Alternatively, an esophagram may reveal lumen anatomic abnormalities (“filling voids”), and may be a reasonable second line radiologic technique that can lead to earlier diagnosis. 3 In patients with suspected foreign bodies and negative imaging, it is important to further assess with bronchoscopy and esophagoscopy.
“Red flags” include respiratory symptoms unresponsive to medical management, recurrent croup, abnormal oral-motor activities with food, choking or gagging during feeds, and mediastinitis or mediastinal abscess in an otherwise healthy patient.
In young children with such symptoms, bronchoscopy by a respiratory specialist is warranted for further investigation. However, when to enlist the help of otolaryngology or gastroenterology colleagues is often less clear. For the pulmonologist, tracheobronchial foreign bodies are often considered, but it should be noted that esophageal foreign bodies are twice as likely in the pediatric population. 4 Therefore, when a foreign body is on the differential, direct visualization in a multidisciplinary fashion may benefit the patient. As the incidence of serious morbidity increases significantly when diagnosis of an esophageal foreign body is delayed, it is important to pursue this line of action promptly when suspicion is high. 5
Conclusion
In a child with chronic respiratory symptoms recalcitrant to medical management, it is imperative to consider a foreign body. In pediatrics, foreign bodies are twice as common in the esophagus versus the tracheobronchial tree. Furthermore, chronic esophageal foreign bodies have been found to present primarily with respiratory symptoms. Diagnostic measures should include multidisciplinary evaluation by pulmonology, otolaryngology, and/or gastroenterology with both flexible and rigid bronchoscopy and esophagoscopy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.