
Abstract

Introduction
W
Methods
Both patients with DAH were admitted to the same pediatric intensive care unit. The patients were both in respiratory failure, requiring intubation and mechanical ventilation. Flexible bronchoscopy was performed via the preplaced endotracheal tube for direct visualization of the airways and instillation of rFVII. The dose administered was 50 μg/kg, diluted in normal saline and equally divided into the two main bronchi. Recombinant FVII was diluted in 50 mL of normal saline for the first patient, as suggested by the Heslet protocol. 3 However, dilution in only 25 mL of normal saline was used for the younger patient.
Case Reports
Case 1
This patient has been briefly reported previously. 1 A 16-year-old male was transferred to our pediatric intensive care unit with newly diagnosed acute myelogenous leukemia (AML). He responded well to therapy, but his course was complicated by pulmonary hemorrhage. The patient was transferred from another hospital after presenting originally with fever, pancytopenia, patchy bilateral pulmonary infiltrates, influenza A, and Aeronas veronii bacteremia. He rapidly deteriorated, developed diffuse bilateral pulmonary infiltrates and pulmonary hemorrhage, and progressed to respiratory failure requiring mechanical ventilation. Bone marrow biopsy revealed AML type 4. The hemorrhage was initially controlled with high doses of corticosteroids and supportive therapy of platelets, fresh frozen plasma, and cryoprecipitate infusions. The patient was started on chemotherapy and broad-spectrum antibiotics. Four weeks into admission while on AML therapies, he further deteriorated with persistent pulmonary hemorrhage requiring an increase in ventilatory pressures. With the recognition that the hemorrhage was unremitting and would most likely be fatal, informed consent was obtained from his guardians, emphasizing the experimental nature of the intended procedure. He underwent flexible bronchoscopy with instillation of rFVIIa into both main stem bronchi. During the procedure, active bleeding was noted from the left lower lobe bronchus.
The procedure was tolerated uneventfully and the pulmonary hemorrhage resolved shortly following the procedure. The patient was gradually weaned off the ventilator. On 5-year follow-up, he is completely healthy, leads an active lifestyle, and has had no further bleeding.
Case 2
A 2-year-old boy, diagnosed with relapsed ALL, was referred for treatment from another hospital. He was diagnosed 1 year earlier, received treatment, and was considered in remission. Three weeks prior to his referral, he was diagnosed with bone marrow relapse. In the absence of treatment to be offered locally, he was started on systemic steroids and transferred to our institution for further management.
Shortly following arrival, he presented to the Emergency Department with fever and epistaxis. Laboratory work-up revealed extreme leukocytosis, severe thrombocytopenia, and anemia. Initial chest X-ray revealed clear lung fields. He was admitted for initiation of treatment and blood transfusion, as well as management of possible tumor lysis syndrome.
His admission was complicated by respiratory failure requiring intubation and mechanical ventilation. Suctioning of the endotreacheal tube revealed a steady bloody aspirate coinciding with rapidly progressive diffuse patchy infiltrates bilaterally on radiography. Pulmonary hemorrhage was diagnosed, which did not respond to correction of thrombocytopenia and high-dose steroids. He received packed red blood cell transfusion in small boluses to avoid hyperviscosity and fluid overload. Additionally leukopheresis was undertaken to reduce leukocyte load.
Given the persistence of high-pressure ventilatory support and the nonremitting bleeding, a bronchoscopy was performed, which revealed a persistent bloody return on bronchoalveolar lavage from both lungs, consistent with DAH. Therefore, administration of rFVIIa was undertaken. As above, a similar dose of rFVIIa (50 μg/kg) was administered. However, considering the young age and weight of the patient, the dilution was in a smaller volume of 25 mL normal saline. The rFVIIa solution was divided equally and instilled into both main stem bronchi. Apart from a transient hypoxia, the procedure was well tolerated, and the bleeding ceased.
Following the procedure, no further bleeding was noted. Ventilatory support was weaned, and he was successfully extubated in short sequence and no adverse effects were noted. Radiologic improvement of the patchy infiltrates was noted 2 days after rFVIIa instillation with progression to clear lungs.
He continued chemotherapeutic treatment for ALL, with a favorable response and no respiratory issues. However, his treatment course was complicated by a persistent systemic fungal infection (Fusarium sp.) with a paraspinal abscess, which resulted in his demise.
Discussion
We report the successful treatment of leukemia-related DAH with rFVIIa in two children. In both cases, the treatment was a last-resort intervention for nonremitting bleeding that did not respond to conventional therapies.
DAH has been observed as a severe complication in patients on chemotherapy, after hematopoietic stem cell transplantation, and in a variety of autoimmune disorders. 4
The efficacy of systemic use of rFVIIa has been demonstrated in hemophilia with antibodies to factor VIII and IX and as a promising agent in a wide range of hemorrhagic conditions, including trauma, surgery, obstetric bleeding, reversal of oral anticoagulation, reversal of heparin, lepirudin, fondaprinux, thrombocytopenia, thrombocytopathy, bleeding with impaired liver function, and gastrointestinal bleeding. 5 Its systemic use was first reported in pulmonary hemorrhage in an unstable patient without coagulopathy in whom conventional treatment was not immediately available 6 and subsequently expanded to other conditions with refractory pulmonary bleeding.7,8 It should be noted, however, that a 2012 Cochrane Review concluded that the clinical value of intravenous rFVIIa for uncontrollable bleeding in patients without hemophilia is unproven. 9
The rationale for direct instillation of rFVIIa into the lung is based on the previous observations of systemic use. Heslet et al. 3 described six consecutive adult patients with pulmonary bleeding who were not responding to conventional therapy (including high-dose intravenous instillation of rFVII in one case). The efficacy was demonstrated in all patients after a 50 μg/kg dose via bronchoscopic instillation. No adverse effects were demonstrated. They concluded that the intervention had a significant hemostatic effect for a disease with high mortality and no documented specific intervention. Similarly, Estella et al. presented two adult patients with massive hemoptysis in whom the pulmonary route of administration was preferred; one patient had concomitant renal failure with recent arteriovenous fistula intervention, and the other had acute myocardial infarction. Local administration of rFVII was used as an emergency measure with excellent results and no adverse effects. 2 A recent additional reported case of a 60-year-old patient in whom FVIIa was successfully used for pulmonary bleeding suspected as being due to systemic disease (Wegener's granulomatosis, systemic lupus erythmatosus (SLE), or Goodpasture's syndrome). 10
We have briefly reported case 1 previously as the only pediatric case of a successful treatment via direct airway instillation of rFVIIa that we could find in our literature review. 1
The pathophysiologic background of the intervention may be related to the presence of tissue factor (TF) in the alveolus and receptors on the air side of the lung, a theory that has been known for many years. Rose et al. demonstrated that in the case of granulocyte macrophage colony stimulating factor (GM-CSF), the inhaled route was needed in order to reach the receptor on the air side, resulting in increased numbers of alveolar macrophages, whereas intravenous administration of the drug had no effect on macrophage numbers. In addition, the inhaled route did not affect systemic monocytes.4,11
The cell-based model of coagulation5,12 supports the concept that rFVIIa enhances hemostasis at the site of injury, binding to either TF or activated platelets at the site of damage without a systemic, hypercoagulable state (Fig. 1). Homeostasis is divided into three phases—initiation, amplification, and propagation—with the endpoint leading to generation of large amounts of thrombin: so-called thrombin burst. The thrombin converts fibrinogen to fibrin. High concentrations of VIIa, which are achieved only by pharmacologic doses of rFVIIa, bypass the need for VIIIa or IXa by directly converting X to Xa on the activated platelet, resulting in a thrombin burst, 13 hence the potential utility of rFVIIa in patients with coagulation defects.
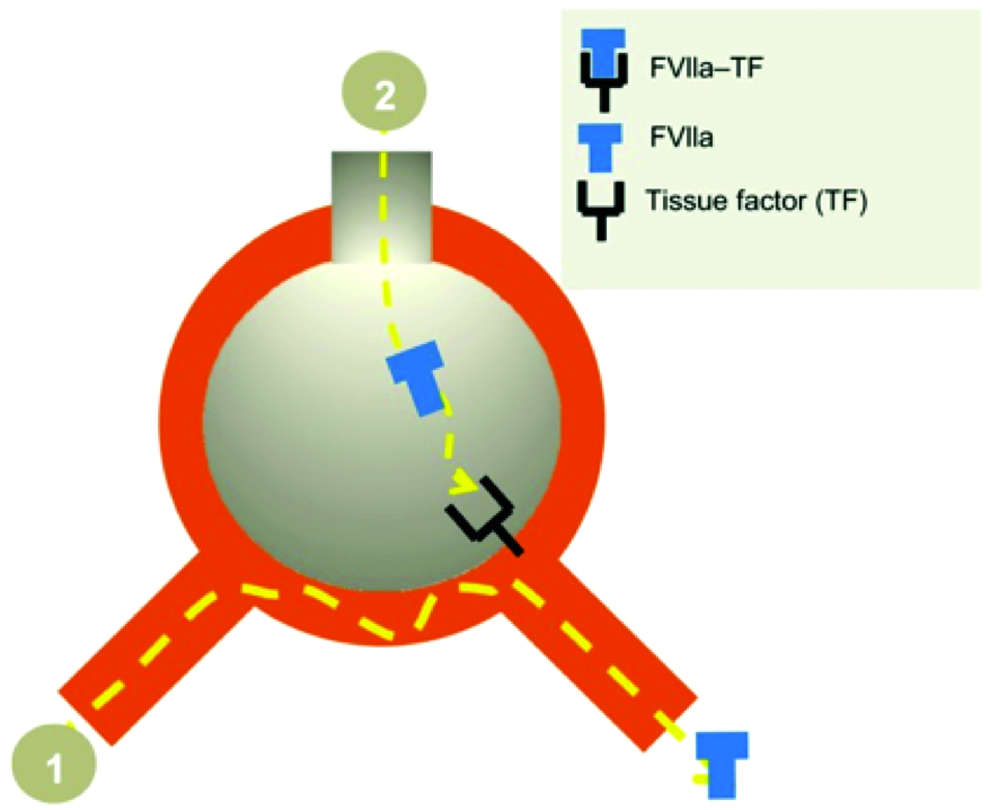
Suggested mode of action of intra-alveolar human recombinant activated factor VII (rFVIIa) in diffuse alveolar hemorrhage (DAH) where sufficient concentration is not achieved with the intravenous FVIIa (1) (since the molecular weight of FVIIa does not permit passage to the alveoli space) compared to the airway route (2) where a direct access to the receptor tissue factor (TF) is obtained. Eventually, the activated FVIIa-TF complex induces hemostasis (Heslet et al. Biologics 2012; 6:37–46). Color images available online at www.liebertpub.com/ped
During inflammatory pulmonary conditions such as pneumonia or ARDS, a high concentration of alveolar tissue factor is present and plays a central role in initiating hemostasis. However, tissue factor pathway inhibitor (TFPI) is also produced in lung injury and likely counteracts this hemostatic effect. This report further supports the notion that intrapulmonary administration of rFVIIa can activate a local coagulation pathway in the lung and counteract TFPI-induced anticoagulation. This therapeutic effect of rFVIIa occurs at concentrations that are 10-fold higher than the physiologic concentrations of endogenous factor VII. Beyond this high topical concentration element, direct instillation offers an advantage over systemically administered factor preparations such as fresh frozen plasma or factor VIII that can cause fluid overload as well as time delays. Ultimately, the key advantage of pulmonary administration of rFVIIa may be that it bypasses the risk of thrombotic complications in other systems, which have been reported in intravenous administration of rFVIIa. 14
Alten et al. reported the association of the off-label use of systemic rFVIIa with thromboembolic events in children. 15 This experience was further expanded by a multi-cohort study describing the increase of off-label use of systemic rFVIIa in hospitalized children, despite the absence of adequate clinical trials demonstrating its safety and efficacy with an increased thrombotic events and mortality. 16
The present report documents the successful treatment of two children with DAH who were treated with bronchoscopic instillation of rFVIIa with immediate and unequivocal results in both and without evidence of significant adverse effects. The ease of administration and rapid symptomatic response makes this an attractive option, particularly when confronted with the steep increase off-label systemic use of rFVIIa, which is expensive, carries potential severe side effects, and is often unsuccessful.15,16 The addition of these cases to the pediatric literature further supports the use of bronchoscopic instillation of rFVIIa as a viable and potentially lifesaving alternative to other more traditional supportive approaches.
Footnotes
Author Disclosure Statement
No competing financial interests exist.